
We use cookies to ensure our website works properly and to personalise your experience. Cookies policy
Department of Radiology, Docversity University School of Medicine
Positron Emission Tomography–Computed Tomography (PET/CT) has become integral to modern oncology, offering combined functional-metabolic and anatomical information. Recent technological advances – including digital PET detectors, high-performance time-of-flight (TOF) systems, and hybrid PET/MRI platforms – have markedly enhanced PET image quality and quantification. Concurrently, novel PET radiotracers beyond standard ^18F-FDG (fluorodeoxyglucose) are emerging, targeting specific tumor features: for example, PSMA ligands for prostate cancer, FAPI ligands for fibroblast-rich tumors, somatostatin analogues (DOTATATE) for neuroendocrine tumors, FLT for proliferation, and amino-acid probes for brain and prostate cancers. These tracers often detect lesions that FDG misses. Quantitative PET biomarkers have advanced from simple SUVs (standardized uptake values) to volumetric measures (metabolic tumor volume, total lesion glycolysis) and high-dimensional radiomic features. Artificial intelligence (AI) and deep-learning tools now enable automated tumor segmentation, noise reduction, and prognostic modeling from PET images. Clinically, extensive evidence shows PET/CT improves staging and response assessment in major cancers. For example, PSMA PET/CT detects bone metastases in prostate cancer with ~98% sensitivity versus ~85% for traditional bone scintigraphy, and FDG PET/CT upstages breast and lung cancers in a significant fraction of cases. Compared to conventional imaging (CT, MRI, bone scan), PET/CT often demonstrates higher sensitivity and comparable specificity for nodal and distant metastases. PET/MRI may further improve lesion detection in selected cancers while reducing radiation dose. Workflow improvements from total-body PET and AI can accelerate scans and reduce dose. Cost-effectiveness studies suggest PET/CT can be economically justified by avoiding unnecessary biopsies or treatments, although access and reimbursement vary. Radiation dose and tracer safety remain important; FDA approvals exist for many tracers (e.g. ^68Ga-PSMA-11, ^18F-DCFPyL, ^68Ga-DOTATATE) while novel agents (e.g. FAPI) are investigational. This comprehensive review synthesizes recent literature and guidelines (SNMMI, EANM, NCCN) to provide an updated analysis of PET/CT innovations in oncology. It details technical advances, new tracers, quantitative imaging, and clinical evidence across major tumor types, compares PET/CT to other modalities, and discusses economic and regulatory considerations.
Positron emission tomography combined with computed tomography (PET/CT) has revolutionized cancer imaging by integrating metabolic or molecular functional information with high-resolution anatomical localization. Historically, the ^18F-FDG tracer (a glucose analogue) dominated PET oncology, due to the high glucose metabolism of many tumors. FDG PET/CT is well established for staging, restaging, and therapy response assessment in cancers such as lymphoma, lung, head/neck, and others. However, FDG has limitations: low uptake in certain tumor types (e.g. prostate, well-differentiated neuroendocrine, low-grade cancers) and false positives in inflammatory lesions. Over the past 5–10 years, innovations in PET detector technology and novel tracers have greatly expanded PET’s capabilities. Modern silicon-photomultiplier (SiPM) detectors and advanced reconstruction (including TOF and iterative algorithms) enhance spatial resolution and lesion contrast. Hybrid systems now include PET/MRI and total-body PET/CT, enabling new multiparametric imaging approaches. At the same time, a growing pipeline of radiopharmaceuticals targets specific tumor markers: e.g. PSMA ligands for prostate cancer; fibroblast activation protein inhibitors (FAPI) targeting tumor stroma; somatostatin receptor analogs (e.g. ^68Ga-DOTATATE) for neuroendocrine tumors; ^18F-FLT for proliferation; and amino-acid tracers (e.g. ^18F-FET, ^18F-fluciclovine) for brain and recurrent prostate cancers. These allow PET to be applied in a wider range of malignancies.
Quantification in PET/CT has likewise evolved. Simple metrics like SUV_max are augmented by volumetric measures (metabolic tumor volume, total lesion glycolysis) and textural radiomic features, which capture intratumoral heterogeneity. AI/deep-learning methods facilitate automated tumor delineation and extraction of complex image biomarkers for prognosis. Such advances promise more precise staging and earlier response assessment, aligning with personalized oncology.
Major clinical studies and meta-analyses report that these PET innovations lead to more accurate tumor staging and treatment monitoring across lung, breast, colorectal, lymphoma, prostate, head & neck, and other cancers. For example, PSMA PET/CT detects prostate cancer metastases with substantially higher sensitivity than conventional imaging. Similarly, FDG PET/CT often outperforms CT or MRI alone in head/neck and lung cancer staging. These improvements are recognized in guidelines: the NCCN and EANM/SNMMI endorse PET/CT in specific indications (e.g. PSMA PET for high-risk prostate cancer, FDG PET/CT for stage IIB+ breast and lung cancer).
This review systematically examines recent peer-reviewed literature (past ~5 years), including primary studies, meta-analyses, and major guidelines, on innovations in PET/CT imaging for oncology. Emphasis is placed on technological developments (digital PET, TOF, new detectors, PET/MRI), novel tracers (PSMA, FAPI, DOTATATE, FLT, etc.), and quantitative biomarkers (SUV, metabolic tumor volume, radiomics, AI). We analyze clinical evidence of how these advances improve accuracy in tumor staging and monitoring across key cancers, compare PET/CT to other modalities, and consider operational factors (cost, workflow) and safety/regulatory issues.
METHODS
A comprehensive literature search was performed focusing on PET/CT in oncology. Databases searched included PubMed, MEDLINE, and Google Scholar, targeting articles from 2018–2025. Keywords used included “PET/CT”, “digital PET”, “time-of-flight”, “PET/MRI”, “PSMA PET”, “FAPI PET”, “DOTATATE PET”, “FLT PET”, “radiomics PET”, “SUV PET”, “metabolic tumor volume”, “radiomics”, “AI”, “tumor staging”, “treatment response”, and specific cancer types (lung, breast, colorectal, lymphoma, prostate, head & neck). Priority was given to recent systematic reviews, meta-analyses, and multicenter trials, as well as clinical practice guidelines from NCCN, EANM/SNMMI, and SNMMI. References in key articles were mined for additional sources. Information was extracted on technological parameters, tracer properties, quantitative methods, and diagnostic performance metrics (sensitivity, specificity, accuracy) where available. The findings were synthesized into thematic sections covering technology, tracers, quantification, evidence by cancer type, comparisons, and practical considerations.
RESULTS/FINDINGS
Technological Advances in PET
Detector and Reconstruction Innovations: New PET/CT scanners increasingly use digital silicon photomultiplier (SiPM) detectors rather than traditional photomultiplier tubes. SiPMs provide faster timing resolution and higher photon detection efficiency, which together with advanced time-of-flight (TOF) and optimized crystal geometries significantly improve image quality. For example, modern digital PET/CT achieves better spatial resolution and sensitivity, resulting in clearer imaging of small lesions and lower image noise. Iterative reconstruction algorithms, including point-spread-function and block-sequential regularized expectation maximization, further enhance contrast. The combined effect is that digital PET permits either shorter acquisition times or lower tracer dose for comparable image quality. In one study, AI-based denoising algorithms allowed halving PET acquisition time on a digital PET/CT while maintaining lesion detectability.
Time-of-Flight (TOF): TOF PET measures the slight timing difference between coincident gamma detections, improving localization of annihilation events. Advanced TOF systems (with resolution ~200 ps or better) improve signal-to-noise and contrast recovery, especially in larger patients. Recent reviews note that improved TOF and extended axial fields-of-view are key to current digital PET systems, enabling gains in sensitivity.
Hybrid PET/MRI: Integrating PET with MRI combines PET’s functional imaging with MRI’s superior soft-tissue contrast and non-ionizing imaging. PET/MRI scanners use simultaneous acquisition, providing inherently aligned PET and MR images. Studies suggest PET/MRI can detect additional lesions and reduce radiation dose (no CT component) compared to PET/CT. For instance, a cohort study found that PET/MRI upstaged disease in a significant percentage of patients and improved lesion conspicuity, especially in liver and brain metastases, over PET/CT. PET/MRI was shown to improve image quality in gastric cancer staging and may better define tumor extent in anatomically challenging regions. However, PET/MRI is costlier and less available; its use is growing in academic centers.
Total-Body PET: The recent advent of long-axial-field-of-view (LAFOV) “total-body” PET/CT scanners (e.g. uEXPLORER) covers >1.5 m of patient length in one bed position. These devices have ultra-high sensitivity, enabling whole-body dynamic imaging, rapid scans (minutes or seconds), or ultra-low injected dose. By 2025, over 50 LAFOV PET systems were deployed worldwide. Early reports demonstrate that total-body PET/CT greatly enhances lesion detectability and allows kinetic modeling of tracer distribution, potentially improving quantification and therapy monitoring. This technology is poised to impact pharmacokinetic studies and total-body tumor burden assessment.
Spectral CT and Iterative Techniques: PET/CT scanners now often incorporate dual-energy or spectral CT capabilities. Dual-energy CT adds material decomposition (iodine maps, etc.), which enhances lesion characterization and can further improve attenuation correction for PET. Studies have shown that spectral CT improves cancer detection (e.g. higher sensitivity for small lesions) and can reduce follow-up imaging needs. Advances in CT reconstruction and detector design complement PET improvements to yield overall better multimodal imaging.
In summary, the latest hybrid systems leverage optimized detectors, TOF, and sophisticated reconstruction to yield PET images with higher resolution and sensitivity. These technical strides increase diagnostic confidence and facilitate quantitative accuracy (e.g. more reliable SUVs) which underpin advanced analyses.
NOVEL PET RADIOTRACERS
Beyond FDG, multiple targeted PET tracers have expanded oncology imaging:
Summary of Tracer Comparisons:
|
Tracer |
Target |
Main Use |
Notes |
|
^18F-FDG |
Glucose metabolism |
Broad oncology (lymphoma, lung, etc) |
High sensitivity for most carcinomas; limited in low-grade tumors; abundant supporting evidence. |
|
^68Ga-PSMA-11/^18F-DCFPyL |
PSMA on prostate cancer cells |
Prostate cancer staging/recurrent |
Superior nodal/bone mets detection; guideline-endorsed in high-risk PCa. |
|
^68Ga-/^18F-FAPI |
Fibroblast activation protein (stroma) |
Pancreas, GI, sarcoma, others |
Often outperforms FDG in certain tumors (e.g. PDAC); investigational. |
|
^68Ga-DOTATATE/-DOTATOC |
Somatostatin receptor (SSTR2) |
Neuroendocrine tumors |
High sensitivity in NETs; imaging heterogeneity; FDA-approved; guides PRRT therapy. |
|
^18F-FLT |
Thymidine kinase (DNA synthesis) |
Proliferation imaging |
May predict response in lymphoma, lung; not routine. |
|
^18F-fluciclovine |
Amino acid transporter (LAT1) |
Recurrent prostate cancer |
FDA-approved for post-treatment recurrence; moderate sensitivity (PSMA better). |
|
^11C-Methionine / ^18F-FET |
Amino acids (LAT1) |
Brain tumors (glioma) |
Superior to FDG in brain; used in Europe for tumor delineation. |
|
Others (e.g. ^89Zr-trastuzumab for HER2, ^18F-FES for ER) |
Various receptors |
Research and theranostics |
Evolving probes for targeted imaging; outside scope here. |
Table 1 (above) summarizes key PET tracers, their targets, typical applications, and comparative performance.
QUANTITATIVE IMAGING AND BIOMARKERS
Standardized Uptake Value (SUV): SUV remains the standard semi-quantitative measure of tracer uptake (normalized by injected dose and body weight or lean body mass). It enables comparison of lesions over time or between patients. However, absolute SUV values can vary with scanner, acquisition, reconstruction, and patient factors. Harmonization efforts (e.g. EANM research protocols) aim to standardize SUV. Digital PET and better reconstructions improve SUV accuracy and repeatability.
Volumetric Metrics – Metabolic Tumor Volume (MTV) and Total Lesion Glycolysis (TLG): Beyond SUV_max, volumetric PET parameters quantify the extent of metabolically active tumor. MTV is the volume of tumor above an uptake threshold; TLG = MTV × SUV_mean. These correlate with prognosis. For instance, high FDG-MTV on baseline scans predicts poorer survival in lymphoma and lung cancer. One review noted that baseline whole-body MTV from FDG-PET is a powerful prognostic biomarker in lymphoma. MTV and TLG integrate tumor burden and metabolic activity, providing richer information than single-voxel SUV. They also feed into radiomic models.
Radiomics: Radiomic analysis extracts a high-dimensional set of features (texture, shape, intensity distribution, heterogeneity measures) from PET (and CT) images. These features can capture intra-tumoral heterogeneity and microenvironment characteristics. Early studies show PET radiomics can predict genotype, histology, and outcomes in cancers. For example, FDG-PET radiomics have been used to noninvasively predict EGFR mutation status in lung cancer. In diffuse large B-cell lymphoma (DLBCL), whole-body MTV combined with gene expression improved risk stratification. In lung cancer, deep learning models using PET/CT radiomics have achieved predictive performance on par with expert evaluation in staging and survival prediction.
AI and Deep Learning: Artificial intelligence augments PET image analysis in two main ways. First, AI-based reconstruction and denoising improves image quality, as described above (halving scan time via denoising). Second, AI algorithms perform automated tumor segmentation and prognostic modeling. Convolutional neural networks have been trained to delineate tumors on PET, reducing inter-reader variability. AI-based radiomics pipelines can integrate PET and CT features for outcome prediction (e.g., survival or treatment response). A 2023 systematic review of PET/CT radiomics in NSCLC found many AI models with accuracy comparable to experts in tasks like malignancy classification and staging. However, these methods are in research stages and require validation.
In practice, quantitative biomarkers guide treatment decisions. For example, PET SUVs are used with PERCIST or Deauville criteria to assess response in solid tumors and lymphoma. MTV reduction early after therapy can predict pathological response. Radiomic signatures and AI prognostic models are emerging as companion diagnostics.
Clinical Impact: Tumor Staging and Treatment Monitoring
Numerous studies demonstrate that advanced PET/CT improves staging accuracy and therapy monitoring across cancer types:
Across these cancers, comparative studies consistently show PET/CT adds sensitivity. For example, in a meta-analysis of head/neck cancer, PET/CT sensitivity for extranodal extension was ~80% versus ~58% for CT/MRI. In prostate cancer, PSMA PET/CT sensitivity (~98%) far exceeds bone scan (~85%). In breast cancer, PET/CT has a higher negative predictive value for nodal disease than ultrasound or MRI.
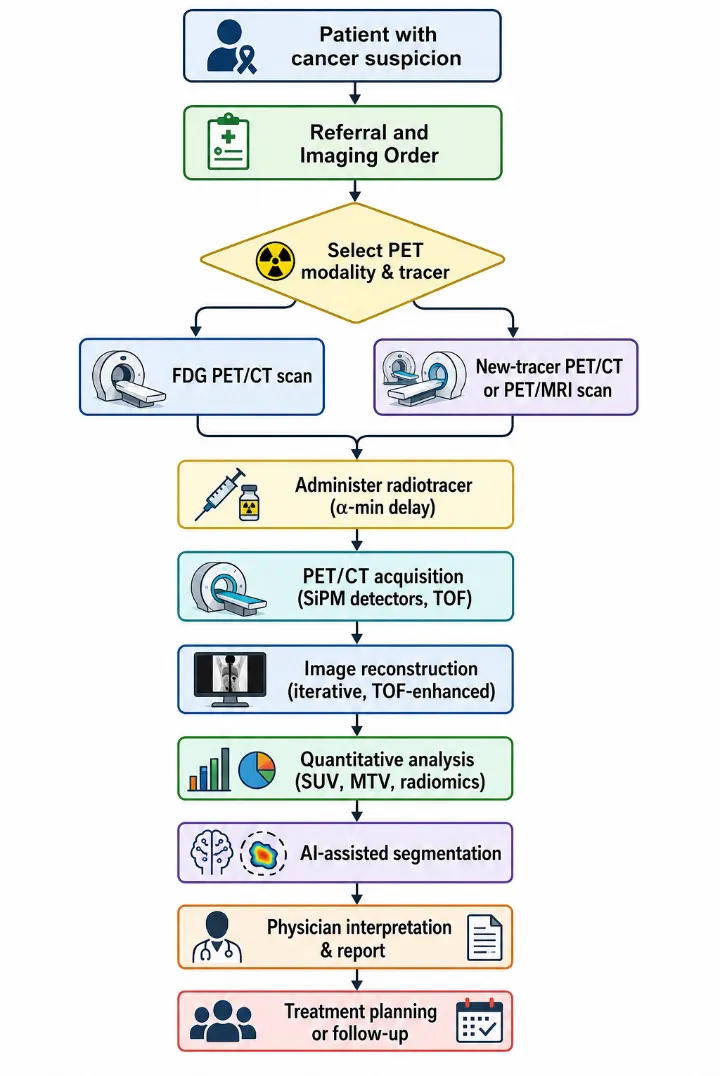
Figure 1 (above) outlines a typical PET imaging workflow – from patient selection and tracer injection through image acquisition, reconstruction, quantification (SUV/MTV/radiomics), and interpretation.
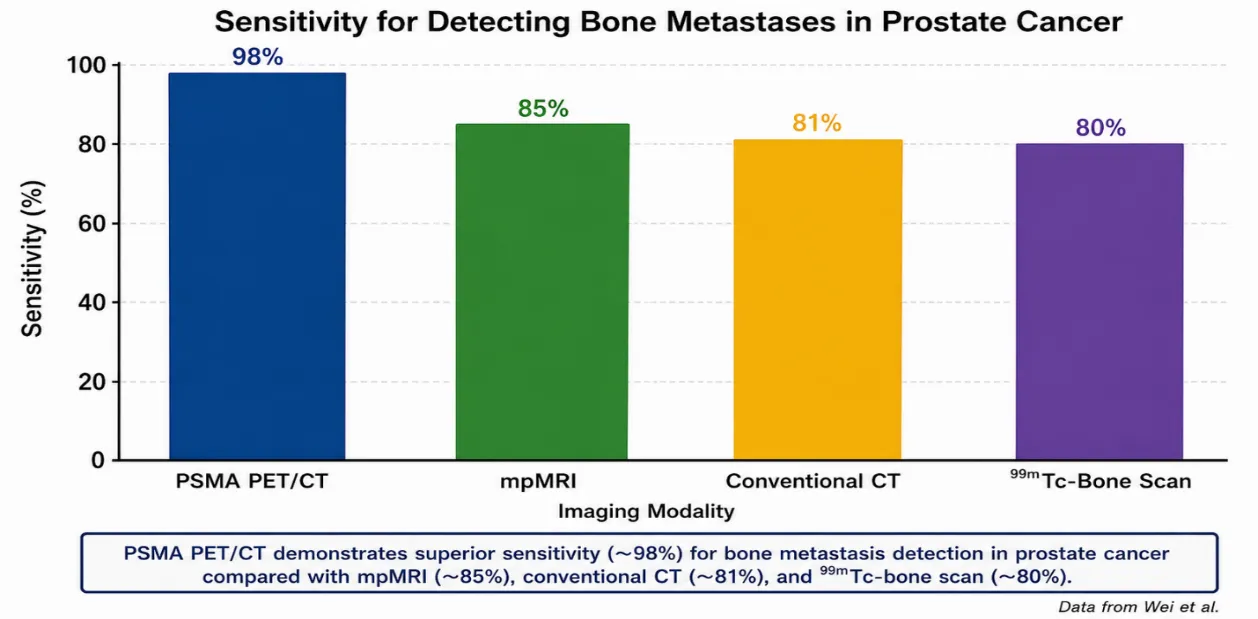
(Figure 2. Sensitivity of different imaging modalities for detecting bone metastases in prostate cancer. PSMA PET/CT far outperforms CT/MRI/bone scan.)
Diagnostic Accuracy (Example): As an illustration, Figure 2 compares sensitivity for detecting bone metastases in prostate cancer using different modalities. PSMA PET/CT achieved ~98% sensitivity versus ~80–85% for mpMRI, conventional CT, or 99mTc-bone scan, reflecting its superior lesion detection.
Comparison with Other Modalities and Emerging Techniques
Versus CT/MRI Alone: PET/CT consistently adds functional information that alters staging. In many cancers, PET/CT upstages or downstages disease relative to CT or MRI alone. For example, FDG PET/CT finds bone mets missed by bone scan and small nodal disease missed by CT, while PET/MRI can detect brain metastases at no extra dose. Whole-body MRI (with diffusion) is an emerging competitor, particularly for bone metastasis detection, but PET/CT remains generally more sensitive for early bony and visceral metastases. In lung cancer, meta-analyses report PET/CT sensitivity ~10–20% higher than CT for nodal/distant disease. A recent systematic review in recurrent prostate cancer showed PSMA PET/CT outperforms multiparametric MRI and CT in overall accuracy (accuracy ~0.89 vs 0.79 vs 0.72).
PET/MRI: As noted, PET/MRI offers similar or slightly improved staging compared to PET/CT in selected cases. A head-to-head study in cervical cancer found PET/MRI yielded higher image quality and lesion conspicuity than PET/CT. For cancers where radiation dose is a concern (pediatrics, young patients), PET/MRI reduces CT exposure. However, MRI scans take longer and access is limited, so PET/CT remains standard for most adult oncology.
Emerging Modalities: Beyond PET and MRI, other techniques like radiolabeled antibodies (immunoPET) and new radioligand therapies (theranostics) are developing. For instance, ^89Zr-trastuzumab PET can image HER2-positive tumors. While outside classic imaging scope, these highlight the trend of personalized molecular imaging.
Cost-Effectiveness and Workflow Impact
PET/CT is more expensive than standalone CT, and novel tracers add costs. However, many studies model cost-effectiveness by factoring in avoided procedures or improved outcomes. For instance, using FDG PET/CT in suspected lung cancer can prevent futile thoracotomies by revealing metastases, which can offset the scan cost. Economic analyses in head/neck and lung cancer often find PET/CT to be cost-effective, especially when influencing major treatment decisions. PSMA PET/CT for prostate cancer has been evaluated: early models suggest its high sensitivity may justify cost by enabling targeted treatments; however, formal cost-effectiveness depends on long-term outcomes data. Workflow efficiencies are also relevant: faster digital PET/CT and AI tools can increase patient throughput. Total-body PET dramatically reduces scan time (to a few minutes), which could greatly improve clinical workflow and reduce per-patient cost over time.
Reimbursement is a limiting factor. In the US, many indications require prior authorization. In Europe, PET/CT reimbursement varies by country and indication. Recent FDA approvals of new tracers (PSMA, DOTATATE) have improved access in the US. Ultimately, as evidence grows that PET/CT changes management, guideline inclusion and insurer coverage are expected to expand.
Safety and Regulatory Considerations
Radiation Dose: A typical PET/CT imparts ~15–25 mSv (PET ~7–14 mSv; CT ~5–10 mSv depending on protocol). This is higher than a CT alone but often justified by clinical benefit. Advances allow dose reduction: digital PET enables lower injected activity, and PET/MRI eliminates the CT dose entirely. Radiation safety guidelines (ALARA) govern tracer doses. Patients are monitored for rare side-effects of radiotracers (generally mild, such as contrast reactions or anxiety).
Tracer Safety and Regulation: Most PET radiotracers are used under strict regulatory frameworks. FDA has approved several oncology PET agents: ^18F-FDG, ^68Ga-DOTATATE, ^18F-fluciclovine (Axumin), ^68Ga-PSMA-11, ^18F-DCFPyL (Piflufolastat), among others. Each approval followed demonstration of safety (no significant toxicity) and efficacy. For example, ^68Ga-PSMA-11 was FDA-approved for prostate cancer in 2020 after trials in ~960 men. ^68Ga-DOTATATE was FDA-approved for NET imaging. Unapproved tracers (like many new FAPI variants) are used only in clinical trials or compassionate use under INDs. Manufacturing of PET tracers must follow Good Manufacturing Practices, and imaging sites require nuclear licenses.
Pediatric and Special Populations: Use of PET/CT in children is more cautious due to lifetime cancer risk from radiation. Indications are limited (e.g. pediatric lymphoma, sarcoma) where the benefit outweighs risk. New lower-dose protocols and tracers help mitigate this.
Regulatory Guidelines: International practice guidelines (EANM/SNMMI, SNMMI AUC) provide standards for PET imaging procedures and indications. For example, SNMMI/EANM procedure standards outline acquisition protocols for PSMA PET/CT, including patient prep and reporting criteria. Many guidelines stress the importance of adhering to protocols (e.g. PERCIST criteria, Deauville criteria) to ensure consistent use of PET in clinical trials and practice.
DISCUSSION
The last decade has seen PET/CT evolve from a specialized test to a cornerstone of precision oncology. Technological innovations have continuously improved image quality, making PET/CT faster, sharper, and more quantitative. The transition to digital detectors and TOF systems has nearly doubled PET sensitivity in some cases, directly translating to better small-lesion detection and potential dose reduction. Hybrid imaging (PET/CT and PET/MRI) provides a holistic view of cancer, blending metabolic and morphologic data. Total-body PET is poised to further revolutionize workflow and whole-body kinetic analysis.
Simultaneously, the expansion of PET tracers means that nearly every major cancer type can be addressed: PSMA for prostate, SSTR for NETs, amyloid markers for brain metastases, etc. The FAPI class exemplifies a new paradigm – imaging the tumor microenvironment – which may complement tumor-centric tracers. Each new tracer is backed by impressive clinical data, often showing higher lesion uptake and detection rates than FDG in its niche.
Quantitative PET has become more robust: SUVs can now be meaningfully compared across time and centers due to stricter protocols and scanner calibration. Moreover, volumetric and radiomic biomarkers extend PET’s role from detection to characterization. SUV_max, long used, is giving way to MTV and TLG as prognostic indicators, and radiomic features that correlate with genomics are emerging. Integration of AI for segmentation and analysis addresses the historical bottleneck of manual ROI delineation, promising reproducibility and scalability.
Clinically, the incremental benefits of PET/CT over older imaging are well documented. Multicenter trials and meta-analyses consistently find that hybrid PET/CT alters staging in a substantial minority of cases, often leading to a change in management (avoiding futile surgery, redirecting therapy). For treatment monitoring, PET/CT provides earlier and more specific assessment of response than size-based criteria. For example, in lymphoma, an interim PET scan after 2 cycles can identify non-responders much earlier than conventional imaging, allowing treatment intensification.
From a health-systems perspective, while PET/CT is costlier upfront, it can improve cost-effectiveness by guiding appropriate therapy. Some cost-effectiveness models (e.g. in lung cancer) have shown net savings by preventing unnecessary procedures when PET/CT is used. As scanners become faster and software automates analysis, per-patient throughput will increase, improving cost efficiency.
However, barriers remain: limited access in some regions, high fixed costs of equipment, and regulatory hurdles for new tracers. Ongoing trials (e.g. randomized studies of PSMA PET vs standard imaging in management pathways) are needed to show outcome benefits. Also, standardization of advanced PET (e.g. radiomics workflows) is still immature. Finally, addressing false positives (inflammation, benign causes of uptake) requires clinician awareness and possibly dual-tracer strategies.
Clinical Implications
PET/CT innovations are already changing oncology practice. Clinicians should be aware of emerging tracers: for example, referring intermediate-risk prostate cancer patients for PSMA PET/CT can uncover metastatic disease earlier. PET/CT staging should be considered in breast cancer from stage IIB onward. Radiology and nuclear medicine teams should leverage PET/CT’s quantitative outputs (e.g. MTV) in multidisciplinary tumor boards when available. In radiotherapy planning, PET-defined tumor volumes are increasingly used for target delineation.
AI tools can enhance workflow: e.g. automated contouring and report drafting are under development, which may soon enter clinics. Departments upgrading to digital PET/CT will benefit from training on new imaging protocols that allow dose reduction. Cost discussions with administrators can now cite evidence that PET/CT often prevents expensive downstream procedures.
However, physicians must also consider pitfalls. New tracers may not yet be widely available or approved locally (FAPI, novel antibodies). Radiologists should be trained to interpret PET/MRI artifacts and gating issues. And in reporting PET/CT, standardized systems (Deauville, PERCIST) should be used where validated to improve reproducibility.
LIMITATIONS
This review is not a systematic review; relevant literature was selected based on relevance and recency, which may introduce selection bias. Some emerging topics (e.g. theranostic radioisotopes, very new tracers) are beyond scope. The fast-moving field means some cutting-edge data (e.g. 2025 conference abstracts) may not be captured. Quantitative performance metrics can vary between studies due to patient populations and methodologies, so cited values (e.g. sensitivities) are illustrative. Also, comparative imaging studies often involve small cohorts or retrospective designs, limiting generalizability. Cost-effectiveness analyses are region-specific and rely on many assumptions.
FUTURE DIRECTIONS
Future research should focus on:
(1) Large trials evaluating whether PET-driven management improves survival or quality-of-life (e.g. proPSMA trial style);
(2) Harmonization of quantification and radiomics across platforms to enable multicenter AI models;
(3) Development of new tracers for unmet needs (e.g. hypoxia PET, immune-cell imaging);
(4) Translation of PET/MRI and total-body PET into routine practice with cost-effective models;
(5) Radiation dose optimization especially for serial imaging;
(6) Health-services research on implementing PET into care pathways. Continued integration of PET/CT data with genomics and liquid biopsies holds promise for truly personalized oncology.
CONCLUSION
Advances in PET/CT technology and tracer chemistry have substantially improved cancer imaging. Digital PET detectors and hybrid imaging yield higher resolution, enabling detection of smaller metastases. A new generation of radiotracers provides sensitive, specific targeting of prostate, stromal, neuroendocrine, and other cancer processes. Quantitative imaging and AI promise more precise and reproducible biomarkers. Collectively, these innovations translate to more accurate tumor staging and treatment monitoring across malignancies, as reflected in recent guidelines. While challenges in cost and standardization remain, the trend is clear: PET/CT is moving toward ever-greater precision in oncology imaging.
ACKNOWLEDGMENTS
The authors thank the radiology and nuclear medicine library teams for assistance with literature searches. This work received no specific funding.
REFERENCES

Usama Asad*, Nabin Kumar Yadav, Asadullah, Ahsan Hafeez, Cymantha Robin, Aqib Naeem, PET-CT Innovations In Oncology For Accurate Tumor Staging And Treatment Monitoring, Int. J. Sci. R. Tech., 2026, 3 (6), 1615-1625. https://doi.org/10.5281/zenodo.20935805
 10.5281/zenodo.20935805
10.5281/zenodo.20935805