
We use cookies to ensure our website works properly and to personalise your experience. Cookies policy
M.A.M College of Pharmacy
Recent advances in the clinical assessment and management of neonatal hyperbilirubinemia have significantly improved the early identification of infants at risk for severe jaundice and bilirubin-induced neurotoxicity. Key developments include the implementation of universal predischarge bilirubin screening during birth hospitalization, which facilitates early detection and timely intervention. Increasing evidence has also confirmed that hemolysis is a major risk factor for bilirubin neurotoxicity, emphasizing the importance of careful monitoring in affected neonates. In addition, the introduction of standardized numeric scoring systems has enhanced the clinical staging and assessment of acute bilirubin encephalopathy. Therapeutic innovations such as turquoise-light phototherapy have shown potential advantages over conventional phototherapy by improving bilirubin reduction efficiency. Furthermore, emerging therapies, including heme-oxygenase inhibitors, may help reduce bilirubin production and decrease the need for exchange transfusions in severe cases. These advancements collectively contribute to safer, more effective strategies for the prevention and treatment of neonatal hyperbilirubinemia.
Neonatal hyperbilirubinemia is the most common clinical condition in newborns requiring evaluation and management and remains a leading cause of hospital readmission during the first week of life. The high prevalence of neonatal hyperbilirubinemia is primarily due to developmental immaturity of red blood cell turnover, hepatic function, and gastrointestinal bilirubin clearance mechanisms, which together create an imbalance favoring bilirubin production over elimination. In most neonates, hyperbilirubinemia represents a benign transitional phenomenon with no significant clinical consequences. However, a subset of infants develops clinically significant elevations in bilirubin levels that may progress to severe complications if not recognized and treated promptly. The estimated incidence of hyperbilirubinemia according to peak total serum bilirubin (TSB) levels is approximately 1 in 10 infants for significant hyperbilirubinemia (>17 mg/dL or 291 μmol/L), 1 in 70 for severe hyperbilirubinemia (>20 mg/dL or 342 μmol/L), 1 in 700 for extreme hyperbilirubinemia (>25 mg/dL or 428 μmol/L), and 1 in 10,000 live births for hazardous hyperbilirubinemia (>30 mg/dL or 513 μmol/L). Because excessive bilirubin accumulation can lead to acute bilirubin encephalopathy and kernicterus, timely identification of at-risk neonates and appropriate management strategies are essential to reduce morbidity and mortality associated with this condition. Despite the implementation of evaluation and treatment guidelines for neonatal hyperbilirubinemia by the American Academy of Pediatrics (AAP). and others to “reduce the incidence of severe hyperbilirubinemia and bilirubin encephalopathy, ” cases of kernicterus are still occurring in the United States, Canada, Europe, and elsewhere.!’ In developed countries, population-based estimates for kernicterus in term infants range from I in 30, 000 to I in 200.000 live births. The current review focuses on recent advances in our approach to risk assessment for the development of severe hyperbilirubinemia and bilirubin neurotoxicity, as well as treatment measures to control hyperbilirubinemia in newborns. The crux of hyperbilirubinemia and bilirubin- induced neurotoxicity risk evaluation remains the measurement of total serum bilirubin interpreted in an hour-specific fashion, 718 and the mainstays of intervention are photo-therapy and exchange transfusion.920 These are detailed, along with other evaluation strategies, clinical tools, and adjunctive therapies, including several currently under study that hold promise for potential future application to the management of neonatal jaundice.
Universal predischarge birth hospitalization bilirubin screening:
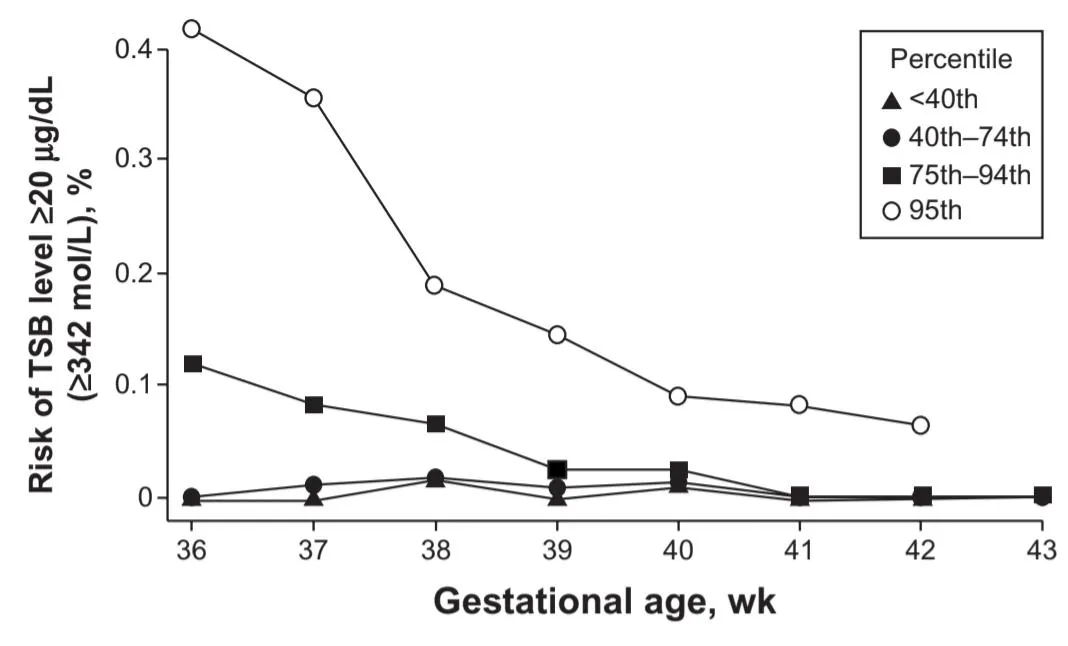
The 2009 update of the American Academy of Pediatrics (AAP) guideline recommended universal bilirubin screening before newborn discharge using total serum bilirubin (TSB) or transcutaneous bilirubin (TcB). This helps identify infants at risk for severe hyperbilirubinemia, especially when combined with gestational age assessment. Studies show that routine screening significantly reduces cases of hazardous bilirubin levels. TcB is a noninvasive screening method that estimates bilirubin through skin color measurement. Since TcB may underestimate high bilirubin levels, especially above 13 mg/dL, confirmatory TSB testing is recommended when TcB readings are elevated.
Neurotoxicity risk factors:
The major determinants of bilirubin neurotoxicity currently used in clinical practice are:
* Total serum bilirubin (TSB) level
* Gestational age of the newborn
* Presence of neurotoxicity risk factors
Neurotoxicity risk factors are clinical conditions that increase the likelihood of bilirubin-induced brain injury in infants with severe hyperbilirubinemia. According to the 2004 American Academy of Pediatrics guideline, these include:
* Isoimmune hemolytic disease
* Glucose-6-phosphate dehydrogenase (G6PD) deficiency
* Asphyxia
* Sepsis
* Acidosis
* Serum albumin level <3.0 g/dL
These factors are considered together with the infant’s gestational age and hour-specific TSB levels to determine the thresholds for phototherapy and exchange transfusion. When any neurotoxicity risk factor is present, treatment is recommended at lower TSB levels because of the increased risk of bilirubin neurotoxicity.
TSB and neurotoxicity risk:
TSB is the measure of albumin-bound bilirubin, whereas the small circulating fraction not bound to albumin or other serum proteins is indexed by the unbound or “free” (Bf) bilirubin level. The latter is in dynamic equilibrium with the extravascular tissues, including the central nervous system, and provides a measure of the relative amount of bilirubin that will exit the vascular space at a given level of TSB. TSB alone is of limited value in predicting neurologic impairment and kernicterus in hyperbilirubinemic newborns, a conclusion reaffirmed in recent clinical studies. Nevertheless, it is clear that marked elevations in TSB are associated with kernicterus risk, and TSB remains for all intents and purposes the only biochemical measurement of bilirubin widely available to clinicians. There continues to be a keen interest in Bf, the bilirubin-albumin (B/A) ratio as a proxy of Bf, and the Bf/TSB ratio as potential more reliable indices of neurotoxicity risk than the TSB. At this time, however, no commercial instrument is available to measure Bf, although a newly developed fluorescence sensor for quantifying Bf in plasma has been detailed and applied in research reports. This novel methodology is less complex than the previously studied horseradish peroxidase method, requires only a small sample volume, and therefore holds promise for clinical application in the future. In the interim, the most frequently used proxy for Bf is the ratio of TSB (mg/dL) to serum albumin (g/dL), an index that correlates with measured circulating Bf. Use of the B/A ratio has been endorsed by the AAP in determining the need for exchange transfusion, albeit in conjunction with, but not in lieu of, the TSB. Evidence from the recent prospective randomized multi center Bilirubin Albumin Ratio Trial (BART) in The Netherlands, however, showed that the neurodevelopmental outcome of preterm infants treated according to the B/A ratio or TSB (whichever was exceeded first) was not superior to those treated according to the TSB threshold alone. Although this study may have been underpowered (only 30% of infants in the experimental group were treated on the basis of the B/A ratio, as opposed to TSB), it is also possible that B/A ratios selected for study lacked sensitivity and that a lower B/A ratio than those used for intervention in the BART might better index neurotoxicity risk. Indeed, preliminary data from Japan suggest that lower B/A ratios may be more sensitive to unbound bilirubin levels in the putative neurotoxic range, and to bilirubin-induced abnormalities on brainstem auditory evoked responses, particularly in preterm neonates. For Example, in infants of less than 30 weeks’ gestational age, A B/A molar ratio of 0.40 (equivalent to B/A of 3.4 mg/g) Was predictive of a Bf of more than 1 µg/dL and abnormal Brainstem auditory evoked responses, with 100% sensitivity And 85% specificity. In contrast to these, Iskander et al were Unable to show improved sensitivity in predicting ABE, CBE, And hearing loss risk using B/A as compared with TSB in a Large cohort of infants with TSB levels higher than 25 mg/dL in Cairo. In fact, only a B/A molar ratio of 1:1 or greater (B/A ratio of $8.6 mg/g) was revelatory of ABE risk. The Nature of the differences across these studies merit clarification to determine the potential utility of B/A as aproxy of Bf and a predictor of neurotoxicity risk. Should Bf measurements become clinically available, it will Be important to remember that Bf and TSB are not competing Independent determinants of bilirubin toxicity but, rather, critically interrelated and interdependent factors in estimating risk, a Point highlighted by Ahlfors et al in several publications. TSB is needed to gauge the size of the bilirubin load, and Bf its Distribution. Ahlfors et al therefore suggest that the Bf-to-TSB Ratio may be the best risk predictor of all . It will Be of interest to study this possibility in a larger cohort once Bf Measurements are available in the clinical arena. An alternative or complementary approach to Bf and the Bf/TSB ratio in predicting bilirubin-induced neurotoxicity is the Bilirubin binding capacity (BBC), using hematofluorometry. The latter index provides a measure of the neonate’s capacity to Handle a bilirubin load. BBC encompasses both the albumin Level and the nuances of albumin–bilirubin binding, which can Be affected by several clinical conditions, including gestational Age. Interest in the BBC has been rekindled by the development of a point-of-care hematofluorometric device now being Trialed in the clinical arena. Collectively, these observations show that much work Remains to be done in effectively applying bilirubin measurements (TSB, Bf, Bf/TSB, BBC) to identify infants at Neurotoxicity risk. In theory, we should be able to do better Than TSB alone, but in clinical reality, that is not yet the Case. Finally, although Bf has biologic effects in the brain, The Bf level alone is not likely to dictate the risk for bilirubin Encephalopathy. Bilirubin-induced neurotoxicity depends On a complex interaction between the level and duration of CNS Bf exposure and the innate cellular characteristics of The developing CNS that may predispose or protect against Bilirubin-induced neuronal injury.
Hemolysis and neurotoxicity risk:
The clinical impression that hemolysis potentiates bilirubin neurotoxicity in neonates is long-standing and dates back to the early work on Rh isoimmunization and the first reports correlating increasing TSB and the risk for bilirubin encephalopathy. Hemolytic conditions remain prevalent contributors to both hyperbilirubinemia and bilirubin neurotoxicity risk. They encompass immune-mediated hemolytic disorders (Rhesus, non-Rhesus, and ABO hemolytic disease), red cell enzyme defects (G6PD, pyruvate kinase deficiencies), and red cell membrane abnormalities (hereditary spherocytosis, elliptocytosis, and others), as well as some unstable hemoglobin’s. Although the mechanism or mechanisms underlying the neurotoxicity-intensifying effect is unclear, recent data provide strong corroboration that hemolysis augments bilirubin neurotoxicity in neonates, with Rh hemolytic disease and G6PD deficiency playing particularly prominent etiologic roles. More specifically, Gamaleldin et al showed that the TSB threshold for identifying 90% of babies with bilirubin encephalopathy was 25.4 mg/dL (434 µmol/L) in infants with neurotoxicity risk factors (primarily hemolytic disorders) in contrast to 31.5 mg/dL (539 µmole/L) in those without. The presence of Rh hemolytic disease alone greatly increased the risk for bilirubin encephalopathy (odds ratio, 48.6; 95% confidence interval, 14–168). Of concern, it is increasingly apparent that the diagnosis of hemolysis in neonates remains problematic and, as a result, under recognized. Several reports demonstrate that the etiology of extreme or hazardous hyperbilirubinemia is often unclear and not identified, when almost assuredly a hemolytic process is an important contributor to their genesis in many, if not most, cases. Indeed, Christensen et al recently reported that when an exhaustive search, including “next-generation” sequencing of a panel of gene variants involved in neonatal hyperbilirubinemia, was performed, a specific diagnosis was made in all infants with extreme hyperbilirubinemia (TSB .25 mg/dL) and was explained by an underlying hemolytic condition in each instance. These data suggest that clinical indices to detect accelerated red blood cell turnover may be useful adjuncts in identifying neonates with hemolysis. The approach that has received the most attention in this regard is the measurement of end-tidal carbon monoxide (ETCO) corrected for ambient CO or ETCOc. The catabolism of heme derived from red cell hemoglobin produces equimolar amounts of CO and bilirubin, providing the physiologic basis for ETCOc to index hemolysis. Previous studies have demonstrated that elevated levels of ETCOc correlate with blood carboxyhemoglobin concentrations. Recent studies have detailed measurements of ETCOc levels in neonates and are nicely summarized in a succinct review by Tidmarsh and colleagues. Collectively, they suggest an ETCOc cutoff of more than 2.5 parts per million to predict the presence of clinically significant hemolysis. Although no commercial ETCOc device is currently available, one is in development and undergoing preliminary testing. Such an instrument holds potential for point-of-care application in helping identify neonates with hemolysis once normative data are first established. One can envision the measurement of ETCOc as an adjunct in helping to identify infants at risk for subsequent severe hyperbilirubinemia and in further stratifying treatment criteria.
Identifying neonates with Intermediate to advanced ABE:
ABE defines an encephalopathic state induced by hazardous hyperbilirubinemia during the first days of postnatal life and is characterized by a constellation of abnormal clinical signs typically progressive in their severity. In term ($370/7 weeks’ Gestation) and late preterm (340/7–366/7 weeks’ gestation) Infants, the initial phase of ABE is characterized by stupor (lethargy), hypotonia, and poor sucking. These nonspecific signs are seen in numerous clinical contexts, but in a hyperbilirubinemic infant, they should raise the possibility of early ABE. Clinical signs of intermediate to advanced stages of ABE are increasingly more specific to bilirubin-induced neurotoxicity and herald a marked increased risk for permanent injury. These include hypertonia, often manifested by Retrocollis, and opisthotonus, fever, and high-pitched cry. Inability to feed and apnea may ensue. There is growing evidence that bilirubin-induced neurotoxicity resulting in brainstem injury may manifest clinically as symptomatic apneic events and presage intermediate to advanced stages of ABE. Infants younger than 34 weeks’ gestation less frequently show these classic abnormal neuromotor signs. Recurrent apnea and desaturations may be the only clinical manifestations of ABE in preterm infants during the neonatal period, if any appear at all. In contrast, CBE defines the permanent clinical sequelae of bilirubin toxicity that become evident in the first year of life and is synonymous with kernicterus. Recently, a numeric scoring system for quantifying the degree of ABE has been outlined; it is detailed in Table 1. This scoring system of bilirubin-induced neurologic dysfunction may prove to be a useful clinical tool in identifying Infants with intermediate to advanced ABE, conditions that pose significant risk for CBE and are an indication for the urgent application of bilirubin reduction strategies. Indeed, preliminary observations suggest this numeric approach may be quite reliable in characterizing the severity of ABE and may prove helpful in managing infants with hazardous hyperbilirubinemia. Notably, as detailed in the section on exchange transfusion, the AAP recommends immediate exchange transfusion in any infant who is jaundiced and manifests signs of intermediate to advanced stages of ABE (hypertonia, arching, retrocollis, opisthotonos, fever, high pitched cry), even if the TSB is falling.
Table 1: Clinical bilirubin-induced neurological dysfunction (BIND) score of onset, severity, and progression of acute bilirubin encephalopathy, as elicited by history and physical examination.
|
Clinical signs Bilirubin-induced Acute bilirubin neurological encephalopathy dysfunction score Mental status Normal 0 none Sleepy but able to be arouse: decreased feeding 1 subtle Lethargy, poor suck,and irritable with strong suck 2 moderate Semi coma, apnea, unable to feed, seizures, coma 3 Advanced Muscle tone Normal 0 none Persistent mild to moderate hypertonia alternating with hypotonia 1 subtle Mild to moderate hypertonia alternating with hypertonia, 2 moderate beginning arching to neck and trunk on stimulation Persistent retrocollis and opisthotonos, bicycling of 3 Advanced hands and feet Cry pattern Normal 0 none High-pitched when aroused 1 subtle Shrill, difficult to console 2 moderate Inconsolable crying 3 Advanced Total BIND(acute bilirubin encephalopathy score) |
Photography:
Phototherapy is the mainstay of hyperbilirubinemia treatment in neonates across the gestational age spectrum. In widespread application since the 1970s, phototherapy has resulted in a marked reduction in the need to perform exchange transfusions to prevent hazardous hyperbilirubinemia and bilirubin encephalopathy. The effectiveness of phototherapy is Determined by the irradiance, the surface area of exposure, and the light spectrum used. Irradiance is the radiant power, and the irradiance in a specific wavelength band is termed the spectral irradiance and is expressed as micro-Watts per centimeter squared per Nanometer. There is a direct dose–response relationship between the efficacy of phototherapy and the irradiance used, and the level of irradiance is related to the distance between the light and the infant. In contrast to the early data from Tan, Vandborg et al recently demonstrated a linear relationship between irradiance and the decrease in the TSB with no evidence of a saturation point. The surface area of the infant exposed to phototherapy and the spectrum of light delivered are also key elements in determining the efficacy of phototherapy. The spectrum of light delivered by the phototherapy unit is determined by the type of light source and any filters used. Unconjugated bilirubin absorbs light most strongly in the blue region of the spectrum, near 460 nm, and the penetration of tissue by light increases with increasing wavelength. Only wavelengths that penetrate tissue and are absorbed by bilirubin have a phototherapeutic effect. Recently, Lamola et al detailed the important effect hematocrit has on the efficacy of phototherapy for neonatal jaundice. More specifically, they calculated that the wavelength at which the highest fraction of light is absorbed by bilirubin across a range of hematocrits Peaked at 476 nm, not 460 nm. On the basis of this previously unrecognized hematocrit effect, they speculate that narrow-band light-emitting diode phototherapy at 476 nm would be 60% more effective than blue fluorescent lamps, a conclusion consistent with observations that blue-green (turquoise) light with emission peak at 490 nm and bandwidth of 65 nm is more effective than blue light.66,67 Others, however, have observed no difference between turquoise and blue light Phototherapy effectiveness. Further study is necessary to clarify the potential advantage of turquoise phototherapy. The benefit of timely phototherapy application in infants who show marked, potentially hazardous hyperbilirubinemia is clear and highlighted by the work of Mreihil et al, who report that configurational photo isomerization of bilirubin occurs almost instantaneously and is detectable in appreciable amounts in the blood of newborns within 15 minutes of initiating intensive phototherapy. These photo isomers can account for up to 20%–30% of the total unconjugated bilirubin and are less lipophilic than native bilirubin, and therefore are less likely to cross the blood–brain barrier. So the immediate detoxification of some bilirubin, even before it is excreted, is a possible additional benefit of phototherapy. Clearance of the structural photo isomer lumirubin is felt to be primarily responsible for the ultimate bilirubin-lowering effect of Phototherapy, although the actual contributions of individual isomers remain uncertain. Photo oxidation of bilirubin is a slow process and a minor contributor to the elimination of bilirubin during phototherapy.
Exchange transfusion :
Exchange transfusion remains an important, if infrequently required, clinical intervention to prevent or reduce the risk for kernicterus. The prevention of Rh (D) hemolytic disease with Rh (D) immunoglobulin and the more effective use of intensive phototherapy have led to a dramatic decline in the number of exchange transfusions performed. Although there is little new to report on exchange transfusion per se, it is important to highlight a few clinical issues that remain relevant to its effective use.
To what hematocrit should the donor blood be reconstituted for exchange transfusion? Given that bilirubin is bound to albumin in the vascular compartment, the efficacy of a double-volume exchange Transfusion is a function of the plasma volume, and most Important, the mass of albumin exchanged. It follows that donor blood of high plasma volume, that is, low hematocrit (∼40%), to enhance the amount of bilirubin free albumin introduced into the infant’s circulation during exchange is preferred. Surprisingly, this fundamental aspect of performing an exchange transfusion is not consistently highlighted in current reviews or textbook recommendations.
Exchange transfusion in intermediate to advanced stages of ABE: The 2004 AAP statement on hyperbilirubinemia specifies that “immediate exchange transfusion is recommended in any infant who is jaundiced and manifests signs of intermediate to advanced stages of acute bilirubin encephalopathy (hypertonia, arching, retrocollis, opisthotonos, fever, high-pitched cry) even if the TSB is falling.” This recommendation is consistent with reports that at least some infants so treated may escape unscathed without chronic bilirubin encephalopathy (kernicterus) and with earlier observations that a decline in TSB coincident with the clinical onset of intermediate to advanced signs of ABE can occur and is often a prognostic sign for poor outcome, as opposed to a sign of clinical improvement.
Pharmacological treatment:
Intravenous immunoglobulin:
Early studies and a systematic review suggested that the administration of intravenous immunoglobulin (IVIG) to infants with Rh hemolytic disease would significantly reduce the need for exchange transfusion. Two recent randomized controlled trials, however, showed no benefit from the administration of IVIG to newborns with Rh hemolytic disease, and a Cochrane meta-analysis86 concluded that the efficacy of IVIG was not conclusive in Rh or ABO hemolytic disease of the newborn. The mechanism of action of IVIG is unknown, But it is possible that it might alter the course of immune mediated hemolytic disease by blocking Fc receptors, thereby inhibiting hemolysis. The 2004 AAP guideline reserves the use of IVIG to direct Coombs-positive infants whose TSB continues to rise despite intensive phototherapy or whose TSB is within 2–3 mg/dL of the exchange level.
Heme oxygenase inhibitors:
The rate-limiting step in bilirubin production is the conversion of heme to biliverdin by heme oxygenase. Certain Synthetic metalloporphyrins are powerful competitive inhibitors of heme oxygenase and suppress the formation of bilirubin. One such compound that has been studied extensively is tin mesoporphyrin (SnMP). A series of controlled clinical trials have demonstrated that SnMP is a potent inhibitor of heme oxygenase and is highly effective in reducing TSB levels and the requirements for phototherapy in term and preterm neonates. The only reported adverse effect has been a transient erythema that disappeared without sequelae in infants who received white light phototherapy after SnMP administration. This drug is still awaiting approval by the US Food and Drug Administration, although it can be obtained for compassionate use (InfaCare Pharmaceutical Corp, Trevose, PA, USA). If approved, SnMP could find immediate application in preventing the need for exchange transfusion in infants who are not responding to phototherapy. Other Metalloporphyrins formulations are currently under study that hold the additional promise of being orally bioavailable and nonphotosensitizing.
CONCLUSION
Neonatal hyperbilirubinemia remains one of the most common clinical conditions encountered during the neonatal period, affecting a significant proportion of both term and preterm infants. Over the years, substantial advances in understanding bilirubin metabolism, risk factors, and disease progression have led to the development of effective and evidence-based treatment strategies. Current management focuses on early identification through universal bilirubin screening, careful clinical assessment, and risk stratification based on gestational age, postnatal age, and the presence of underlying conditions such as hemolytic disease or prematurity. Phototherapy continues to be the cornerstone of treatment due to its proven safety, effectiveness, noninvasive nature, and ability to rapidly reduce serum bilirubin levels, thereby preventing the progression to severe hyperbilirubinemia. In cases where bilirubin levels rise to dangerous thresholds or fail to respond adequately to phototherapy, exchange transfusion remains a lifesaving intervention, while adjunctive therapies such as intravenous immunoglobulin may be beneficial in selected infants with immune-mediated hemolysis. Improvements in clinical guidelines, standardized treatment thresholds, and advances in neonatal care have significantly reduced the incidence of bilirubin-induced neurological dysfunction and kernicterus. Furthermore, the promotion of adequate breastfeeding, parental education regarding jaundice recognition, and timely post-discharge follow-up have enhanced the overall effectiveness of treatment and prevention strategies.
REFERENCES
Amsterdam: Harwood Academic Publishers; 2000:75–88.


M. Prasada Rao*, Y. Narasimha Rao, S. Rajini, B. Satwika, Clinical Review Of Current Approaches In The Management Of Neonatal Hyperbilirubinemia, Int. J. Sci. R. Tech., 2026, 3 (6), 400-408. https://doi.org/10.5281/zenodo.20557391
 10.5281/zenodo.20557391
10.5281/zenodo.20557391