
We use cookies to ensure our website works properly and to personalise your experience. Cookies policy
Department of Pharmacology, Matoshri College of Pharmacy, Eklahare, Nashik-422105
Caffeine is one of the most widely consumed central nervous system (CNS) stimulants, traditionally administered through oral beverages and solid dosage forms. However, conventional oral delivery is often associated with delayed onset of action due to gastrointestinal absorption and first-pass metabolism. In recent years, alternative delivery systems such as oral and nasal sprays have emerged as promising strategies for rapid drug absorption and immediate pharmacological response. Caffeine spray represents a novel and innovative approach designed to bypass gastrointestinal limitations and deliver the drug directly through the buccal or nasal mucosa into systemic circulation. This review highlights the pharmacological profile of caffeine, its mechanism of CNS stimulation and the limitations of traditional dosage forms. It further explores the formulation strategies, absorption pathways, and advantages of caffeine spray systems in achieving rapid onset of action. Special emphasis is placed on applications in conditions requiring quick alertness, such as fatigue, drowsiness, and cognitive impairment. Additionally, challenges related to formulation stability, dose accuracy, and regulatory considerations are discussed. Overall, caffeine spray offers a promising, patient-friendly, and fast-acting alternative to conventional delivery systems, with potential applications in both therapeutic and lifestyle settings.
Caffeine is one of the most widely consumed psychoactive substances worldwide and is extensively recognized for its ability to enhance alertness, mood, and cognitive performance through stimulation of the central nervous system (CNS). It has long been used as an ergogenic aid, particularly in athletic and physically demanding environments, where it improves endurance, reduces perceived fatigue, and enhances overall performance. Importantly, caffeine remains a legally accepted stimulant and is not included in the prohibited substances list of the World Anti-Doping Agency (WADA), making it a preferred choice among athletes and individuals seeking performance enhancement. Over the past decade, numerous studies have evaluated its pharmacological and ergogenic effects, emphasizing its efficacy at lower doses that primarily target CNS activity while minimizing peripheral side effects such as cardiovascular stimulation [1-2]. Traditionally, caffeine has been administered through oral routes such as coffee, tea, energy drinks, and pharmaceutical formulations including tablets and capsules. Following oral administration, caffeine is absorbed mainly through the gastrointestinal tract, with onset of action dependent on gastric emptying time and hepatic first-pass metabolism. Although oral delivery provides high bioavailability, it is often associated with a delayed onset of pharmacological action, typically requiring 20–45 minutes to achieve peak plasma concentration. This delay limits its effectiveness in situations requiring rapid stimulation, such as emergency response, shift work, or competitive sports performance [2]. To overcome these limitations, recent research has focused on the development of alternative drug delivery systems aimed at improving the rate and efficiency of caffeine absorption. Novel delivery approaches such as caffeinated chewing gums, gels, buccal tablets, lozenges, and transdermal systems have been explored to enhance absorption through non-gastrointestinal pathways. Among these, oromucosal and intranasal delivery systems have gained significant attention due to their ability to bypass first-pass metabolism and facilitate rapid drug absorption directly into systemic circulation. These routes offer the additional advantage of potential direct nose-to-brain transport via olfactory and trigeminal neural pathways, enabling faster CNS stimulation compared to conventional oral methods [2-3]. In particular, caffeine sprays administered either intranasally or via the oromucosal route represent a promising and innovative approach for rapid CNS activation. These formulations deliver caffeine in the form of fine aerosols, allowing absorption through highly vascularized mucosal surfaces and potentially enabling immediate pharmacological effects. Preclinical studies have demonstrated that intranasal delivery can result in higher concentrations of caffeine in cerebrospinal fluid and brain tissues compared to oral administration, suggesting enhanced efficiency of CNS targeting. Additionally, early human studies have reported a quicker subjective perception of alertness following spray administration, although pharmacokinetic variability and limited clinical evidence remain challenges [3]. Despite the growing interest in caffeine spray systems, several gaps persist in understanding their full therapeutic potential. Variability in formulation techniques, differences in delivery devices, and limited large-scale clinical trials contribute to inconsistencies in reported outcomes. Furthermore, concerns related to dosing accuracy, mucosal irritation, and long-term safety must be addressed before widespread clinical or commercial adoption. Therefore, this review aims to critically evaluate the current advancements in caffeine spray delivery systems, focusing on their pharmacokinetic and pharmacodynamic profiles, mechanisms of rapid CNS stimulation, and comparative effectiveness with traditional delivery methods, while also identifying key challenges and future research directions [4].
MECHANISM OF ACTION
Caffeine exerts its primary pharmacological effects through antagonism of adenosine receptors in the central nervous system (CNS). Due to its amphiphilic nature (both lipid- and water-soluble), caffeine readily crosses the blood–brain barrier and distributes widely throughout body tissues. It acts as a non-selective antagonist of all four adenosine receptor subtypes (A1, A2A, A2B, and A3), with particular emphasis on A1 and A2A receptors. Under normal physiological conditions, adenosine functions as an inhibitory neuromodulator that promotes sleep, suppresses arousal, and reduces neuronal activity. By competitively inhibiting adenosine binding, caffeine prevents these inhibitory effects, resulting in increased neuronal firing, enhanced neurotransmitter release (including dopamine, norepinephrine, and glutamate), and improved alertness, vigilance, and cognitive performance. The antagonism of A2A receptors, especially in dopaminergic regions of the brain, is largely responsible for the wakefulness-promoting effects of caffeine [4]. Beyond the CNS, adenosine receptors are distributed throughout peripheral tissues, contributing to caffeine’s systemic effects. In the cardiovascular system, blockade of A1 receptors in cardiac tissue leads to positive inotropic and chronotropic effects, thereby increasing heart rate and myocardial contractility. Additionally, caffeine stimulates the release of catecholamines such as adrenaline, further enhancing sympathetic nervous system activity. At the vascular level, caffeine exhibits complex and sometimes opposing actions. It can induce vasodilation by inhibiting vascular adenosine receptors and stimulating nitric oxide release from endothelial cells, while simultaneously promoting vasoconstriction through increased sympathetic tone. The net vascular response varies depending on individual sensitivity, dose, and habitual caffeine consumption. Acute intake in non-habitual users may increase systolic blood pressure by approximately 5–10 mmHg, whereas regular consumers often develop tolerance to these effects [5-6].
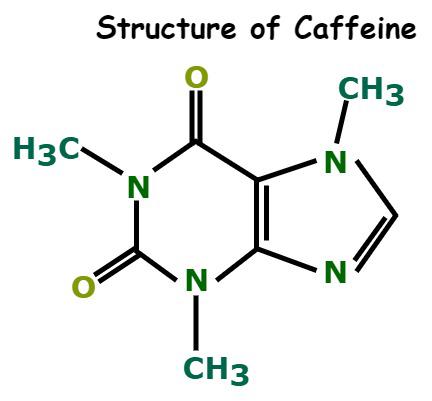
Figure 1: Chemical Structure of Caffeine
Caffeine also influences respiratory and renal physiology. It enhances respiratory drive by increasing the sensitivity of the medullary respiratory center to carbon dioxide, leading to improved ventilation and diaphragmatic contractility. This property has clinical relevance in neonatal apnea management. In the kidneys, caffeine promotes diuresis by increasing renal blood flow, glomerular filtration rate, and inhibiting sodium reabsorption, resulting in increased urine output. Additionally, caffeine stimulates gastric acid secretion and gastrointestinal motility, which may contribute to digestive effects and, in some individuals, gastric discomfort [6-8]. At higher concentrations, caffeine exhibits additional molecular mechanisms that further contribute to its stimulatory profile. It inhibits phosphodiesterase (PDE) enzymes, leading to increased intracellular levels of cyclic adenosine monophosphate (cAMP), thereby amplifying signal transduction pathways associated with energy metabolism and neurotransmission. Furthermore, caffeine facilitates the release of calcium ions from intracellular stores such as the sarcoplasmic and endoplasmic reticulum, enhancing muscle contraction and neurotransmitter release. At very high doses, caffeine may also exert weak antagonistic effects on gamma-aminobutyric acid (GABAA) receptors, reducing inhibitory neurotransmission and further promoting CNS excitation [9-10]. Collectively, these mechanisms adenosine receptor antagonism, catecholamine release, phosphodiesterase inhibition, and intracellular calcium mobilization—contribute to caffeine’s multifaceted pharmacological profile. These actions explain its widespread use as a central nervous system stimulant, its ergogenic benefits in enhancing physical and cognitive performance, and its potential therapeutic applications. Importantly, in the context of novel delivery systems such as caffeine sprays, rapid absorption through nasal or oromucosal routes may further potentiate these mechanisms by accelerating drug delivery to the brain and minimizing metabolic delays associated with oral administration [10].
Pharmacology of Caffeine
Caffeine (1,3,7-trimethylxanthine) is a naturally occurring methylxanthine alkaloid widely consumed for its central nervous system (CNS) stimulant properties. It exhibits a complex pharmacological profile involving both central and peripheral mechanisms. The primary mode of action of caffeine is the non-selective antagonism of adenosine receptors, particularly A1 and A2A subtypes. Under physiological conditions, adenosine acts as an inhibitory neuromodulator that suppresses neuronal excitability and promotes sleep. By competitively inhibiting adenosine binding, caffeine removes this inhibitory tone, resulting in enhanced neuronal activity, increased release of excitatory neurotransmitters such as dopamine and norepinephrine, and improved alertness, mood, and cognitive performance. The blockade of A2A receptors in dopaminergic regions is particularly significant in mediating wakefulness and psychostimulant effects [11]. In addition to adenosine receptor antagonism, caffeine influences intracellular signaling pathways. At moderate to high concentrations, it inhibits phosphodiesterase (PDE) enzymes, leading to an accumulation of cyclic adenosine monophosphate (cAMP). Elevated cAMP levels enhance cellular metabolic activity and amplify neurotransmitter signaling pathways, contributing to increased energy availability and improved neuromuscular performance. Furthermore, caffeine facilitates the mobilization of intracellular calcium ions from the sarcoplasmic and endoplasmic reticulum, which enhances muscle contraction and neurotransmitter release. These actions are particularly relevant in skeletal and cardiac muscle, where caffeine improves contractility and endurance capacity [12-14]. Caffeine also exerts mild antagonistic effects on gamma-aminobutyric acid (GABAA) receptors at higher concentrations, thereby reducing inhibitory neurotransmission and further contributing to CNS stimulation. This combined effect of increased excitatory signaling and reduced inhibitory tone underlies caffeine’s well-known stimulatory and psychoactive properties. In the cardiovascular system, caffeine increases heart rate and myocardial contractility through adenosine receptor blockade and enhanced catecholamine release. It may also cause transient increases in blood pressure, particularly in non-habitual users, due to peripheral vasoconstriction and sympathetic activation [15]. Pharmacokinetically, caffeine is rapidly and almost completely absorbed following oral administration, with bioavailability approaching 100%. Peak plasma concentrations are typically achieved within 30–60 minutes, although this may vary depending on formulation and physiological factors. Caffeine is widely distributed throughout the body, readily crossing the blood–brain barrier and placenta. It undergoes extensive hepatic metabolism, primarily via the cytochrome P450 enzyme CYP1A2, producing active metabolites such as paraxanthine, theobromine, and theophylline, which contribute to its pharmacological effects. Elimination occurs mainly through renal excretion, with a half-life ranging from 3 to 7 hours in healthy adults, though this can be influenced by factors such as age, pregnancy, liver function, and genetic variability [16]. Overall, the pharmacological profile of caffeine is characterized by its rapid absorption, extensive distribution, and multifaceted mechanisms of action involving receptor antagonism, enzyme inhibition, and intracellular signaling modulation. These properties make caffeine an effective CNS stimulant with applications in enhancing alertness, cognitive function, and physical performance. Importantly, in the context of novel delivery systems such as nasal and oromucosal sprays, the pharmacokinetic advantages of bypassing first-pass metabolism may further enhance the onset and intensity of these pharmacological effects, making caffeine a promising candidate for rapid-action CNS stimulation [17-19].
Conventional Route of Caffeine Delivery
Caffeine is most commonly administered through conventional oral routes, including beverages such as coffee, tea, soft drinks, and energy drinks, as well as pharmaceutical formulations like tablets and capsules. These methods remain the most widely accepted and utilized forms of caffeine consumption across both general populations and clinical or research settings. Following oral administration, caffeine is rapidly absorbed from the gastrointestinal (GI) tract, with approximately 99% of the administered dose absorbed within 30–45 minutes. This high absorption efficiency contributes to its near-complete bioavailability and predictable pharmacokinetic profile [20]. In addition to traditional beverages and solid dosage forms, other oral formulations such as caffeinated chewing gums, gels, and bars have been developed to provide relatively faster onset of action. These formulations allow partial absorption through the buccal mucosa, thereby slightly reducing the time required to reach peak plasma concentrations compared to conventional tablets or beverages. However, despite this advantage, a significant portion of caffeine is still swallowed and absorbed through the gastrointestinal tract, resulting in overall bioavailability comparable to other oral dosage forms [21]. Despite their widespread use, conventional oral routes of caffeine administration are associated with several pharmacokinetic limitations. One of the primary drawbacks is the delayed onset of action, as caffeine typically requires 20–30 minutes to achieve noticeable plasma concentrations and pharmacological effects. This delay is largely attributed to gastric emptying time and intestinal absorption processes. Furthermore, caffeine undergoes first-pass metabolism in the liver, primarily via the CYP1A2 enzyme, which can lead to inter-individual variability in plasma concentrations and therapeutic response. Factors such as age, genetic polymorphisms, diet, and liver function can further influence this variability [22]. Another limitation of oral caffeine delivery is its reduced effectiveness under certain physiological conditions. For instance, during intense physical activity or stress, splanchnic blood flow to the gastrointestinal tract is decreased, which can impair drug absorption and delay onset of action. This limitation is particularly relevant in sports performance or emergency scenarios where rapid CNS stimulation is required. Additionally, gastrointestinal discomfort, including gastric irritation and increased acid secretion, may occur in some individuals following oral caffeine consumption [23-26]. Nevertheless, oral administration remains the most convenient, non-invasive, and socially acceptable method of caffeine intake. It is easy to use, widely available, and does not require specialized devices or training. Alternative oral approaches such as chewing gums, sublingual strips, and lozenges offer modest improvements in onset time but still face challenges related to dosing precision and variability in absorption. Overall, while conventional oral delivery systems are effective for routine use, their limitations in achieving rapid onset and consistent pharmacokinetic profiles have driven the development of novel delivery approaches such as intranasal and oromucosal caffeine sprays [27].
Novel Drug Delivery System: Spray (Aerosol)
The concept of spray-based drug delivery has emerged as an innovative and patient-compliant approach in modern pharmaceutical technology. This system offers a rapid, non-invasive, and convenient mode of administration that ensures precise dosing and enhanced therapeutic efficacy. Spray formulations are particularly advantageous for drugs requiring a fast onset of action or those significantly affected by first-pass metabolism. Among these, nasal and oromucosal sprays have gained considerable attention due to their ability to facilitate systemic delivery and target the central nervous system (CNS) effectively [28]. The nasal route of administration utilizes the highly vascularized nasal mucosa, providing a large surface area (approximately 160 cm²) for drug absorption and rapid entry into systemic circulation. More importantly, intranasal delivery enables a direct nose-to-brain pathway via the olfactory and trigeminal nerves, allowing drugs to bypass the blood–brain barrier and reach the CNS more efficiently [29–30]. This pathway has been extensively explored for delivering peptides, hormones, and CNS-active agents, and recent investigations have extended this application to caffeine for rapid neurostimulation. Intranasal spray systems offer several advantages, including avoidance of hepatic first-pass metabolism, rapid absorption, and quick onset of pharmacological action. Additionally, they support both local and systemic drug delivery and enable direct targeting of brain tissues through neuronal pathways [31]. However, this route also presents limitations such as restricted dose volume (typically 100–200 µL per nostril), potential mucosal irritation, enzymatic degradation, and variability in drug absorption due to pathological nasal conditions. To overcome these challenges, advanced formulation strategies involving mucoadhesive polymers, nanoemulsions, and microparticulate carriers have been developed to prolong nasal residence time and enhance bioavailability [32]. Oromucosal spray systems represent another promising alternative for rapid drug delivery. This route includes sublingual and buccal administration, where drugs are absorbed through the highly vascularized oral mucosa, bypassing gastrointestinal degradation and hepatic metabolism. Oromucosal sprays deliver the drug in the form of a fine mist that adheres to the mucosal surface, facilitating rapid systemic uptake [33]. This method has been successfully applied to drugs such as nitroglycerin, nicotine, and certain CNS-active agents, including caffeine. The advantages of oromucosal sprays include rapid onset of action due to rich blood supply, accurate dosing through metered systems, ease of self-administration, and suitability for emergency or on-the-go use [34]. Nevertheless, certain limitations persist, such as unpleasant taste, mucosal irritation, and variability in absorption influenced by saliva flow and pH conditions. To address these issues, formulation approaches like cyclodextrin inclusion complexes and the use of mucoadhesive excipients (e.g., chitosan, carbopol) have been employed to enhance drug solubility, stability, and retention time at the absorption site [35]. The successful development of spray-based delivery systems requires careful optimization of physicochemical and mechanical parameters. Critical formulation variables include droplet size (typically 50–150 µm), viscosity, spray angle, and mucosal permeability, all of which influence drug deposition and absorption efficiency [36]. Key formulation components generally comprise solvents such as water, ethanol, or propylene glycol to improve solubility; permeation enhancers like surfactants or cyclodextrins to facilitate mucosal transport; stabilizers and preservatives (e.g., benzalkonium chloride, EDTA, parabens) to ensure product stability; and mucoadhesive polymers to prolong contact time. Additionally, delivery systems incorporate propellants or mechanical pump devices to ensure uniform and reproducible dosing. Recent advancements in drug delivery technology have led to the development of nanoparticle-based sprays, liposomal carriers, and thermosensitive gels, which significantly enhance drug targeting, controlled release, and bioavailability. These next-generation systems hold great promise for improving patient compliance and therapeutic outcomes, particularly for CNS-active drugs like caffeine, where rapid onset and efficient brain targeting are critical [37].
Evidence from Clinical and Preclinical Studies
The concept of rapid central nervous system (CNS) stimulation through intranasal and oromucosal caffeine delivery is supported by a growing body of preclinical and limited clinical evidence. These studies primarily focus on evaluating pharmacokinetic (PK) and pharmacodynamic (PD) parameters, as well as the efficiency of nose-to-brain transport mechanisms. Preclinical investigations using animal models have provided strong evidence for direct drug transport from the nasal cavity to the brain. Studies conducted in rats and other species demonstrate that intranasally administered compounds can bypass the blood–brain barrier via olfactory and trigeminal nerve pathways, resulting in rapid drug delivery to the CNS [38]. Quantitative PK studies have shown that intranasal administration can achieve higher concentrations of drugs in brain tissue and cerebrospinal fluid compared to traditional systemic routes such as oral or intravenous delivery. These findings support the hypothesis that nasal delivery systems can significantly enhance the onset of CNS effects [39]. Further supporting evidence arises from comparative studies in animals, where intranasal delivery consistently demonstrates improved brain targeting efficiency. Parameters such as drug targeting efficiency (%DTE) and direct transport percentage (%DTP), derived from area-under-the-curve (AUC) ratios of brain to plasma concentrations, confirm preferential delivery to brain tissues [40]. Techniques such as brain microdialysis have enabled direct measurement of drug concentrations in extracellular fluid, providing robust evidence of rapid CNS penetration following intranasal administration [41]. In addition to conventional formulations, advanced delivery systems such as nanoparticles, solid lipid nanoparticles (SLNs), and nanostructured lipid carriers (NLCs) have been evaluated in preclinical models. These systems enhance drug stability, improve mucosal adhesion, and prolong residence time within the nasal cavity, thereby increasing drug bioavailability and CNS targeting efficiency [42]. Liposomal formulations have also demonstrated improved permeability and faster localization in brain regions such as the olfactory bulb following intranasal administration [43]. Despite the extensive preclinical evidence, clinical data on caffeine spray delivery remain limited and somewhat inconsistent. Human studies involving nasal and oromucosal caffeine sprays have reported a rapid subjective perception of alertness and improved cognitive performance within minutes of administration. However, objective pharmacokinetic measurements such as plasma caffeine concentration often show variability, suggesting that both systemic absorption and direct neural stimulation may contribute to the observed effects [44]. Comparative clinical studies indicate that alternative delivery systems such as caffeine chewing gum provide faster absorption than traditional oral formulations, yet still rely partially on gastrointestinal uptake. In contrast, nasal sprays have the potential to produce an even faster onset of action due to direct mucosal absorption and possible nose-to-brain transport, although this mechanism is not yet fully quantified in humans [45]. A major limitation in current clinical research is the lack of large-scale, randomized, placebo-controlled trials evaluating the efficacy and safety of caffeine sprays. Most available studies involve small sample sizes, short durations, and limited evaluation of long-term safety outcomes. Additionally, variability in formulation composition, spray devices, and dosing strategies makes it difficult to standardize results across studies [46]. Overall, while preclinical data strongly support the feasibility of intranasal and spray-based caffeine delivery for rapid CNS stimulation, clinical evidence remains preliminary. Further well-designed human studies are required to establish definitive pharmacokinetic profiles, optimize dosing strategies, and confirm both efficacy and safety for widespread therapeutic or performance-enhancing use [47].
Table 1: Anatomical and Histological Differences Between the Nasal Cavity of Mice, Rats, Rabbits, and Humans [34-36]
|
Parameter |
Mice |
Rats |
Rabbits |
Humans |
|
Bodyweight (kg) |
0.03 |
0.25 |
3 |
70 |
|
Nasal cavity volume (cm3) |
0.03 |
0.26 |
6 |
25 |
|
Nasal cavity surface area (cm²) |
2.89 |
13.4 |
61 |
160 |
|
Relative surface area (NCSA/NCV) (cm-1) |
96.3 |
51.5 |
10.2 |
6.4 |
|
Olfactory epithelium (% of NCSA) |
47 |
50 |
10 |
8 |
|
Olfactory epithelium (cm3) |
1.37 |
6.75 |
6 |
12.5 |
Nasal Structure
The human nasal cavity is a highly specialized anatomical structure that plays a crucial role in respiration, filtration, and drug absorption. It extends from the nostrils (anterior nares) to the nasopharynx and is divided into two symmetrical halves by the nasal septum. Each cavity measures approximately 12–14 cm in length and about 5 cm in height, providing a total surface area of nearly 160 cm², which is significantly enhanced by the presence of nasal turbinates [48]. The lateral walls of the nasal cavity contain three bony projections known as the inferior, middle, and superior turbinates (or conchae). These structures increase the surface area and create turbulent airflow, which enhances the contact of inhaled substances with the mucosal lining. This feature is particularly advantageous for intranasal drug delivery, as it promotes efficient deposition and absorption of administered formulations [49]. Functionally, the nasal cavity is divided into two main regions: the respiratory region and the olfactory region. The respiratory region constitutes the majority of the nasal cavity and is lined with pseudostratified ciliated columnar epithelium containing goblet cells. This region is responsible for warming, humidifying, and filtering inhaled air, and it also serves as the primary site for systemic drug absorption due to its rich vascularization [50]. In contrast, the olfactory region is located in the upper part of the nasal cavity and contains specialized olfactory receptor neurons. This region is of particular importance in nose-to-brain drug delivery, as it provides a direct neuronal pathway to the central nervous system via the olfactory bulb. Drugs deposited in this area can be transported along olfactory neurons, bypassing the blood–brain barrier and enabling rapid CNS targeting [51]. Additionally, the nasal cavity is innervated by the trigeminal nerve, which offers another pathway for drug transport to the brain. This dual pathway (olfactory and trigeminal) significantly enhances the potential of intranasal delivery systems for CNS-active agents such as caffeine [52]. The nasal mucosa is covered by a mucus layer that acts as a protective barrier, trapping foreign particles and pathogens. However, this mucus layer, along with mucociliary clearance mechanisms, can limit drug residence time and absorption. Therefore, formulation strategies often incorporate mucoadhesive agents to prolong contact time and improve drug uptake [53]. Overall, the unique anatomical and physiological features of the nasal cavity including large surface area, rich blood supply, and direct neuronal connections make it an ideal route for rapid drug delivery, especially for achieving fast central nervous system stimulation through innovative systems like caffeine nasal sprays [54].
Regulatory and Safety Issues Surrounding Caffeine Spray System
The development of caffein

Sakshi Bhagat*, Prathamesh Sargar, Caffeine Spray as A Novel Approach for Rapid Central Nervous System Stimulation, Int. J. Sci. R. Tech., 2026, 3 (4), 200-212. https://doi.org/10.5281/zenodo.19414966
 10.5281/zenodo.19414966
10.5281/zenodo.19414966