
We use cookies to ensure our website works properly and to personalise your experience. Cookies policy
SSJ GIMSR, Almora, Uttrakhand
The 2022 WHO classification of Endocrine and Neuroendocrine Tumours divide thyroid tumours into new categories to provide a clearer understanding of their cell of origin, pathologic features, molecular classification, and biological behaviour. Some neoplasms were subclassified, renamed, or redefined as a specific entity. Histopathologic variants of PTC and FTC were redefined to better stratify prognosis and management of patients. Advances in our understanding of the molecular genetics of thyroid cancer is leading to development of a variety of biomarkers that are being used as early detection markers, prognostic markers, and markers for predicting treatment responses. This review introduces changes in the fifth edition WHO classification of thyroid tumours and updates the contemporary diagnosis and classification of thyroid tumours. We also discuss several challenges with the proposal of new diagnostic rare entities, as they have unique histopathologic, immunogenic reactivity, and molecular features and clinical relevance.
Thyroid cancer is the most prevalent endocrine cancer, and it is one of the fastest-growing malignancies in the world. Females are three times more likely than males to develop thyroid cancer, and it is the fifth most common tumour among women. It is the ninth most prevalent malignancy, according to the National Cancer Institute’s Surveillance, Epidemiology, and End-Result (SEER) database. Depending upon wide spectrum of morphology and behaviour, with its pathogenesis ranging from common and indolent tumours to aggressive malignancies, there are four main histologic subtypes of thyroid cancer, namely papillary thyroid carcinoma (PTC), follicular thyroid carcinoma (FTC), medullary thyroid carcinoma (MTC), and anaplastic thyroid carcinoma (ATC). Among these variants, PTC is the most common, occurring in 80% of all reported thyroid cancer cases and being the one with the best prognosis. The thyroid gland is composed of two types of cells; follicular cells that generate thyroid hormone and parafollicular cells (C cells) that secrete calcitonin. Differentiated thyroid cancers include PTC and FTC, which are derived from follicular cells. ATC contains undifferentiated cells that develop from follicular cells, whereas MTC is derived from C cells.1
Clinical, epidemiologic, and pathologic evidence supports the concept of stepwise progression and dedifferentiation. For example, the gradual loss of papillary and follicular growth patterns and the simultaneous increase in a solid growth pattern, with increased mitoses, necrosis, and nuclear pleomorphism, are often observed in aggressive thyroid carcinomas. A majority of these tumours exhibit residual foci of differentiated thyroid carcinoma. There exhibits relative frequency of the so-called rare tumours of the thyroid that were redefined to better stratify prognosis and management of the patients.
Over the last 15 years, the importance of molecular biology in thyroid pathology has both revolutionized the discipline and, at the same time, proven the inherent value of classical histopathology. It is a field in which pathologists have long recognized patterns that reflect specific molecular alterations, but the addition of molecular tools to the pathologist’s armamentarium has enhanced our ability to prognosticate and predict the efficacy of targeted therapies.
This review will focus on the most important and novel changes in the new WHO thyroid tumour classification scheme (Table 1). We encourage the reader to use this as a framework to understand the new classification.
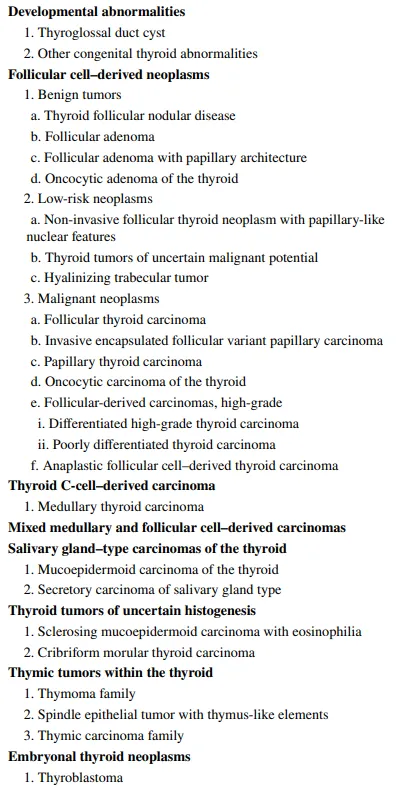
Table 1. WHO classification scheme of thyroid neoplasm, 5th edition2
A new terminology proposed in this new edition, “thyroid follicular nodular disease” that avoids defining a lesion as hyperplastic, neoplastic, or the contradictory “adenomatous hyperplasia”.3 An unusual but clinically important tumour is follicular adenoma with papillary architecture. This is a benign non-invasive encapsulated follicular cell-derived neoplasm characterized by a distinct “centripetal” intrafollicular papillary architecture that is more organized than PTC, lacks nuclear features of PTC. Unlike follicular adenomas that harbor RAS mutations, these tumours are often associated with activating TSHR mutations (in up to 70% of cases) or GNAS mutations and/or EZH1 mutations.4-6 These tumours are features of McCune-Albright syndrome due to germline mosaic GNAS mutations, and Carney complex, due to germline inactivating mutations in PRKAR1A that also cause constitutive activation of the cAMP-protein kinase A (PKA) pathway.7
The importance of oncocytic change in the thyroid cannot be overemphasized therefore oncocytic follicular adenomas now hold their own special place in the classification. The term “Hurthle cell” is discouraged; it is actually a misnomer since Hurthle described the C cells of the thyroid gland.8 It is associated with GRIM19 (NDUFA13) gene mutation, and more than one-third have copy number variations.9
These are borderline tumours that are morphologically and clinically intermediate between benign and malignant tumours. Histologically, they are classified into three types including non-invasive follicular thyroid neoplasm with papillary-like nuclear features (NIFTP), thyroid tumours of uncertain malignant potential (UMP), and hyalinizing trabecular tumour (HTT). In the 2017 WHO classification, HTT was described in a different chapter from that of NIFTP and UMP tumours, but in new edition, they were all combined into one category of low-risk follicular cell-derived neoplasms.10
Some studies reported BRAF V600E and lymph node metastasis in a subset of NIFTPs with <1% papillae. In a study performed at Memorial Sloan Kettering Cancer Center, lymph node metastasis or tumour recurrence was not found in non-invasive encapsulated PTC even if the criterion for the percentage of papillae extended to 10%.11 Therefore, in the absence of BRAF V600E mutation, the original criterion allowing <1% true papillae remains unchanged in the 2022 WHO classification.12
They are defined as “well-differentiated thyroid tumours with follicular architecture that are encapsulated or unencapsulated but well-circumscribed. They are divided into two subtypes according to their nuclear alterations: follicular tumour of uncertain malignant potential (FT-UMP) that lacks PTC-like nuclear features (nuclear score 0-1) and well-differentiated tumour of uncertain malignant potential (WDT-UMP) that has more or less pronounced nuclear features of PTC (nuclear score of 2-3). The term “atypical adenoma” is not recommended. Some of these tumours can have oncocytic features and may display clear cells or glomeruloid features and mucinous stromal changes. Tumours of UMP are distinguished from follicular adenoma and NIFTP by the presence of questionable capsular or vascular invasion.13-17 Encapsulated or well-demarcated follicular-patterned thyroid neoplasms are characterized by the high prevalence of RAS-like molecular alterations and the lack of BRAF V600E.
HTTs are well demarcated nodules with PTC-like nuclear changes, trabecular architecture, and a peculiar prominent intratrabecular hyaline material not seen in other thyroid neoplasms that have accumulated as the result of secretion of an active basal membrane type of protein. The relationship between HTT and PTC was initially suggested by the detection of RET::CCDC6 rearrangements, but still not confirmed.18-22 Recent molecular studies have demonstrated that HTT is a distinct thyroid neoplasm with a specific molecular alteration. GLIS gene rearrangements define HTT and have not been identified in other thyroid tumours.23-24 While HTTs lack BRAF and RAS mutations. The most common rearrangement types are PAX8::GLIS3 (the most frequent type) and PAX8::GLIS1. Diagnosis can be confirmed by a peculiar membrane staining of MIB1 antibody tested at room temperature, in conjunction with immunopositive follicular markers such as thyroglobulin, TTF1, and PAX8.24 The intratrabecular eosinophilic hyaline material resembles amyloid but negative with the congo red stain. It is diastase-resistant material that stains with the periodic acid-Schiff stain and is immunoreactive for collagen IV.
PTC is the most common malignancy of follicular cell derivation in both adult and pediatric populations.25 PTC commonly occurs as a sporadic tumour, however, familial forms are being increasing appreciated.26 Until the 2017 WHO classification of thyroid tumours, PTC was exclusively diagnosed based on characteristic nuclear cytology regardless of growth pattern and invasive features.27-28 The 5th edition of WHO classification introduced the diagnostic term NIFTP (non-invasive follicular thyroid neoplasm with papillary-like nuclear features) that changed the diagnostic criteria as now done on the basis of molecular studies. Based on the molecular data, PTC can be considered as “less well-differentiated” form of carcinoma than follicular carcinoma or encapsulated follicular variant papillary carcinoma.29 BRAF V600E is the most common molecular alteration in classic PTC and its subtypes with papillary growth pattern and infiltrative tumours with follicular architecture. These BRAF-like tumours show focal to diffuse papillary growth and readily identifiable characteristic nuclear features; they are most often infiltrative, but can be localized with expansile growth or pushing borders, or confined to a cyst.30-31 Telomerase reverse transcriptase (TERT) promoter mutations, as a secondary pathogenic event, are encountered in 10% of PTCs. RET gene rearrangements (CCDC6::RET and NCOA4::RET) are found in classic PTC and other subtypes.32-33 A strong association is reported between RET rearrangements and radiation-induced PTC.32 Other less common molecular variations in PTC include gene fusion in NTRK and other genes, mutations in other gene expression and altered microRNA expression.33-36
Among PTC variants, tall cell, columnar cells, and hobnail variants are of undoubted clinical significance, since they are aggressive variants associated with aggressive clinicopathological features and worse prognosis than for classic and encapsulated PTC. In the 2015 American Thyroid Association risk stratification system, patients with these three aggressive variants are classified as having an intermediate risk of recurrence.
PTC variants:
It is a BRAF-like lesion that has the infiltrative growth pattern of classic PTC but lacks prominent papillae; it has predominant follicular architecture but florid nuclear atypia, prominent psammoma bodies, and stromal fibrosis, and focal small papillary structures. It showed association with BRAF V600E and K601E mutations as well as NRAS and CTNNB1 gene mutations. RET translocation, NTRK and ALK fusions were also seen.37
At least 30% of tumour cells are two to three times as tall as they are wide, arranged in tightly packed follicular follicles and papillae, also known as “tram track appearance”. Histologically it shows nuclear features of PTC along with abundant to moderate eosinophilic cytoplasm with distinct cytoplasmic border. There is increasing evidence that PTCs with as little as 10% tall cell change have a worse prognosis than those without tall cells and that PTCS with focal tall cell change (>10%) should be reported and handled beyond the low-risk classification. The diagnosis of the tall cell variant should not be missed, in that patients with this variant are more refractory to radioactive iodine ablation and have a worse prognosis than those with classic PTC. BRAF V600E mutations are most common (approximately 90% of cases) as compared to other subtypes; TERT promoter mutations have also been reported in some cases. The molecular events seen in TC-PTC include loss of heterozygosity for chromosome 1 and TP53 mutation.38
The columnar cell variant consists of columnar cells with marked pseudostratified hyperchromatic nuclei and the absence of conventional PTC nuclear features. It is an interesting finding that CDX2, a gut-specific nuclear transcription factor, the expression of which is a putative feature of intestinal-type differentiation, is positive in 10% to 55% of this variant, which may behave indolently or aggressively depending on tumour encapsulation and tumour size. CC variants of circumscribed or intrathyroidal types have an excellent prognosis, whereas invasive tumours with extrathyroidal extension have a less favourable prognosis. It is associated with BRAF V600E mutation; less common are BRAF fusions, RAS mutations, TERT promoter mutations, and loss of CDKN2A and TP53 mutations.39
A rare variant requiring >30% of tumour cells with hobnail features. The prevalence of HV of PTC ranges from 0.2% to 1.2% of all PTCs. Hobnail features in PTC were first described by Kakudo et al. in 2004 as loss of cellular polarity and cohesiveness, with the main growth pattern of micropapillary and papillary structure, which was correlated with a higher risk of recurrence. Some studies clarifying that hobnail features represented an aggressive growth and were correlated with poor prognosis, in that most cases had lymph node/distant metastases and local recurrence.
HV of PTC must be differentiated from classic PTCs showing hobnail-like morphology, which is associated with papillae with the hyalinized and oedematous fibrovascular core. The typical areas of HV of PTC can be mixed with aggressive histologic variants such as tall cell, columnar cell and/or trabecular/solid variant in varying proportions. Although hobnail features are more commonly observed in association with poorly differentiated thyroid carcinoma (PDTC) (22%) than with PTC (1.3%), the differential diagnosis between HV of PTC and PDTC should be made according to the Turin criteria. Interestingly, numerous small papillary formations partially covered with hobnail cells are typically seen in the diffuse sclerosing variant of PTC, but in this variant, the papillae are located within extensive squamous metaplasia, a large number of psammoma bodies, lymphocytic thyroiditis and prominent fibrosis. The neoplastic cells have a mean ki-67 proliferation index (as determined using the MIB1 antibody) of 10%. Tumour cells are immunoreactive for thyroglobulin, thyroid transcription factor-1(TTF-1), TTF-2 (FOXE1), paired box-8 (PAX-8), cytokeratin (CK AE1/3, CK7, CK19), epithelial membrane antigen (EMA), Hector-Battifora mesothelial cell-1 (HBME-1), galactin-3, cyclin D1, p27KIP1 and PTEN. Tumour cells are negative for CK20, thyroperoxidase, calcitonin, chromogranin A and synaptophysin. BRAF V600E mutations are the most common genetic alteration in this variant, followed by deleterious TP53 mutations as well as TERT promoter and PIK3CA mutations. Rarely, RET rearrangements, molecular CTNNB1, EGFR, ATK1, ATM, ARID2, and NOTCH1 gene mutations were involved.37
It is unusual for PTC to exhibit foci of solid and/or trabecular growth. This pattern is more common in paediatric tumours. The term “solid variant” should be used when all or nearly all of a tumour not belonging to any of the other variants has a solid, trabecular, or nested (insular) appearance. The solid variant constitutes 1-3% of adult papillary carcinomas. It is more common in young patients and in patients with a history of exposure to ionizing radiation. Radiation-associated pediatric cases frequently show RET/PTC3 rearrangement and sporadic cases show RET/PTC1/3 and ETV6/NTRK3 fusions. BRAF V600E mutations are less commonly found than are classic PTC.37
DSV of PTC is more frequent in female, young patients. It is a PTC variant that diffusely involves one or both thyroid lobes, clinical mimicking Hashimoto’s thyroiditis. This variant is characterized by dense sclerotic stroma involving nests of solid, squamoid, spindled and papillary arranged cells. Abundant psammoma bodies, lymphocytic infiltration and extensive lymph vessel invasion are also present. Lymph node and lung metastases are frequent. Tumour cells express focally thyroglobulin, TTF-1, PAX8 and p63.
RET/PTC rearrangements represented the genetic initiation event for this variant. The BRAF V600E mutation is rare in this variant. This variant is associated with extrathyroidal extension, cervical lymph node and distant metastasis, and shorter disease-free survival; however, the mortality rate is comparable to that of the classic variant. The excellent long-term survival despite a higher recurrence rate may result from the favourable effect of younger patient age.37
They are extremely rare and without known impact on prognosis include the following: the oncocytic classic PTC with well-developed papillae lined by oncocytic cells; warthin-like PTC essentially an oncocytic PTC with papillary growth and heavy lymphoplasmacytic infiltrate in its stroma that bears morphologic similarities to warthin tumour of salivary glands; and the rare clear cell subtype.
Other less common PTC subtypes discussed in the 5th edition of WHO classification of thyroid neoplasms include spindle cell PTC and PTC with fibromatosis/fasciitis-like/desmoid-type stroma.40-42The former can be difficult to distinguish from other neoplasms without the use of proper ancillary tools. The latter is an unusual tumour that has two discrete components: a BRAF-mutated PTC embedded within a fibromatosis that has CTNNB1 mutation and nuclear localization of beta-catenin.
FTC is the second common malignancy with follicular cell differentiation, which lacks the diagnostic nuclear features of PTC.43 The highest annual incidence rate of FTC was among patients aged 70-79. FTC and encapsulated follicular variant papillary thyroid carcinoma (EFVPTC) harbor somatic mutations of RAS gene family members NRAS. HRAS, and KRAS that are recurrently found in follicular pattern tumours. Of these, NRAS mutations are the most prevalent, most often represented by recurrent codon 61 mutations, and less often of codon 12/13 alterations. While RET and TRK fusions do not seem to play a role in the development of follicular patterned lesions. PAX8::PPARG rearrangements are frequently reported (10-40% of cases).44PAX8::PPARG fusions and RAS mutations are mutually exclusive, and the rearrangement is predominantly observed in younger patients with smaller primary tumours.45-46 Moreover, FTCs often display alterations in genes related to the AKT signaling pathway, such as deleterious PTEN mutations, activating PI3KCA mutations, and PIK3CA copy number gain. As PTEN negatively regulates PI3K mediated activation of the oncogenic PI3K-AKT pathway, these alterations lead to augmented AKT signaling and tumorigenesis. Apart from MAPK and PI3K-AKT signaling pathway alterations, a subset of FTCs may harbor mutations in miRNA processor genes DICER1 and DGCR8.47-49 The mutations are believed to perturb the maturation of miRNAs, causing dysregulation of various target genes. As in PTCs, subset of FTCs (15-20%) and IEFVPTC harbors TERT promoter mutations, and FTCs with this alteration exhibit a specific transcriptome and miRNA landscape compared to wild-type cases.50-51 TERT promoter mutations are particularly amassed in cases with distant metastases and poor patient outcomes. Moreover, tumour mutational burden has also been implicated as a prognostic tool in FTC, and this factor was more confident in predicting patients outcome than conventional histological subtyping.49
It accounts for approaching 5% of differentiated thyroid carcinomas, can occur anywhere in the thyroid and usually presents as a slowly enlarging painless solitary thyroid nodule. There are no known risk factors for developing OCA. The mean age of patient at diagnosis is approximately 60 years. It is more common in women (F:M::1.6:1).10 Oncocytic follicular cell-derived thyroid carcinomas as a group can include many different entities: oncocytic PTC, oncocytic encapsulated follicular subtype of PTC, oncocytic poorly differentiated carcinoma, and oncocytic medullary thyroid carcinoma.52-53 However, the term “oncocytic carcinoma of the thyroid" is used in the new WHO to refer to invasive malignant follicular cell neoplasms composed of at least 75% oncocytic cells in which the nuclear features of PTC and high-grade features are absent. This term replaces Hurthle cell carcinoma, a misnomer given that Hurthle actually described parafollicular C cells. It represents the malignant counterpart of oncocytic adenoma.54 Although there are no major substantive changes to the description of these tumours in the 2022 WHO, it is helpful to review the distinct clinicopathologic correlates of OCA.
Histologically OCAs are encapsulated tumours with capsular and/or vascular invasion and at least 75% oncocytic cells. OCAs are subclassified into minimally invasive (those with capsular invasion only), encapsulated angioinvasive, and widely invasive (those with gross invasion through the gland) tumours due to differences in clinical outcome. When evaluating OCA, it is important not only to document extent of invasion, but also to evaluate for progression to oncocytic poorly differentiated thyroid carcinoma; thus all tumours should be assessed for increased mitotic activity (3 or more mitoses per 10 hpf/~2mm2) and tumour necrosis. OCA can metastasize to lymph nodes.55 Some authors have shown that OCA usually spreads to distant sites via blood vessels. Distant metastasis at presentation are seen in 15-27% of patients with OCA and in up to 40% of tumours with extensive vascular invasion.56
Prognosis is depending on staging of tumour and patient’s age. The 5-year overall survival has been reported to be 85%, but only 24% among patients with distant metastases at diagnosis compared to 91% for patients with M0 disease at diagnosis. Benign and malignant oncocytic thyroid tumours have both been shown to harbor homoplasmic or highly heteroplasmic (>70%) mitochondrial DNA mutations in complex I subunit genes of the electron transport chain. OCAs include loss of chromosomes 2, 8, and 22 and gains of chromosomes 7, 12, and 17. OCAs have also been shown to have recurrent DNA mutations, including RAS mutations (though at a lower rate than is seen with follicular thyroid carcinoma), EIF1AX, TERT, TP53, NF1, and CDKN1A.57-59
They are usually develop through genetic multistep fashion from a pre-existing well-differentiated thyroid carcinoma by establishing mutations in MAPK or PI3K-AKT signaling pathways. As the majority of DHGTCs develop from PTCs, the BRAF V600E mutation and PTC-related gene fusions are the most common “early-type” driver gene events in these lesions, while PDTCs are enriched for RAS mutations, indicating a relationship to FTCs or EFVPTC. DHGTCs and PDTC acquire variable gene alterations along their path of progression, including TP53 and TERT promoter mutations.60-61 In adolescent patients with PDTC, DICER1 mutations seem common and may reflect a coupling between high-grade features and an underlying disturbance of miRNA regulation.62
The majority of ATCs develop through dedifferentiation from a preceding well-differentiated DHGTC or PDTC. Thus, ATC developing from PTCs or DHGTCs often carry TERT promoter mutations with synchronous BRAF mutations, while ATCs arising from FTCs or EFVPTCs usually carry combinations of RAS and TERT promoter mutations.63 Moreover, tp53 gene mutations are commonly reported, as are deletions of CDKN2A/B (encoding cell cycle regulators p16 and p14, respectively).63 Subsets of ATC with mismatch repair (MMR) gene mutations display a hypermutator phenotype compared to non-MMR gene mutated cases, but the clinical relevance of this observation is not known.64-65
Includes benign neoplasms such as spindle cell adenoma, meningioma-like follicular adenoma, pericystic-like follicular adenoma, and hyalinizing trabecular neoplasms; and malignant neoplasms such as hyperfunctioning (Hot) follicular thyroid carcinoma. There is no significant changes in new addition of WHO classification. they have shown similar histologic features, immunoreactivity and molecular gene alteration as described in previous WHO classification.10
MTC is a malignant tumour of the thyroid gland composed of cells with evidence of C-cell differentiation. It accounts for <2-3% of all thyroid malignancies. The peak incidence of sporadic tumours occurs among patients in their fifth or sixth decade of life, with younger patient ages in hereditary cases. About 30% of MTCs are heritable, with an autosomal dominant pattern of inheritance caused by gain-of-function germline mutations in the RET proto-oncogene. Currently, MTC is considered a variant along the spectrum of disease expression in MEN2A.2
There is no change in definitive histologic description of MTC in new WHO classification, and no widely recognized histopathological grading system for this entity in previous edition of classification. In 2020, two groups independently developed grading scheme for MTC based on proliferative activity (mitotic count and ki67 proliferative index) and tumour necrosis.66-67Subsequently 2021, a two-tiered grading system named “The international medullary thyroid carcinoma grading scheme”. In this system, high-grade tumours are defined as having at least one of the three following features: tumour necrosis, mitotic count >5 per 2mm2, and/or a ki67 proliferation index >5%.68 One study has shown that there was no correlation between grade and RET or RAS mutation status. This novel histologic grade may benefit high-grade patients leading to closer follow-up, low thresholds for cross-sectional imaging, and careful monitoring for distant metastasis. Additionally, this histologic grade can be used as a data point in clinical trials of adjuvant therapy since it is likely that adjuvant therapy will have greatest benefit in high-grade medullary carcinomas. There is no more changes in its subtypes/ variant classification and their respective molecular pathology in the new edition of WHO.
ATC is a highly aggressive thyroid malignancy composed of undifferentiated follicular thyroid cells. It is also known as undifferentiated thyroid carcinoma, sarcomatoid carcinoma, metaplastic carcinoma, spindle cell carcinoma, giant cell carcinoma, carinosarcoma, or pleomorphic based on the respective variable histologic presentation.it is the most aggressive form of primary thyroid malignancies, with a median 1-year survival rate of only 10-20%. Patients are typically elderly and present with advanced-stage tumours; the female-to-male ratio is 2:1. Tumour cells show immunoreactivity for PAX8, and CK; while show negative expression of TTF1 and thyroglobulin. In the previous WHO classification, SCC of the thyroid (i.e. carcinoma composed almost entirely of squamous cells without a differentiated carcinoma component) was considered a separate entity from anaplastic thyroid carcinoma. In the recent multi-institutional study, pure SCC with or without a differentiated thyroid carcinoma component displayed BRAF V600E mutations in 87% of cases and had an outcome similar to ATC in general. In addition, these SCC express PAX8 and TTF1 in 91% and 38% of cases, respectively, confirming their follicular cell origin.69 Furthermore, pure SCC without any differentiated thyroid carcinoma component (i.e. fulfilling the 2017 WHO definition of SCC) carries BRAF V600E mutations in 60% of cases and has the same prognosis as ATC. From the above reason, SCC of the thyroid is now classified as a morphologic pattern of ATC.
A wide variety of genetic alterations found in ATC. The most frequently mutated gene is TP53 (in 30-70% of cases) followed by other recurring alterations include BRAF V600E mutation and RAS mutation (NRAS, KRAS, or HRAS; mutated in 20% of cases), PIK3CA (in 10-20%), PTEN (IN 10-15%), and ALK. Another important addition to the ATC is the emphasis on rapid and prompt testing of all anaplastic carcinomas for the presence of BRAF V600E mutation. This testing is mandatory since the combination of BRAF and MEK inhibitors was found to be active against BRAF V600E-mutated anaplastic carcinoma.70 This testing can be performed using immunostaining against the mutated protein or through genotyping. As described in previous WHO also that alterations in p73, beta-catenin, RAF genes are also seen. Copy-number gains have been found in ATCs, in genes such as EGFR, FLT1 (also called VEGFR1; in 45%), PDGFRB (in 38%), and PIK3CA/B (in 38%). Epigenetic and microRNA changes have been reported to be associated with ATC.
The 5th edition of the WHO classification of endocrine tumours has introduced minor changes and a new approach in SGTNs for appropriate diagnostic and therapeutic purpose. It includes mucoepidermoid carcinoma with its subtype “mucinous carcinoma”, and the secretory carcinoma. It is one of the rare entity with 48 reported cases.71 Sclerosing mucoepidermoid carcinoma with eosinophilia shares some features with the above tumours, but has currently been classified within the group of uncertain histogenesis tumours.
MEC has been defined as a malignant neoplasm of salivary gland type, characterized by mucinous, intermediate, and squamoid tumour cells, having a solid or cystic growth pattern. Generally, epidermoid cells are cytologically bland and predominate over mucocytes in the dense fibrotic stroma of the tumour, although the proportion of each component can vary significantly. In fact, the very rare mucinous carcinoma of the thyroid has been incorporated in this entity. The histogenesis of MEC is controversial; a link to ectopic salivary gland tissue or solid cell nests has been suggested. Thus, squamous metaplasia is the currently favoured precursor event.72 IHC may help confirm this diagnosis with CK and p63 expression, in the absence of neuroendocrine markers and calcitonin. While, follicular lineage markers are expressed in a fraction of cases only, including thyroglobulin, TTF1, and PAX8.72-74
Although only 12 cases are on record, SC of the thyroid gland (also known as mammary analog of secretory carcinoma) has been incorporated in the new WHO classification of thyroid tumours as part of the salivary gland-type neoplasms. It is both morphological and genetically similar to its mammary and salivary gland counterparts and does not share the histological and immunophenotypical features of differentiated follicular cell-derived carcinomas. It contains more specific molecular alterations involving the ETV6 gene. Although to SC of other sites, the diagnostic hallmarks include a solid, papillary, tubular, or microcystic growth of eosinophilic cells with vacuolated, “bubbly” cytoplasm; rare cases may show high-grade features.75 Nuclear atypia is bland, and occasional nuclear clearing and contour irregularities can be detected. SC is diffusely immunoreactive for GATA3, mammaglobin, and S100 in the absence of thyroglobulin, TTF1, and PAX8 expression.76 ETV6 translocations are the hallmark of SC, with fusion products with NTRK3. In the salivary gland SC series, a novel fusion of ETV6 with RET was detected, but this alteration has not been reported in the thyroid, yet. It follows a more aggressive course than that of other locations, with locoregional recurrences and distant spread in up to 30% of cases.71-72
It is a rare entity with 12 reported cases. Intra- or perithyroidal thymic tumours are grouped under the umbrella of thymic tumours and thymoma and spindle epithelial tumour with thymus-like elements and thymic carcinoma.
Compared to the WHO 2017 classification, no major changes occurred in the new WHO scheme: three types of thymic tumours in the thyroid region are described, with benign and malignant tumours sharing a thymic epithelial differentiation included under the term “thymoma family” and “thymic carcinoma family”. They are postulated to develop from either ectopic thymus or from branchial pouch remnants differentiating along the thymic line. Hassall bodies may in fact be seen at the periphery of these tumours.77
Thymoma develop within or attached to the thyroid, generally in the left lower lobe portion, from embryological remnants. Histologically, they resemble their mediastinal counterparts, all subtypes being represented, with solid, or lobular growth of cuboidal, spindled, or squamoid cells in a loose stroma infiltrated by immature, TdT-positive, T lymphocytes. Rare cases are invasive, but most are well circumscribed or encapsulated tumours, occasionally entrapping thyroid follicles, and after surgery follow an uneventful course.78-79
It is a rare malignant tumour generally arising in the pediatric age or in young male adults with less than 50 cases reported in the literature. Histologically, a lobulated growth of two epithelial cell types with spindle or cuboidal shape (the latter arranged in tubules, papillae or glands) is observed. Tumour cells have low-grade atypia and a low proliferative activity, which helps to distinguish this tumour from sarcomas, medullary carcinomas, and sarcomatoid anaplastic carcinoma. No recurrent molecular alterations have so far been identified. SETTLE has a relatively good prognosis with over 80% 5-year survival rate, although cases with locoregional and distant metastases (mostly to the lung) are on record.80-81
It is a malignant tumour with thymic epithelial differentiation that affects the adult population with a slight female preponderance and a high occurrence in Asians. It develops in intra- or perithyroidal regions, generally in the lower poles as a firm, solid mass of variable size.77,82 The old terminologies CASTLE and lymphoepithelioma-like carcinoma are no longer recommended in the new WHO classification. Histologically, ITC shares the orthotopic thymic carcinoma features, with a lobulated growth of squamous (keratinizing or basaloid) epithelial cells in a desmoplastic stroma infiltrated by lymphocytes and plasma cells. Tumour cells have poorly defined cell borders, mild nuclear atypia, distinct nucleoli, and a low proliferative activity. The ITC immunophenotype includes expression of CK, CD5, p63, CD117, CEA, p53 and bcl-2, in the absence of thyroid follicular markers (thyroglobulin, TTF1) and of EBV-related markers (EBER).82 Recurrent TERT promoter mutations have been reported in ITC, but not in mediastinal thymic carcinomas.83
At this moment, no molecular tests are required for the diagnostic classification of thymomas, SETTLE, and intrathyroid thymic carcinomas.
The tumour previously known as the “cribriform-morular variant of papillary thyroid carcinoma” can be associated with familial adenomatous polyposis (FAP) or may occur as a sporadic form. It was originally classified as a subtype of papillary carcinoma because of the presence of papillae and in some instances diagnostic nuclear features.
Several studies have shown that this tumour has a molecular profile distinct from follicular cell-derived thyroid carcinoma. In contrast to latter that harbor mutations in the MAPK pathway (e.g., BRAF, RAS), these tumours do not display BRAF V600E mutations and only rarely have RAS or PIK3CA mutations. Almost all cribriform-morular tumours have genetic alterations in the Wnt/beta-catenin pathway with APC mutations being the most common and found in both the familial and sporadic setting.84-86 Mutations in other genes involved in the Wnt/beta-catenin pathways such as CTNNB1 have also been detected.85-86 By IHC, these tumours show diffuse cytoplasmic and nuclear beta-catenin expression. In addition, a recent study , it has been shown that the follicular cell derivation of this neoplasm since it often lacks PAX8 and thyroglobulin expression while retaining TTF1 protein only in the cribriform elements. The cribriform areas also express estrogen and progesterone receptors. The morulae are positive for CD5, CK5. CDX2, and CK5, but lack TTF1 expression.87 In the new WHO classification scheme and the tumour is now classified under the umbrella of thyroid tumours of uncertain histogenesis.
It is a rare thyroid tumour with less than 60 cases, characterized by a morphology partially overlapping with that of MEC, in association with a marked infiltration of lymphocytes and eosinophils in the fibrotic stroma.77,88 Associated with papillary carcinoma is reported in 20% of cases. The immunoprofile resembles that of MEC with no expression of follicular markers, except for TTF1 in half of the cases. A few genotyped cases of SMECE lack the typical genetic alteration of MEC of salivary gland (i.e. MAML2 translocation). Associations with anaplastic thyroid carcinoma and with NUT carcinoma have been reported.89-90
The histiogenesis of this low-grade malignant tumour is debated and the new WHO classification included this entity among tumours of uncertain histiogenesis. An origin from ultimobranchial cells is favoured, but the genomic profile has not identified gene alterations associated with either MEC or PTC, with rare exceptions. Mutations typical of follicular cell-derived thyroid carcinomas such as BRAF V600E have also not been found.91 While some have hypothesized a follicular cell origin through the mechanism of squamous metaplasia of the follicular epithelium, this view is not supported by the lack of PAX8 and thyroglobulin positivity. Because of the presence of p63 in the tumour, some authors have favoured an origin from solid cell nests. While other investigators acknowledge that the origin of this rare carcinoma is unknown.88
CONCLUSION
The 2022 WHO classification categorized thyroid neoplasm into benign, borderline and malignant tumours. Certain types of thyroid cancers were reclassified as borderline tumours. Histopathologic variants of PTC and FTC were redefined to better stratify the prognosis and management of patients. Some newly terms were introduced while a few terms were discouraged. Recent advances in understanding the molecular biology of thyroid cancer aid in the development of novel molecular-based strategies to effectively tackle these diagnostic, prognostic, and therapeutic obstacle of thyroid cancer.
REFERENCES

Samaira Rawat*, Sufiyan Zaheer, Molecular Alteration In Rare Entities Of Thyroid Neoplasm: A Review Of The 2022 WHO Classification, Int. J. Sci. R. Tech., 2026, 3 (7), 434-448. https://doi.org/10.5281/zenodo.21389488
 10.5281/zenodo.21389488
10.5281/zenodo.21389488