
We use cookies to ensure our website works properly and to personalise your experience. Cookies policy
M.A.M College of Pharmacy, Andhrapradesh
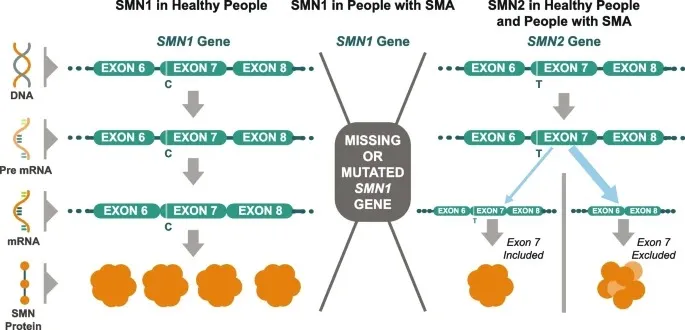
Onasemnogene abeparvovec, sold under the brand name Zolgensma, is a gene therapy used to treat spinal muscular atrophy (SMA), a disease causing muscle function loss in children. It involves a one-time infusion of the medication into a vein It works by providing a new copy of the SMN gene that produces the SMN protein.¹. SMA stems from an SMN1 gene mutation, causing SMN protein deficiency vital for motor neuron survival. Onasemnogene abeparvovec, a biologic drug utilizing AAV9 virus capsids containing an SMN1 transgene, is administered to motor neurons, boosting SMN protein levels. Common side effects include vomiting and elevated liver enzymes, while more severe reactions involve liver issues and low platelet count.². Developed by Alexi’s and acquired by Novartis, onasemnogene abeparvovec gained various FDA designations and approvals globally. Controversies included data manipulation concerns and delayed reporting to regulatory agencies. Onasemnogene abeparvovec's price is high, earning it the title of the world's most expensive medication at the time of commercial approval. This has later been exceeded by other gene therapies like Hemgenix. Japan negotiated a lower price for Zolgensma for its public healthcare system.³
Zolgensma is indicated for the treatment of: patients with 5q spinal muscular atrophy (SMA) with a bi-allelic mutation in the SMN1 gene and a clinical diagnosis of SMA Type 1, or. Patients with 5q SMA with a bi-allelic mutation in the SMN1 gene and up to 3 copies of the SMN2 gene.â´
Zolgensma has been shown to be the more effective medication for SMA Type 1 in trials pertaining to motor function and survival rate. While only 71% of individuals in the Nusinersen had a rise in their score, 100% of patients who took Zolgensma saw an increase of four or more CHOP-INTEND points. These studies demonstrate that Zolgensma is the more effective medication for SMA Type 1 in terms of motor function.âµ
ZOLGENSMA is an adeno-associated virus (AAV) vector-based gene therapy indicated for the treatment of pediatric patients less than 2 years of age with spinal muscular atrophy (SMA) with bi-allelic mutations in the survival motor neuron 1 (SMN1) gene.Onasemnogene abeparvovec is a non-replicating recombinant adeno-associated virus serotype 9 (AAV9) based vector containing the cDNA of the human survival motor neuron (SMN) gene under the control of the cytomegalovirus enhancer/chicken-β-actin-hybrid promoter. Onasemnogene abeparvovec is produced in human embryonic kidney cells by recombinant DNA technology.â¶
Cases of acute liver failure with fatal outcomes have been reported. Acute serious liver injury, acute liver failure, and elevated aminotransferases can also occur with ZOLGENSMA. Patients with preexisting liver impairment may be at higher risk. Prior to infusion, assess liver function of all patients by clinical examination and laboratory testing. Administer systemic corticosteroid to all patients before and after ZOLGENSMA infusion. Continue to monitor liver function for at least 3 months after infusion, and at other times as clinically indicated. If acute serious liver injury or acute liver failure is suspected, promptly consult a pediatric gastroenterologist or herpetologist.â·
TREATMENT:
DOSE AND INFUSION:
1. Treat patients with systemic corticosteroids (equivalent to oral prednisolone at 1 mg/kg/day) 24 hours before ZOLGENSMA infusion. Continued corticosteroid treatment is required following infusion.â¸
2. Clinical signs or symptoms of infection should not be evident at the time of ZOLGENSMA infusion.
3. ZOLGENSMA is provided as a kit customized to meet the weight-based dosing requirements of each patient.â¹
4. ZOLGENSMA is a suspension administered as a single intravenous infusion over 60 minutes. Insertion of a backup catheter prior to administration is recommended.¹â°
INFUSION AND ADMINSTRATION:
Administer ZOLGENSMA to patients who are clinically stable in their overall baseline health status. Postpone infusion in patients with infections until the infection has resolved and the patient is clinically stable. Clinical signs or symptoms of infection should not be evident at the time of ZOLGENSMA infusion.1
ZOLGENSMA is a suspension administered as an intravenous infusion over 60 minutes. A programmable syringe pump should be used to infuse the full volume of ZOLGENSMA. The recommended dose of ZOLGENSMA is 1.1 × 1014 vector genomes per kilogram (vg/kg) of body weight.¹¹
The recommended treatment regimen is detailed in the prescribeing information and on the After Treatment page of this website. Prophylactic corticosteroid treatment is required to help manage potential increases in liver Prednisolone should be administered daily at 1 mg/kg/day (or equivalent if another corticosteroid is used) for 30 days (including the day of administration of Zolgensma) following infusion with Zolgensma. At the end of the 30-day period of systemic corticosteroid treatment, check liver status clinically and by assessing ALT, AST, and total bilirubin Liver function should be monitored for at least 3 months following Zolgensma infusion, and at other times as clinically indicated (see section 6 Warnings and precautions). Promptly consult a pediatric gastroenterologist or herpetologist if patients do not respond adequately to the equivalent of 1 mg/kg/day oral prednisolone. If oral corticosteroid therapy is not tolerated or not effective, intravenous corticosteroids may be considered as clinically indicated (see section 6 Warnings and precautions).¹² Variance from these recommendations is at the discretion of the treating physician. If another corticosteroid is used by the physician in place of prednisolone, similar considerations and approach to taper the corticosteroid dose after 30 days following infusion with Zolgensma should be taken as appropriate.
ADVERSE EFFECTS :
Nausea and elevated liver enzymes. Serious adverse reactions may include liver problems and low platelets.¹³
PLACEBO TRAILS:
Transient elevated levels of cardiac troponin‑I were observed in clinical trials; the clinical importance of these findings is not known. However, cardiac toxicity was seen in studies of other animals in albino mice.¹â´

CONCLUSION
The rare genetic neuromuscular condition known as spinal muscular atrophy (SMA), which affects roughly 1 in 10,000 live births in the US, has two approved treatments from the FDA. Spin Raza (nusinersen, Biogen Idec) is an antisense oligonucleotide that targets SMN2 to produce more functional SMN protein and was approved in 2016 for the treatment of any subtype of SMA. On May 24, 2019, Zolgensma (onasemnogene abeparvovec, Novartis AG/Avex is) received approval to treat patients with any subtype of SMA who were younger than two years old. Oneintravenous dosage of the gene treatment Zolgensma is givens that replaces the native gene that is missing or damaged by delivering a copy of the SMN1 gene using the adeno-associated virus serotype 9 vector (AAV9).¹âµ The most exciting advancement in medicine is the emergence of new, highly effective treatments for a disease that affects children and results in severe disability and death. It is still very early in the study process to determine the true long-term impacts of Spin Raza and Zolgensma, especially for Zolgensma. Nonetheless, the most severe form of SMA has demonstrated notable short-term benefits, and the use of both drugs is anticipated to shift toward presymptomatic children as genetic screening at birth becomes more widespread.¹â¶
REFERENCES

M. Prasada Rao*, Y. Narasimha Rao, S. Rajini, P. Venkata Lokesh, Onasemnogene Abeparvovec On Gene Therapy In Spinal Muscular Dystrophy, Int. J. Sci. R. Tech., 2026, 3 (6), 737-740. https://doi.org/10.5281/zenodo.20639017
 10.5281/zenodo.20639017
10.5281/zenodo.20639017