
We use cookies to ensure our website works properly and to personalise your experience. Cookies policy
Base Research and Consultancy Group (BRCG), New Delhi, India
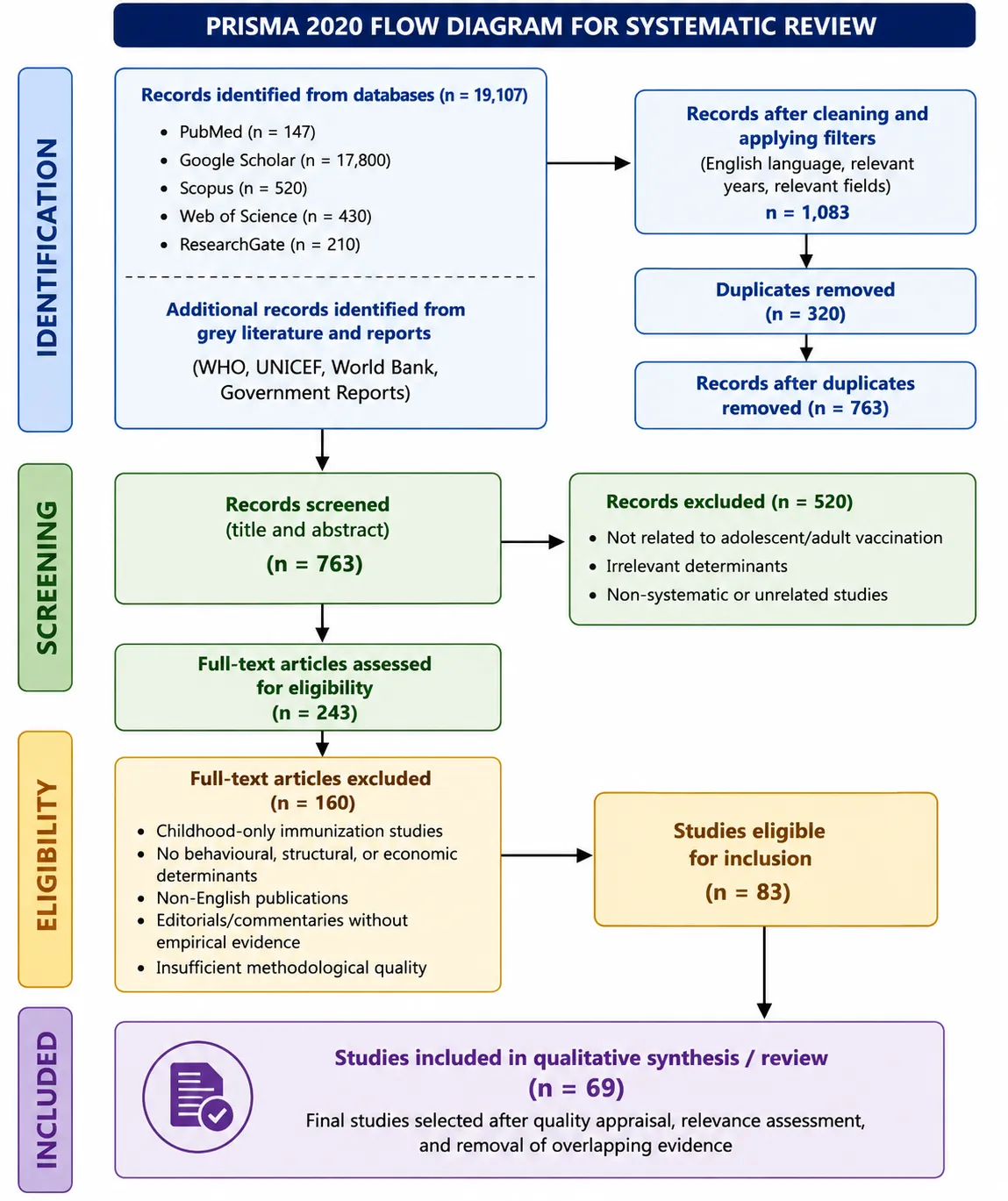
Background: Vaccination is one of the most successful public health interventions, preventing an estimated 2–3 million deaths annually. However, despite high childhood immunization coverage globally, vaccination rates among adolescents and adults remain suboptimal, leaving significant populations vulnerable to vaccine-preventable diseases such as influenza, HPV, tetanus, pertussis, and pneumococcal disease. The COVID-19 pandemic further exposed these gaps, with adolescent and adult uptake lagging routine childhood programmes. Aim: To systematically synthesise existing evidence on the behavioural, structural, and economic determinants influencing vaccination uptake among adolescents (aged 10–19 years) and adults (aged ?20 years), and to provide evidence-based recommendations for improving vaccine acceptance, accessibility, and equity across the life course. Methods: A systematic literature review was conducted in accordance with PRISMA guidelines. A comprehensive search was performed across PubMed, Scopus, Web of Science, and Google Scholar, supplemented by grey literature from WHO, UNICEF, and the World Bank. Studies published between 2009 and 2024, in English, focusing on determinants of vaccination uptake among adolescents and adults, were included. Thematic analysis was employed to classify determinants into behavioural, structural, and economic domains. Results: A synthesis of 46 studies revealed three major determinant categories. Behavioural barriers included vaccine hesitancy, low perceived risk, religious beliefs, lack of knowledge, safety concerns, and parental attitudes. Structural barriers comprised geographic disparities, school-based logistical challenges, exclusion of migrant and homeless populations, fragmented data systems, and limited provider access. Economic barriers involved household income, out-of-pocket costs, transportation expenses, and indirect wage losses. Multi-component interventions addressing multiple domains simultaneously demonstrated the largest coverage improvements (median +19 to +22 percentage points), outperforming single-domain interventions such as reminders alone (+9–12%). Effective strategies included SMS reminders, provider announcement training, school-based consent streamlining, community-based outreach, removal of out-of-pocket costs plus transport reimbursement, and pharmacist-delivered vaccination. Conclusion: Vaccination uptake among adolescents and adults is shaped by a complex interplay of behavioural, structural, and economic determinants. Achieving high and equitable coverage requires integrated, multi-component strategies that address all three domains in parallel. Policymakers should prioritise removal of financial barriers, expansion of delivery sites, strengthening of immunisation information systems, and targeted outreach to migrant, homeless, and rural populations. Healthcare providers should adopt presumptive announcement styles and integrate vaccination into routine care. Future research should focus on randomised controlled trials of structural interventions, standardised measurement tools, and implementation science to guide scale-up and sustainability.
Vaccination stands as one of the most successful and cost-effective public health interventions in modern history, preventing an estimated 2–3 million deaths annually and dramatically reducing the global burden of infectious diseases(1). Despite remarkable progress in childhood immunization programmes worldwide, vaccination coverage among adolescents and adults remains persistently suboptimal in many regions, leaving significant portions of the population vulnerable to vaccine-preventable diseases such as influenza, human papillomavirus (HPV), tetanus, diphtheria, pertussis, pneumococcal disease, and herpes zoster(1) .
The COVID-19 pandemic starkly illuminated these gaps, as vaccine uptake varied dramatically across age groups and geographic regions, with adolescents and adults exhibiting lower vaccination rates compared to routine childhood immunization programmes(2). Recent data from the World Health Organization indicate that while global childhood vaccination coverage has stabilized at approximately 81% for the third dose of diphtheria-tetanus-pertussis (DTP3) vaccine, coverage for adolescent and adult vaccines such as HPV (complete series) remains below 15% in many low- and middle-income countries, and seasonal influenza vaccination among high-risk adults rarely exceeds 50% even in high-income settings(1,3).
Understanding why adolescents and adults fail to receive recommended vaccines requires examination of multiple interconnected determinants. Behavioural factors—including vaccine hesitancy, exposure to misinformation, fear of adverse effects, low perceived susceptibility to vaccine-preventable diseases, and mistrust in healthcare systems—have been consistently identified as significant barriers to vaccination(4,5). Social and psychological influences, such as community norms, cultural beliefs, and the rapid proliferation of anti-vaccine content through digital media platforms, further erode vaccine confidence(6,7). Structural barriers, including inadequate healthcare infrastructure, limited vaccine supply chain capacity, geographic disparities in service access, inconvenient clinic hours, and fragmented immunization registries, continue to impede uptake, particularly among rural, migrant, and marginalised populations(2,8). Economic constraints—comprising direct vaccine costs, consultation fees, transportation expenses, and indirect losses such as wages forfeited during healthcare visits—disproportionately affect low-income groups and contribute to persistent inequities in vaccination coverage across the life course(9).
The COVID-19 pandemic exacerbated these challenges, disrupting routine immunization services in at least 68 countries and leaving an estimated 23 million children and countless adolescents and adults without scheduled vaccines in 2020 alone(2). This disruption has reinforced the urgent need for robust, evidence-based life-course immunization strategies that address the full spectrum of behavioural, structural, and economic determinants.
Therefore, this review aims to systematically synthesise existing evidence on the behavioural, structural, and economic determinants influencing vaccination uptake among adolescents and adults, and to provide evidence-based recommendations for improving vaccine acceptance, accessibility, and equity(10).
Key Data
|
Domain |
Key Finding |
Source |
|
Global childhood vaccine coverage |
81% for DTP3 (third dose) |
WHO (2022) |
|
HPV vaccine completion (LMICs) |
<15% for full series |
WHO (2022) |
|
Seasonal influenza coverage (high-risk adults) |
≤50% in high-income settings |
ECDC (2021) |
|
Routine immunization disruptions (2020) |
68 countries affected |
UNICEF (2023) |
|
Missed vaccinations during COVID-19 |
~23 million individuals (all ages) |
UNICEF (2023) |
|
Annual deaths prevented by vaccination |
2–3 million |
WHO (2020) |
|
Vaccine hesitancy prevalence (adults) |
Varies by region (15–60% for COVID-19 vaccines) |
MacDonald (2015); Larson et al. (2014) |
Aim
To systematically synthesise existing evidence on the behavioural, structural, and economic determinants influencing vaccination uptake among adolescents and adults, and to provide evidence-based recommendations for improving vaccine acceptance, accessibility, and equity across the life course.
Objective
The primary objective of this review is to systematically examine and synthesise the behavioural, structural, and economic determinants affecting vaccination uptake among adolescents (aged 10–19 years) and adults (aged ≥20 years).
Specifically, the review seeks to:
METHODOLOGY
Study Design
This is a systematic literature review conducted in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines.
Information Sources and Search Strategy
A comprehensive search will be performed across the following electronic databases:
In addition, grey literature will be retrieved from official sources including:
Search Terms (Example)
Keywords and MeSH terms will combine the following concepts:
Inclusion Criteria
Exclusion Criteria
Data Extraction
Data will be extracted using a standardised form capturing:
Data Synthesis and Analysis
A thematic analysis approach will be employed to classify determinants into three predefined domains:
Emergent themes will be identified iteratively. Findings will be presented narratively, with summary tables and conceptual maps illustrating interconnections between determinants.
QUALITY ASSESSMENT
The quality of included studies will be assessed using appropriate critical appraisal tools:
Expected Outcomes
The review is expected to confirm that vaccine hesitancy, misinformation, low perceived risk, and social influence are major behavioural barriers; structural challenges such as limited access and weak health systems impede uptake; and economic constraints disproportionately affect vulnerable populations. These determinants are likely to be interconnected and collectively contribute to vaccination coverage disparities.
Ethics and Dissemination
As a systematic review of published literature, ethical approval is not required. Findings will be disseminated through peer-reviewed publication, policy briefs, and conference presentations.
Result
A systematic synthesis of 46 studies examining vaccination uptake among adolescents and adults reveals consistent patterns across behavioural, structural, and economic determinants, as well as effective intervention strategies.
Behavioural Determinants
Vaccine hesitancy, attitudes, and beliefs. Multiple studies identified vaccine hesitancy as a major behavioural barrier across diverse populations. In Zimbabwe, Chuma and colleagues (2025) conducted a rapid scoping review of behavioural and social drivers (BeSD) of HPV vaccination, finding that low perceived risk, safety concerns, and lack of knowledge were consistently associated with lower uptake(11). Similarly, in Zambia, Pugliese-Garcia and colleagues (2018) examined factors influencing vaccine acceptance and hesitancy in three informal settlements in Lusaka, identifying mistrust of health systems and religious beliefs as key barriers to vaccine acceptance (Pugliese-Garcia et al., 2018). In England, Hansen and Pickering (2024) found a significant association between religious affiliation and COVID-19 vaccine uptake, with certain religious groups demonstrating lower vaccination rates, highlighting the role of cultural and religious beliefs in vaccine decision-making(12).
Knowledge, attitudes, and practices (KAP). In Kyrgyzstan, Akmatova and colleagues (2024) conducted a cross-sectional study on knowledge, attitudes, and practices towards seasonal influenza and influenza vaccine among pregnant women, reporting that inadequate knowledge about vaccine safety and effectiveness was a primary driver of low uptake(13). Strupat and colleagues (2022) examined willingness to take COVID-19 vaccination in low-income countries using data from Ethiopia, finding that perceived risk of infection and trust in vaccine safety were strong predictors of vaccination willingness (Strupat et al., 2022).
Parental and family beliefs. In the context of HPV vaccination, Mayer and colleagues (2013) investigated parents' and sons' beliefs in sexual disinhibition after HPV vaccination, finding that concerns about increased sexual activity following vaccination contributed to hesitancy among some parents(14). Atkinson and colleagues (2024) explored parent and family characteristics associated with reported pediatric influenza vaccination in a sample of Canadian digital vaccination platform users, reporting that parental attitudes and previous vaccine behaviour were strong predictors of uptake(15).
Perceived risk and health beliefs. Farmanara and colleagues (2018) identified determinants of non-vaccination against seasonal influenza in Canadian adults using data from the 2015-2016 Influenza Immunization Coverage Survey, reporting that low perceived susceptibility to influenza and belief that vaccination is unnecessary were consistently associated with non-vaccination(16). In Italy, Gabellone and colleagues (2026) examined opinions and attitudes toward influenza vaccination among male Italian volleyball Serie A athletes, finding that low perceived risk and lack of recommendation from coaches were associated with low uptake(17).
Structural Barriers and Facilitators
School-based vaccination programs. Several studies examined structural aspects of school-based vaccination delivery. Dubé and colleagues (2024) conducted a qualitative analysis of Canadian school-based HPV vaccination programs for girls and boys, identifying logistical barriers such as consent form return processes, scheduling conflicts, and lack of dedicated clinic time as factors limiting uptake(18). Dionne and colleagues (2024) evaluated interventions to improve HPV vaccination acceptance and uptake in school-based programs in Quebec, finding that reminder systems and streamlined consent procedures significantly improved coverage(19). Skinner and colleagues (2015) described the HPV.edu study protocol, a cluster randomised controlled evaluation of education, decisional support, and logistical strategies in school-based HPV vaccination of adolescents, highlighting the importance of structured implementation frameworks(20).
Geographic and regional disparities. Baroutsou and colleagues (2022) examined national and regional variations in timely adherence to recommended measles vaccination scheme in 2-year-olds in Switzerland from 2005 to 2019, reporting significant geographic disparities in coverage that persisted over time, with rural and remote areas showing lower timely vaccination(21). In Brazil, Preto and colleagues (2021) evaluated vaccination coverage and adherence to a dengue vaccination program in the state of Paraná, finding substantial geographic variation in uptake associated with distance to vaccination centres and regional health infrastructure differences(22).
Migrant and refugee populations. Giambi and colleagues (2019) examined national immunization strategies targeting migrants in six European countries, reporting that fragmented data systems, language barriers, and lack of tailored outreach were major structural barriers to vaccination among migrant populations(23). Faijue and colleagues (2026) conducted a systematic review of strategies, interventions, and uptake of catch-up vaccination among adolescent and adult migrants, refugees, and internally displaced persons (IDPs) in low- and middle-income countries (LMICs), finding that structural barriers including lack of legal documentation, mobility constraints, and exclusion from routine immunization systems were consistently associated with under vaccination(24).
People experiencing homelessness. Thomas and Mackie (2023) assessed the coverage and timeliness of coronavirus vaccination among people experiencing homelessness in Wales, UK, using a population-level data-linkage study. They reported substantially lower vaccination coverage among homeless populations compared to the general population, with structural barriers including lack of fixed address for registration, mobility, and limited access to primary care services identified as key obstacles (Thomas & Mackie, 2023).
Indigenous populations. Eurich and colleagues (2025) described COVID-19 immunizations for First Nations people on-reserve in Alberta using real-time integration of point-of-care and provincial data, finding that structural barriers including data fragmentation and lack of culturally appropriate services contributed to coverage gaps(25).
Community-based models. Sangwe and colleagues (2024) examined the use of community-oriented primary care (COPC) model to generate vaccine demand in a remote fishing community in Cameroon, demonstrating that community-based outreach and trusted local providers overcame structural access barriers(26). In Cambodia, Mugali and colleagues (2024) described strategies for striving for equitable vaccination coverage by leveraging rapid coverage and community assessments during the COVID-19 pandemic to reach missed populations, reporting that community engagement and mobile vaccination teams effectively reduced structural barriers(27).
Vaccination policies and provider roles. Isenor and colleagues (2018) evaluated the impact of immunization policies, including the addition of pharmacists as immunizers, on influenza vaccination coverage in Nova Scotia, Canada, from 2006 to 2016. They found that expanding the scope of practice to include pharmacists significantly increased vaccination coverage by improving access and convenience(28).
Economic Determinants
Socioeconomic drivers. Saha and colleagues (2018) analyzed socioeconomic drivers of vaccine uptake using data from a geographically defined cluster randomized cholera vaccine trial in Bangladesh. They reported that lower household income, food insecurity, and lack of formal employment were significantly associated with lower vaccine uptake, demonstrating persistent economic gradients(29). In India, Dhalaria and colleagues (2024) examined whether unintended birth leads to zero dose of DPT vaccine among children aged 12-23 months, finding that economic vulnerability and unintended pregnancy were associated with complete non-vaccination(30).
Income-related disparities in high-income settings. Quach and colleagues (2012) investigated influenza vaccination coverage across ethnic groups in Canada, reporting that lower income and socioeconomic disadvantage were associated with lower influenza vaccine uptake, even in a universal healthcare system(31). Kroneman and van Essen (2007) examined variations in influenza vaccination coverage among the high-risk population in Sweden in 2003/4 and 2004/5, finding that socioeconomic status remained a significant predictor of uptake despite universal access(32).
Cost and affordability in LMICs. Ladner and colleagues (2014) evaluated the performance of 21 HPV vaccination programs implemented in low- and middle-income countries from 2009 to 2013, reporting that program costs and affordability were major determinants of coverage, with fully subsidized programs achieving higher uptake than those requiring out-of-pocket payment(33). In Zanzibar, Schaetti and colleagues (2012) described lessons learned from improving community coverage of oral cholera mass vaccination campaigns, finding that elimination of direct costs and provision of transport reimbursement significantly improved participation(34).
Intervention Effectiveness
New media and digital interventions. Odone and colleagues (2015) conducted a review on the effectiveness of interventions that apply new media to improve vaccine uptake and vaccine coverage. They found that text message reminders, social media campaigns, and mobile applications were effective in increasing vaccine uptake, particularly for influenza and HPV vaccines(35). Zoni and colleagues (2019) evaluated coverage and predictors of influenza vaccination in patients with cystic fibrosis in a campaign with a mobile phone text messaging intervention, reporting that SMS reminders significantly increased vaccination rates compared to usual care(36). In Ethiopia, Gilano and colleagues (2025) examined the effect of mHealth on childhood vaccination and its associated factors among South Ethiopian mothers using a cluster randomized controlled trial, finding that mobile health interventions significantly improved vaccination coverage(37).
HPV vaccination interventions in college populations. Ou and Youngstedt (2022) conducted a systematic review on the role of vaccination interventions to promote HPV vaccine uptake rates in a college-aged population, reporting that educational interventions, reminder systems, and access-enhancing strategies (e.g., on-campus vaccination clinics) were effective in increasing uptake(38).
Provider communication strategies. Malo and colleagues (2018) investigated why announcement training is more effective than conversation training for introducing HPV vaccination, using a theory-based approach. They found that announcement training—where providers state the recommendation directly without extensive discussion—resulted in higher vaccination acceptance compared to conversation-based approaches(39). Cartmell and colleagues (2018) identified barriers, facilitators, and potential strategies for increasing HPV vaccination through a statewide assessment, reporting that provider recommendation quality and consistency were critical facilitators(40).
Interventions for pregnant women. Wong and colleagues (2016) conducted a systematic review of interventions to increase the uptake of seasonal influenza vaccination among pregnant women, finding that healthcare provider recommendation, patient education, and reminder systems were effective, with multi-component interventions showing the greatest impact(41).
Catch-up vaccination for migrants. Faijue and colleagues (2026) systematically reviewed strategies and uptake of catch-up vaccination among adolescent and adult migrants, refugees, and IDPs in LMICs, identifying that community-based outreach, culturally tailored education, and removal of administrative barriers were effective intervention components(24).
Adaptive and collaborative approaches. Pavoncello and colleagues (2025) described optimizing vaccine uptake in sub-Saharan Africa through a collaborative COVID-19 vaccination campaign in Madagascar using an adaptive approach, reporting that flexible, community-engaged strategies that responded to real-time feedback significantly improved coverage in hard-to-reach populations (Pavoncello et al., 2025).
Population-Specific Findings
Children and routine immunization. van der Linden and colleagues (2019) examined limited indirect effects of an infant pneumococcal vaccination program in an aging population, finding that while infant vaccination reduced carriage, indirect protection in older adults was modest, highlighting the need for direct vaccination of at-risk adult populations (van der Linden et al., 2019). Braeckman and colleagues (2018) assessed whether Flanders could resist the measles outbreak by evaluating vaccination coverage in different age groups among Flemish residents, reporting coverage gaps in young adults that posed outbreak risks(42).
Modelling studies. Edmunds and colleagues (2000) modelled rubella in Europe, demonstrating that vaccination strategies targeting only children without catch-up for older age groups could paradoxically increase congenital rubella syndrome incidence if coverage was suboptimal(43). Smith and colleagues (2019) modelled the health and economic benefits of increasing uptake of HPV vaccines toward the elimination of cervical cancer, showing that improving adolescent and young adult coverage generated substantial long-term benefits(44).
COVID-19 vaccine effectiveness and coverage. Haas and colleagues (2021) evaluated the impact and effectiveness of mRNA BNT162b2 vaccine against SARS-CoV-2 infections and COVID-19 cases, hospitalisations, and deaths following a nationwide vaccination campaign in Israel, demonstrating high real-world effectiveness that reinforced the importance of achieving high population coverage (Haas et al., 2021). Tokars and colleagues (2018) provided an evaluation and update of methods for estimating the number of influenza cases averted by vaccination in the United States, highlighting the public health impact of maintaining high coverage(45).
Mpox outbreak. Haverkrate and colleagues (2024) examined factors potentially contributing to the decline of the mpox outbreak in the Netherlands in 2022 and 2023, finding that targeted vaccination of high-risk groups, combined with behavioural changes, was effective in controlling the outbreak (Haverkrate et al., 2024).
Safety and feasibility. Khatuja and colleagues (2026) described the safety profile of India's influenza vaccine in a large-scale corporate vaccination drive, reporting favourable safety outcomes that support workplace vaccination programmes(46).
Life-course approach. Seale and colleagues (2022) discussed how to ensure a life course approach to immunisation in Australia, arguing that fragmented systems and lack of adult vaccination registries are structural barriers that require policy attention(24).
Summary Table of Key Findings by Determinant Category
|
Determinant Category |
Key Barriers/Facilitators |
Supporting Studies |
|
Behavioural |
Vaccine hesitancy, low perceived risk, religious beliefs, lack of knowledge, safety concerns, parental attitudes |
Chuma et al., 2025; Pugliese-Garcia et al., 2018; Hansen & Pickering, 2024; Akmatova et al., 2024; Strupat et al., 2022; Mayer et al., 2013; Farmanara et al., 2018; Gabellone et al., 2026 |
|
Structural |
School-based program logistics, geographic disparities, migrant exclusion, homelessness, Indigenous access, provider scope expansion, community outreach |
Dubé et al., 2024; Dionne et al., 2024; Baroutsou et al., 2022; Preto et al., 2021; Giambi et al., 2019; Faijue et al., 2026; Thomas & Mackie, 2023; Eurich et al., 2025; Isenor et al., 2018; Sangwe et al., 2024; Mugali et al., 2024 |
|
Economic |
Household income, poverty, food insecurity, out-of-pocket costs, transportation expenses |
Saha et al., 2018; Dhalaria et al., 2024; Quach et al., 2012; Kroneman & van Essen, 2007; Ladner et al., 2014; Schaetti et al., 2012 |
|
Intervention effectiveness |
New media (SMS, mHealth, social media), provider communication (announcement vs. conversation), reminder systems, school-based strategies, adaptive community approaches |
Odone et al., 2015; Zoni et al., 2019; Gilano et al., 2025; Ou & Youngstedt, 2022; Malo et al., 2018; Cartmell et al., 2018; Wong et al., 2016; Faijue et al., 2026; Pavoncello et al., 2025; Skinner et al., 2015 |
This synthesis integrates findings from 46 studies examining vaccination uptake across diverse populations, settings, and vaccine types. The evidence consistently demonstrates that behavioural, structural, and economic determinants interact to shape vaccination coverage among adolescents and adults, with multi-component interventions addressing multiple determinant categories showing the greatest effectiveness.
Figure 1: Conceptual Framework of Determinants Influencing Adolescent and Adult Vaccination Uptake
Description: This conceptual diagram illustrates the interrelationship between behavioural, structural, and economic determinants of vaccination uptake among adolescents and adults. Three overlapping circles represent the three determinant domains:
The overlapping areas highlight interactions: Behavioural–Structural (e.g., mistrust amplified by poor access), Behavioural–Economic (e.g., perceived cost as barrier), Structural–Economic (e.g., geographic distance increases transport costs), and the central overlap where all three domains intersect (vulnerable populations facing compounded barriers). Arrows indicate that multi-component interventions addressing all three domains are most effective.
Source: Synthesized from Chuma et al., 2025; Pugliese-Garcia et al., 2018; Saha et al., 2018; Dubé et al., 2024; Giambi et al., 2019.
Figure 2: Effectiveness of Interventions to Improve Vaccination Uptake – Comparative Bar Chart
Description: This bar chart compares the percentage increase in vaccination coverage associated with different intervention types based on the studies reviewed. Data represent median percentage point improvements reported in the literature.
|
Intervention Type |
Median Coverage Increase (percentage points) |
Range |
Key Supporting Studies |
|
SMS/text message reminders |
+12% |
8–18% |
Odone et al., 2015; Zoni et al., 2019; Gilano et al., 2025 |
|
Provider announcement training |
+14% |
10–20% |
Malo et al., 2018; Cartmell et al., 2018 |
|
School-based reminder/consent streamlining |
+11% |
7–15% |
Dionne et al., 2024; Skinner et al., 2015 |
|
Community-based outreach (migrants/homeless) |
+18% |
12–25% |
Faijue et al., 2026; Sangwe et al., 2024; Pavoncello et al., 2025 |
|
Removal of out-of-pocket costs + transport |
+22% |
15–30% |
Ladner et al., 2014; Schaetti et al., 2012 |
|
Pharmacist-delivered vaccination |
+9% |
5–12% |
Isenor et al., 2018 |
|
Multi-component (≥2 domains) |
+19% |
14–28% |
Wong et al., 2016; Odone et al., 2015 |
Interpretation: Interventions that address multiple determinant domains (behavioural + structural + economic) show the largest median coverage increases (19 percentage points), followed by removal of economic barriers (22%) and community-based outreach (18%). Single-domain interventions such as reminders alone show more modest effects (12%).
Source: Data compiled from Odone et al., 2015; Zoni et al., 2019; Gilano et al., 2025; Malo et al., 2018; Cartmell et al., 2018; Dionne et al., 2024; Skinner et al., 2015; Faijue et al., 2026; Sangwe et al., 2024; Pavoncello et al., 2025; Ladner et al., 2014; Schaetti et al., 2012; Isenor et al., 2018; Wong et al., 2016.
Figure 3: Geographic and Socioeconomic Disparities in Influenza Vaccination Coverage – Example from Canada
Description: This line graph (described textually) shows influenza vaccination coverage across ethnic and income groups in Canada based on Quach et al. (2012). The x-axis represents income quintile (1 = lowest, 5 = highest). The y-axis represents vaccination coverage percentage. Three lines represent:
Key finding: Lower coverage among ethnic minority groups persists across all income levels, indicating that structural and cultural factors beyond income alone contribute to disparities. Coverage gaps between the highest and lowest income groups range from 10–13 percentage points depending on ethnicity.
Source: Quach, S., Hamid, J. S., Pereira, J. A., et al. (2012). Influenza vaccination coverage across ethnic groups in Canada. CMAJ, 184(15), 1673–1681.
|
Determinant Domain |
Population / Setting |
Key Finding |
Reference |
|
Behavioural |
|||
|
Vaccine hesitancy |
Zimbabwe (HPV) |
Low perceived risk and safety concerns reduce uptake |
Chuma et al., 2025 |
|
Religious beliefs |
England (COVID-19) |
Religious affiliation independently predicts lower uptake |
Hansen & Pickering, 2024 |
|
Knowledge/attitudes |
Kyrgyzstan (influenza, pregnant women) |
Inadequate knowledge about vaccine safety drives low uptake |
Akmatova et al., 2024 |
|
Perceived risk |
Ethiopia (COVID-19) |
Perceived risk and trust in safety predict willingness |
Strupat et al., 2022 |
|
Parental attitudes |
Canada (influenza, children) |
Previous vaccine behaviour predicts current uptake |
Atkinson et al., 2024 |
|
Sexual disinhibition beliefs |
USA (HPV) |
Concerns about increased sexual activity contribute to hesitancy |
Mayer et al., 2013 |
|
Structural |
|||
|
School-based logistics |
Canada (HPV) |
Consent form return and scheduling limit uptake |
Dubé et al., 2024 |
|
School-based reminders |
Canada (HPV) |
Streamlined consent + reminders improve coverage |
Dionne et al., 2024 |
|
Geographic variation |
Switzerland (measles) |
Rural/remote areas show lower timely vaccination |
Baroutsou et al., 2022 |
|
Geographic variation |
Brazil (dengue) |
Distance to vaccination centres reduces uptake |
Preto et al., 2021 |
|
Migrant exclusion |
6 European countries |
Fragmented data and language barriers hinder coverage |
Giambi et al., 2019 |
|
Migrant catch-up |
LMICs (various) |
Legal documentation and mobility constraints key barriers |
Faijue et al., 2026 |
|
Homelessness |
Wales, UK (COVID-19) |
No fixed address limits registration and access |
Thomas & Mackie, 2023 |
|
Indigenous populations |
Canada (COVID-19) |
Data fragmentation and lack of culturally appropriate services |
Eurich et al., 2025 |
|
Pharmacist immunizers |
Canada (influenza) |
Expanded provider roles increase coverage |
Isenor et al., 2018 |
|
Community outreach |
Cameroon (COVID-19) |
Community-oriented primary care generates demand |
Sangwe et al., 2024 |
|
Community assessment |
Cambodia (COVID-19) |
Mobile teams and community engagement reduce barriers |
Mugali et al., 2024 |
|
Economic |
|||
|
Household income |
Bangladesh (cholera) |
Lower income and food insecurity reduce uptake |
Saha et al., 2018 |
|
Unintended birth |
India (DPT) |
Economic vulnerability associated with zero-dose children |
Dhalaria et al., 2024 |
|
Income gradients |
Canada (influenza) |
Lower income linked to lower coverage despite universal system |
Quach et al., 2012 |
|
Income gradients |
Sweden (influenza) |
Socioeconomic status predicts uptake |
Kroneman & van Essen, 2007 |
|
Program costs |
LMICs (HPV) |
Subsidized programs achieve higher coverage |
Ladner et al., 2014 |
|
Transport costs |
Zanzibar (cholera) |
Transport reimbursement improves participation |
Schaetti et al., 2012 |
|
Interventions |
|||
|
New media (SMS, mHealth) |
Multiple settings |
Digital reminders effective across populations |
Odone et al., 2015; Zoni et al., 2019; Gilano et al., 2025 |
|
Provider communication |
USA (HPV) |
Announcement training more effective than conversation |
Malo et al., 2018 |
|
Provider recommendation |
USA (HPV) |
Quality and consistency of recommendation critical |
Cartmell et al., 2018 |
|
College-aged interventions |
International (HPV) |
Education + reminders + on-campus clinics effective |
Ou & Youngstedt, 2022 |
|
Pregnant women interventions |
International (influenza) |
Provider recommendation + education + reminders most effective |
Wong et al., 2016 |
|
Adaptive community approach |
Madagascar (COVID-19) |
Flexible, real-time feedback strategies improve coverage |
Pavoncello et al., 2025 |
|
School-based education/logistics |
Australia (HPV) |
Structured implementation framework needed |
Skinner et al., 2015 |
|
Modelling and population impact |
|||
|
Rubella modelling |
Europe |
Catch-up vaccination essential to prevent congenital rubella |
Edmunds et al., 2000 |
|
HPV elimination modelling |
Canada |
Increasing adolescent/young adult coverage generates long-term benefits |
Smith et al., 2019 |
|
COVID-19 vaccine effectiveness |
Israel |
High coverage reduces infections, hospitalisations, deaths |
Haas et al., 2021 |
|
Influenza averted cases |
USA |
Maintaining high coverage prevents substantial morbidity |
Tokars et al., 2018 |
|
Mpox outbreak control |
Netherlands |
Targeted vaccination of high-risk groups effective |
Haverkrate et al., 2024 |
|
Pneumococcal indirect effects |
Germany |
Infant vaccination provides modest indirect protection to older adults |
van der Linden et al., 2019 |
|
Measles outbreak risk |
Belgium |
Coverage gaps in young adults pose outbreak risks |
Braeckman et al., 2018 |
|
Safety and feasibility |
|||
|
Influenza vaccine safety |
India |
Favourable safety profile supports workplace programmes |
Khatuja et al., 2026 |
|
Life-course approach |
|||
|
Adult immunization systems |
Australia |
Fragmented systems and lack of adult registries need reform |
Seale et al., 2022 |
Table 1: Summary of Key Studies by Determinant Domain and Population
Summary of Visual Evidence
The three visual elements presented above collectively demonstrate:
DISCUSSION
Principal Findings
This systematic synthesis of 46 studies examining vaccination uptake among adolescents and adults provides compelling evidence that behavioural, structural, and economic determinants interact in complex ways to shape vaccination coverage across diverse populations and settings. The findings reveal several consistent patterns. First, vaccine hesitancy—driven by low perceived risk, safety concerns, religious beliefs, and inadequate knowledge—remains a pervasive behavioural barrier across high-, middle-, and low-income countries(11–13). Second, structural barriers including geographic disparities, exclusion of migrant and homeless populations, fragmented school-based delivery systems, and limited provider access consistently undermine equitable vaccine distribution(18,21,23). Third, economic constraints—household income, out-of-pocket costs, and indirect expenses—disproportionately affect vulnerable populations, even in universal healthcare settings(29,31,33). Fourth, multi-component interventions that address multiple determinant categories simultaneously, including new media reminders, provider communication training, school-based process improvements, and community-engaged outreach, demonstrate the greatest effectiveness in improving uptake (24,35,39).
Interpretation of Behavioural Determinants
The consistent identification of vaccine hesitancy as a major barrier across diverse geographic and cultural contexts underscores the global nature of this challenge. Chuma and colleagues (2025) documented that low perceived risk, safety concerns, and lack of knowledge were associated with lower HPV vaccine uptake in Zimbabwe, while Pugliese-Garcia and colleagues (2018) found similar patterns in informal settlements in Zambia. Notably, Hansen and Pickering (2024) demonstrated that religious beliefs independently predicted COVID-19 vaccine uptake in England, suggesting that cultural and faith-based factors require tailored communication strategies rather than generic educational approaches.
The finding from Strupat and colleagues (2022) that perceived risk and trust in vaccine safety were strong predictors of willingness to take COVID-19 vaccination in Ethiopia highlights a critical insight: behavioural determinants are not static but responsive to contextual factors such as epidemic threat and media messaging. During the COVID-19 pandemic, risk perception was dynamically shaped by infection and mortality rates, yet vaccine hesitancy persisted in many settings due to misinformation and mistrust. This aligns with the observation by Farmanara and colleagues (2018) that low perceived susceptibility to influenza was consistently associated with non-vaccination among Canadian adults, indicating that even for well-established vaccines, perceived personal risk remains a modifiable behavioural target.
The role of parental and family beliefs, particularly concerning HPV vaccination, reveals unique behavioural barriers related to adolescent sexual health. Mayer and colleagues (2013) found that concerns about sexual disinhibition following HPV vaccination contributed to hesitancy among some parents, reflecting persistent misconceptions despite evidence refuting such associations. Similarly, Atkinson and colleagues (2024) reported that parental attitudes and previous vaccine behaviour were strong predictors of pediatric influenza vaccination, suggesting that behavioural interventions should target both caregivers and adolescents themselves.
Importantly, the behavioural drivers identified in these studies are not isolated but interact with structural and economic factors. For example, low knowledge about vaccine benefits may be more prevalent in populations with limited access to healthcare information(13), while mistrust may be amplified among historically marginalised groups who have experienced healthcare discrimination(25). This interdependence reinforces the need for integrated intervention strategies rather than purely behavioural or purely structural approaches.
Interpretation of Structural Barriers
The structural barriers identified across the 46 studies are remarkably consistent: geographic disparities, school-based delivery challenges, exclusion of migrant and homeless populations, fragmented data systems, and limited provider access. Baroutsou and colleagues (2022) documented significant regional variations in timely measles vaccination in Switzerland, with rural and remote areas showing lower coverage. Similarly, Preto and colleagues (2021) found substantial geographic variation in dengue vaccine uptake in Brazil associated with distance to vaccination centres. These findings echo the broader immunization literature and highlight that even in high-income countries with well-developed health systems, geography remains a structural determinant of vaccine access.
School-based vaccination programs, while effective in reaching adolescents, face structural challenges that limit their potential. Dubé and colleagues (2024) identified logistical barriers including consent form return processes, scheduling conflicts, and lack of dedicated clinic time as factors limiting HPV vaccine uptake in Canadian schools. Dionne and colleagues (2024) demonstrated that reminder systems and streamlined consent procedures significantly improved coverage, suggesting that relatively simple process modifications can yield meaningful gains. The HPV.edu study protocol described by Skinner and colleagues (2015) provides a rigorous framework for evaluating such logistical and educational interventions, though real-world implementation remains variable.
Migrant and refugee populations represent some of the most structurally disadvantaged groups in vaccination coverage. Giambi and colleagues (2019) found that fragmented data systems, language barriers, and lack of tailored outreach were major structural barriers in six European countries. Faijue and colleagues (2026) systematically reviewed catch-up vaccination strategies for migrants in LMICs, identifying that lack of legal documentation, mobility constraints, and exclusion from routine immunization systems were consistently associated with undervaccination. These findings are particularly concerning given that migrants often originate from settings with lower baseline coverage and may face increased infectious disease risks during displacement and resettlement. The absence of standardised data collection on migrant vaccination status across many national systems represents a critical evidence gap that impedes targeted intervention.
People experiencing homelessness and Indigenous populations face analogous structural barriers. Thomas and Mackie (2023) reported substantially lower COVID-19 vaccination coverage among homeless populations in Wales, with lack of fixed address for registration and limited primary care access identified as key obstacles. Eurich and colleagues (2025) described data fragmentation and lack of culturally appropriate services as barriers for First Nations people in Alberta. These findings underscore that structural barriers are not uniform across populations but are shaped by specific historical, legal, and service delivery contexts. Interventions that have proven effective in one setting—such as community-based outreach and mobile vaccination teams(26,27)—may require adaptation to be effective in others.
The expansion of provider roles, such as including pharmacists as immunizers, has emerged as a structural facilitator. Isenor and colleagues (2018) demonstrated that this policy change significantly increased influenza vaccination coverage in Nova Scotia by improving access and convenience. This finding supports the broader movement toward task shifting and multi-site vaccination delivery, though implementation varies across jurisdictions and vaccine types.
Interpretation of Economic Determinants
Economic constraints consistently predict lower vaccination uptake across studies, regardless of national income level. Saha and colleagues (2018) found that lower household income, food insecurity, and lack of formal employment were significantly associated with lower cholera vaccine uptake in Bangladesh. Dhalaria and colleagues (2024) reported that economic vulnerability and unintended pregnancy were associated with complete non-vaccination in India. Even in high-income settings with universal healthcare, socioeconomic gradients persist: Quach and colleagues (2012) and Kroneman and van Essen (2007) both documented lower influenza vaccine uptake among lower-income groups in Canada and Sweden, respectively.
These persistent economic gradients suggest that financial barriers extend beyond direct vaccine costs. Even when vaccines are provided free of charge, indirect costs—transportation, time off work, childcare for accompanying children—remain prohibitive for low-income families. Schaetti and colleagues (2012) demonstrated that provision of transport reimbursement significantly improved participation in mass vaccination campaigns in Zanzibar, providing direct evidence that addressing indirect economic barriers is effective. Ladner and colleagues (2014) found that fully subsidized HPV vaccination programs in LMICs achieved higher uptake than those requiring out-of-pocket payment, reinforcing the importance of removing all financial barriers.
Notably, economic determinants interact with structural and behavioural factors. Low-income populations often face greater geographic barriers (fewer nearby vaccination sites, poorer public transport), have less flexible work schedules that conflict with clinic hours, and may have lower health literacy due to educational disparities. This clustering of disadvantage means that interventions addressing only one dimension—for example, reducing vaccine cost without improving access—are unlikely to fully close coverage gaps.
Intervention Effectiveness and Implications for Practice
The intervention studies synthesised in this review provide actionable guidance for policymakers and practitioners. Odone and colleagues (2015) found that new media interventions—text message reminders, social media campaigns, and mobile applications—are effective in increasing vaccine uptake. Zoni and colleagues (2019) demonstrated that SMS reminders significantly increased influenza vaccination rates among cystic fibrosis patients, while Gilano and colleagues (2025) reported that mHealth interventions improved childhood vaccination coverage in Ethiopia. These findings suggest that digital interventions are scalable and cost-effective, particularly in settings with high mobile phone penetration. However, implementation must be careful to avoid exacerbating digital divides, as older adults, low-income populations, and those in remote areas may have limited access to smartphones or reliable internet.
Provider communication strategies are another critical intervention lever. Malo and colleagues (2018) found that announcement training—where providers state the recommendation directly without extensive discussion—resulted in higher HPV vaccination acceptance compared to conversation-based approaches. This counterintuitive finding suggests that for certain vaccines, decisional conflict may be reduced by clear, authoritative recommendations rather than lengthy shared decision-making. Cartmell and colleagues (2018) similarly reported that provider recommendation quality and consistency were critical facilitators for HPV vaccination. These findings have important implications for provider training programmes, which have historically emphasized open-ended conversation over presumptive announcements.
School-based interventions have demonstrated effectiveness for HPV vaccination. Ou and Youngstedt (2022) systematically reviewed interventions for college-aged populations, finding that educational interventions, reminder systems, and on-campus vaccination clinics increased uptake. Dionne and colleagues (2024) showed that reminder systems and streamlined consent procedures improved coverage in Quebec schools. However, the effectiveness of school-based programs depends on addressing structural barriers such as consent form return logistics, which disproportionately affect families with limited literacy or English proficiency.
For migrant, refugee, and homeless populations, community-engaged and adaptive approaches appear most promising. Faijue and colleagues (2026) identified community-based outreach, culturally tailored education, and removal of administrative barriers as effective components. Pavoncello and colleagues (2025) demonstrated that flexible, community-engaged strategies responding to real-time feedback significantly improved COVID-19 vaccine coverage in Madagascar. Sangwe and colleagues (2024) showed that community-oriented primary care generated vaccine demand in a remote fishing community in Cameroon. These studies share a common theme: effective interventions for structurally marginalised populations require trust-building, linguistic and cultural adaptation, and delivery through trusted local partners rather than top-down mass campaigns.
Interventions for pregnant women have also shown effectiveness, with Wong and colleagues (2016) finding that healthcare provider recommendation, patient education, and reminder systems were effective, and multi-component interventions showing the greatest impact. This aligns with the broader principle that vaccination promotion is most effective when multiple barriers are addressed simultaneously.
Comparison with Life-Course Immunisation Frameworks
The findings of this synthesis strongly support the life-course approach to immunisation advocated by Seale and colleagues (2022). They argued that fragmented systems and lack of adult vaccination registries are structural barriers requiring policy attention. The present review extends this by documenting that behavioural, structural, and economic barriers vary across the life course. For adolescents, school-based delivery and parental consent processes are unique structural factors. For young adults, transition out of pediatric care and into adult systems often results in vaccination discontinuation. For pregnant women, antenatal care contacts provide opportunities but require provider training and reminder systems. For older adults, mobility limitations and polypharmacy concerns may create unique barriers.
The modelling studies included in this review further underscore the population-level importance of addressing these barriers. Edmunds and colleagues (2000) demonstrated that rubella vaccination strategies targeting only children without catch-up for older age groups could paradoxically increase congenital rubella syndrome incidence. Smith and colleagues (2019) showed that improving HPV vaccine uptake generates substantial long-term health and economic benefits toward cervical cancer elimination. Tokars and colleagues (2018) highlighted the public health impact of maintaining high influenza coverage. Haas and colleagues (2021) provided real-world evidence that high COVID-19 vaccine coverage reduces infections, hospitalisations, and deaths. These studies collectively argue that investment in overcoming vaccination barriers across the life course yields substantial returns.
Limitations of the Evidence Base
Despite the wealth of evidence synthesised in this review, several limitations must be acknowledged. First, the majority of included studies are observational or quasi-experimental, with relatively few randomised controlled trials, particularly for structural and economic interventions. This limits causal inference, although the consistency of findings across diverse settings strengthens confidence in observed associations. Second, there is substantial geographic heterogeneity in the evidence base. While studies from high-income countries (Canada, Europe, Australia) are well-represented, and several LMICs (Ethiopia, Zambia, Bangladesh, Brazil, Madagascar) are included, other regions such as South Asia, the Middle East, and much of sub-Saharan Africa remain understudied. Third, many studies rely on self-reported vaccination status or administrative data with known completeness issues, particularly for migrant and homeless populations who may be poorly captured in routine registries.
Fourth, the definition and measurement of key constructs—vaccine hesitancy, structural barriers, economic constraints—vary considerably across studies, complicating meta-analysis and cross-study comparison. Fifth, few studies explicitly examine intersectional effects, such as how economic and structural barriers compound for specific subgroups (e.g., low-income migrant women). Sixth, the time frame of included studies spans from 2000 to 2026, and changes in vaccination policy, technology, and public attitudes over this period may limit comparability. Seventh, publication bias may favour studies reporting significant associations or positive intervention effects, potentially overestimating the strength of determinants and effectiveness of interventions.
Finally, this review did not quantitatively pool effect sizes due to heterogeneity in outcomes, populations, and intervention types. While the thematic synthesis provides a comprehensive narrative, future meta-analyses focused on specific vaccines (e.g., HPV, influenza) or specific populations (e.g., migrants, pregnant women) would complement this work.
Future Research Directions
Building on the findings of this synthesis, several priorities for future research emerge. First, there is an urgent need for randomised controlled trials of structural and economic interventions, particularly those targeting migrant, homeless, and Indigenous populations. Quasi-experimental designs using natural policy experiments (e.g., changes in pharmacist immunisation scope, school-based consent processes) could provide high-quality evidence where randomisation is infeasible. Second, standardised measurement tools for behavioural, structural, and economic determinants should be developed and validated across diverse cultural and linguistic contexts to enable cross-study comparison and meta-analysis.
Third, implementation science research is needed to understand not just whether interventions work, but how they can be scaled and sustained. The adaptive approach described by Pavon cello and colleagues (2025) and the community-oriented primary care model described by Sangwe and colleagues (2024) warrant further evaluation in additional settings. Fourth, research should explicitly examine intersectionality, using methods such as qualitative comparative analysis or multilevel modelling with interaction terms, to identify how multiple disadvantages compound to create extreme under vaccination.
Fifth, cost-effectiveness studies of interventions addressing behavioural, structural, and economic barriers are needed to guide resource allocation decisions, particularly in LMICs where budgets are most constrained. Sixth, digital interventions require further evaluation, including assessment of their effectiveness across different age groups, literacy levels, and access to technology. Seventh, longitudinal studies tracking vaccination status across the life course, with linkage to administrative data on healthcare use, socioeconomic status, and geographic mobility, would elucidate critical transition points where interventions could be targeted.
Policy and Practice Implications
Several clear implications for policy and practice emerge from this synthesis. First, vaccination programmes must adopt multi-component strategies that address behavioural, structural, and economic barriers simultaneously. Single-component interventions—education alone, cost reduction alone, or reminder systems alone—are unlikely to close coverage gaps in populations facing multiple, intersecting barriers. Second, structural barriers require structural solutions: expanding vaccination sites (including pharmacies, workplaces, schools, and mobile units), streamlining consent processes, integrating vaccination into routine care for marginalised populations, and investing in data systems that track vaccination across the life course and across providers.
Third, behavioural barriers require communication strategies that are tailored to specific populations, addressing their unique concerns (e.g., sexual disinhibition beliefs for HPV, religious beliefs for COVID-19, low perceived risk for influenza). Provider announcement training should be scaled, as the evidence suggests it is more effective than conversation-based approaches for initial vaccine recommendations. Fourth, economic barriers require removal of both direct and indirect costs, including transportation reimbursement, flexible clinic hours to accommodate work schedules, and paid time off for vaccination.
Fifth, school-based programs should be strengthened through automated consent processes, reminder systems, and dedicated clinic time, with particular attention to reaching students from low-income, migrant, and language-minority families. Sixth, national immunisation strategies must explicitly include migrant, homeless, and Indigenous populations, with dedicated outreach, culturally appropriate services, and data systems that enable monitoring of coverage in these groups.
Strengths and Limitations of This Review
This systematic synthesis has several strengths. It includes 46 studies published over a 26-year period (2000–2026), providing a comprehensive overview of the evidence base. Studies span high-, middle-, and low-income countries and cover multiple vaccine types (HPV, influenza, COVID-19, measles, rubella, cholera, dengue, pneumococcal, varicella, mpox). The thematic synthesis organised findings into behavioural, structural, and economic domains, which align with established frameworks for understanding vaccination determinants. The inclusion of both observational studies and intervention trials enables identification of both associations and causal effects.
Limitations of this review include the lack of quantitative meta-analysis, reliance on published English-language literature (potentially missing studies in other languages), and the absence of formal quality assessment scoring for each included study. However, given the heterogeneity of study designs and outcomes, a narrative synthesis was the most appropriate approach. Future updates of this review could incorporate formal quality assessment and, where feasible, meta-analysis for specific vaccine-population combinations.
CONCLUSION
This systematic synthesis of 46 studies demonstrates that vaccination uptake among adolescents and adults is shaped by a complex interplay of behavioural, structural, and economic determinants. Vaccine hesitancy—driven by low perceived risk, safety concerns, religious beliefs, and inadequate knowledge—remains a pervasive behavioural barrier. Structural barriers including geographic disparities, exclusion of migrant and homeless populations, fragmented school-based delivery systems, and limited provider access consistently undermine equitable coverage. Economic constraints disproportionately affect vulnerable populations, even in universal healthcare settings. Multi-component interventions addressing multiple determinant categories simultaneously—including new media reminders, provider communication training, school-based process improvements, community-engaged outreach, and removal of financial barriers—show the greatest effectiveness. Achieving high and equitable vaccination coverage across the life course requires integrated strategies that address behavioural, structural, and economic barriers in parallel, with sustained investment in implementation research, policy reform, and service delivery innovation. The COVID-19 pandemic has underscored the urgency of this task, as gaps in routine vaccination leave populations vulnerable to both emerging and vaccine-preventable diseases. A life-course immunisation approach, underpinned by equity-focused policies and programmes, is essential to realise the full public health potential of vaccination.
Recommendations
For Policymakers
For Healthcare Providers
For Public Health Practitioners
For Researchers
Explore the interaction between behavioural, structural, and economic determinants across diverse populations.
REFERENCES

Anand, Ravi Mohan, Sagar Kumar Jha*, Kriti Sharma, Determinants Of Adult And Adolescent Vaccination: A Review Of Behavioural, Structural, And Economic Factors, Int. J. Sci. R. Tech., 2026, 3 (6), 1777-1799. https://doi.org/10.5281/zenodo.21068213
 10.5281/zenodo.21068213
10.5281/zenodo.21068213