Severity: Warning
Message: Undefined array key "articleIDUniqueCode"
Filename: frontend/article.php
Line Number: 189
Severity: 8192
Message: substr(): Passing null to parameter #1 ($string) of type string is deprecated
Filename: frontend/article.php
Line Number: 189
Severity: Warning
Message: Undefined array key "articleIDUniqueCode"
Filename: frontend/article.php
Line Number: 190
Severity: 8192
Message: substr(): Passing null to parameter #1 ($string) of type string is deprecated
Filename: frontend/article.php
Line Number: 190
Severity: Warning
Message: Undefined array key "articleIDUniqueCode"
Filename: frontend/article.php
Line Number: 213
Severity: 8192
Message: substr(): Passing null to parameter #1 ($string) of type string is deprecated
Filename: frontend/article.php
Line Number: 213
Severity: Warning
Message: Undefined array key "articleIDUniqueCode"
Filename: frontend/article.php
Line Number: 214
Severity: 8192
Message: substr(): Passing null to parameter #1 ($string) of type string is deprecated
Filename: frontend/article.php
Line Number: 214

We use cookies to ensure our website works properly and to personalise your experience. Cookies policy
Severity: Warning
Message: Undefined array key "articleIDUniqueCode"
Filename: frontend/article.php
Line Number: 424
1School of Pharmacy, Abhilashi University, Chailchowk, Mandi (H.P)
2Maharish Markendeshwar deemed to be University Mullana, Haryana 133204.
New aff
Background: quercus leucotrichophora locally known as banjh oak by rural people of himalayas, banj oak (uttarakhand) and ban oak (himachal), belongs to family fagaceae. In the himalayas, the banjh oak can be found in elevations between 1500 and 2400 meters. The various parts of quercus leucotrichophoraare used to treat asthma, haemorrhage, gonorrhoea and dysentery. The seed (gallnut) of banjh oak is used to treat aphthous ulcers and restoring elasticity of uterine wall. The seeds of quercus leucotrichophora are traditionally used to cure snake bites. Aim: to establish and standardize the seeds of the plant for its macroscopic, microscopic and physicochemical characteristics along with qualitative tests. Materials and methods: the seeds were exposed to macroscopy, microscopy and qualitative study as per the ayurvedic pharmacopoeia of india. Results: the seeds of quercus leucotrichophora were found to be dicotyledon with two layers or surfaces. The weight of whole fruit was found to be 34.02±4.53 whereas, the weight of seed was 9.34±0.23. After drying and size reduction the power was of blackish yellow colour having moisture content7.233±0.0283%. The ash value determines the quantity of the inorganic material present in the drug which was found to be within the limits in present study. The average percentage of total ash of seeds of quercus leucotrichophora is 21.449 ± 2.629%w/w. This may be due to presence of high amount of iron (fe) and zinc (zn) and calcium (ca). The acid insoluble part of ash was found 0.986% w/w whereas water soluble part was18.746%w/w. The extractive values for various solvents such as methanol, n- hexane, chloroform, ethyl acetate, n-butanol and aqueous were found to be 18.746, 4.6224, 0.294, 0.4982, 0.938 and 3.9834 respectively. Swelling index was measured to be 8ml/g. The powder of seeds was found to contain carbohydrate and tannins. Conclusion: the qualitative tests, physicochemical parameters and tlc establish standards in identity and quality of seed material. Quercus leucotrichophora seeds are found to be safe with assured quality.
Doxycycline is the most second generation bacteriostatic antibiotic used to treat various infectious agents including intracellular pathogens. It is effective against gram positive pathogens like Staphylococcus aureus and gram negative pathogens like treptococcus pneumoniae.(1) It is inexpensive and multi- purpose drugs used commonly to treat bacterial infections and it also shows therapeutic benefit in treatment of cancer, Alzheimer’s disease, malaria and cardiovascular disease. Drug reposition is one of the approach to treat viral infections hence antibiotics like macrolides, glycopeptides, tetracyclines and beta-lactams have been approved by regulatory authorities to fight against viral infections.(2) Doxycycline inhibits replication of wide range of viruses including enveloped and non-enveloped viruses, but its use is restricted in children younger than 8 years of age due to its potential side effects.(3) One such example is use of doxycycline in treatment of SARS-CoV-2 and in-vitro based studies revealed that this drug is effective even at low concentrations and it works by inhibiting viral replication of IHUMI-3 and IHUMI-6 strains.(4) Doxycycline is generally well tolerated when compared to minocycline and adverse effects include esophagitis, mediastinitis. It may have the ability to induce photosensitivity reactions and anaphylactic reactions. Long term use leads to bone deformities and teeth discoloration and reduced contraceptive efficacy in women.(5) There is an intricate relation between Chikungunya and post viral arthritis that lead to our present case report focussing on doxycycline induced urticaria. CHIKV is an arbovirus spread by Aedes aegypti mosquitoes and this disease is characterized by high fever, headache, rash, myalgia and severe joint pain. Usually these symptoms resolve over 2 weeks and if not it usually requires medical attention.(6) A series of events led to development of urticaria in the patient and drug induced urticaria can occur alone or associated with other symptoms such as angioedema and anaphylaxis. It is reported that 1-3% of drug reactions are cutaneous that are precipitated through either IgE mediated pathway or circulating immune complex reactions or pseudo-allergic reactions. From a retrospective study it is found that doxycycline accounts for 0.7% of total ADRs making it rare but requires timely medical attention.(7)Regardless of the time course of urticarial symptoms usually range from pink to pale plaques with erythematous flare ups, the plagues are usually in round, oval with few millimeters to few centimeters in size. These are usually not painful and are mostly pruritic.(8) The present case report discusses adverse drug reaction due to doxycycline, its anticipated pathophysiology, differential diagnosis and the effective therapeutic management strategies employed to treat urticaria in the patient.
Case Presentation:
A female patient of age 28 years presented to OPD with chief complaints of generalized body pains more intense in upper limbs and back since 10 days. The patient was also presented with generalized body weakness since 5 days accompanied by fever(low grade). The patient has no history of CAD, CVA, HTN and T2DM. Laboratory investigations like CBP, confirmatory diagnostic tests for malaria, typhoid, dengue and viral marker analysis was also performed. Based on subjective and objective evidence the diagnosis was made as viral arthritis (suspected CHIKV) and the patient was put on symptomatic treatment consisting of pain medicine like T. Ultracet(BD) composed of tramadol(37.5mg) and acetaminophen(325mg); antibiotic like doxycycline 100mg(BD) and as patient had chief complaint of fever she was prescribed with T. Dolo composed of paracetamol 650mg (SOS) and for generalized weakness patient was prescribed with T.Zincovit composed of vitamin-A,D3,E, niacinamide, copper ,zinc and manganese.
Medical history related to present ADR:
After 5 days patient was again admitted in the hospital with chief complaints of redness and swelling of face and edema on both lower and upper limb since 3 days accompanied by severe pain. On physical examination erythema and edema was seen on both arms and legs associated with itching and bruising all over the skin especially on face. Upon patient interview she revealed that she has only taken all the prescribed medications for only one day as there were no more symptoms, and doxycycline 100mg(BD) was the only medication she was taking regularly since 5days and on the 5th day she had an intense itching associated with pain along with increased puffiness of face and angioedema on lips, genital areas and around eyes. The patient had no prior known history of drug and non-drug allergies, no familial history and was found to be non-compliant with medications.
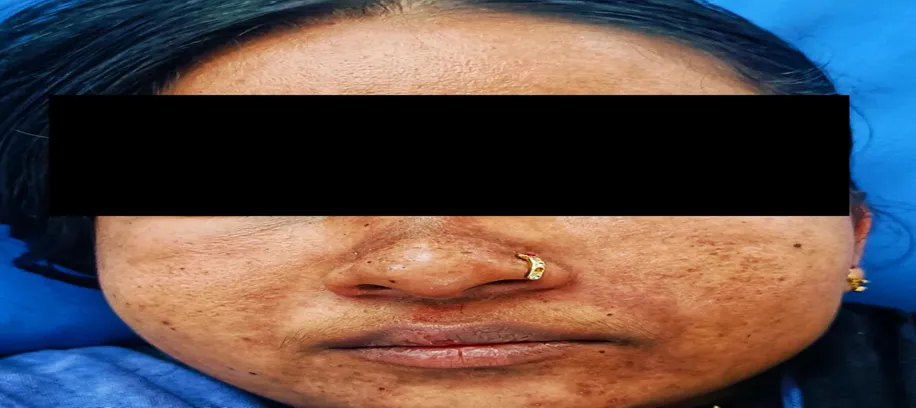
Figure 1. Erythematous wheals accompanied by angioedema, puffiness and purplish bruising
Examination:
Patient was found to be afebrile, conscious and reciprocating to doctors instructions. The vitals noted as PR-92bpm, RR- 22/min; BP-100/70mm hg; Sp02: 98%; CVS-S1, S2+; RS: BAE+ and RBS were found to be 160mg/dl. The abnormal laboratory investigations are as follows:
Table1. Abnormal Lab Investigations Seen in Patient During Hospitalization
|
Parameter |
Result values |
Biological references |
|
Complete Blood Picture |
||
|
Heamoglobin |
10.9 |
12 – 14 gm/dl |
|
T.W.B.C |
13,700 |
4,000 – 11,000/cmm |
|
Polymorphs |
88 |
50 – 70% |
|
Lymphocytes |
08 |
25 – 45% |
|
Monocytes |
02 |
3 – 8% |
|
T.R.B.C |
4.1 |
4.5 – 5.5 millions/cmm |
|
M.C.V |
82 |
86 – 98 FL |
|
M.C.H |
26 |
27 – 32 pg |
|
ESR |
30 |
0 – 15 mm/hr |
|
Platelet Count |
1,37,000 |
1.5 – 4 lak/cmm |
|
Liver Function Test |
||
|
SGOT |
210 |
10 – 38 IU/L |
|
SGPT |
190 |
7 – 55 IU/L |
|
Albumin |
2.7 gm/dl |
2.5 – 5 gm/dl |
|
Lipid Profile Test |
||
|
Triglycerides |
588 |
< 150 mg/dl |
|
VLDL |
117 |
20 – 40 mg/dl |
|
Serum Electrolytes |
||
|
Chlorides (Cl) |
108 |
96 – 106 mmol/l |
After the patient was stabilized in the ER she was shifted to General medicine department and appropriate treatment was given. On second day of hospitalization patient was advised for thyroid profile and results were within normal range. The reticulocyte count is increased(1.9%) indicating chances of hemolytic anaemia that need to be ruled out once the patient is recovered from the ADR. The 24 hours urine proteins were found to be exceeding the normal range (297mg/day). The Ultrasound scan of abdomen had shown increased echogenicity of liver along with hepatomegaly giving the impression of Grade-II fatty liver.
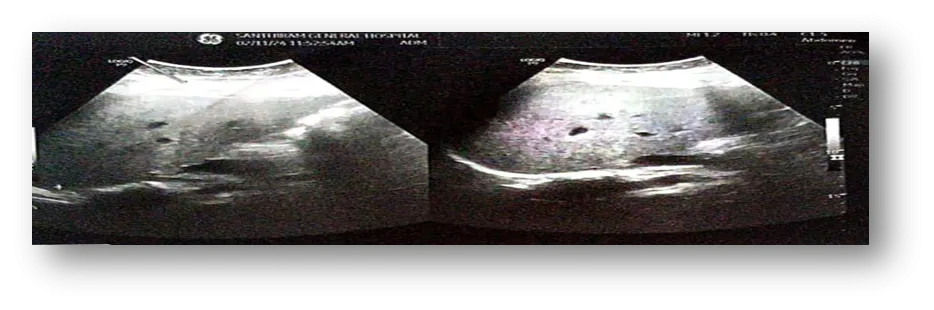
Figure2. USG scan of abdomen showing Grade-II fatty liver
Management of ADR:
Upon evaluation of lab data, presenting symptoms and existing medical history the patient is reported with drug induced urticaria secondary to doxycycline classified under drug induced hepatitis post viral arthritis. Tabet Doxycycline was completely withdrawn and the dechallenge was found to be positive where the patient had shown slight improvement I the symptoms and no rechallenge was performed as it was a serious ADR. The patient was put on symptomatic treatment and was monitored constantly. Patient was put on systemic corticisteroid therapy with inj.Dexamethasone 8mg(BD) to treat urticaria and inj.lasix composed of furosemide(20mg) a loop diuretic was adminstered twice in a day intravenously. To treat the reaction patient was prescribed with tab.Montek LC composed of montelukast(10mg) and levocetirizine(5mg) at night and tab.bilastine(20mg) in the morning.This case was referred to dermatology department and patient was prescribed with Triben B cream composed of cotrimoxazole(1%W/W) and beclomethasone(0.025%W/W) suggested for topical application twice in a day especially at the itchy affected areas of the body. Patient was prescribes with tab.Udiliv composed of ursodeoxycholic acid(300mg) OD that acts as a hepatoprotective preventing further damage to liver.
DISCUSSION:
Drug induced urticaria is a skin reaction caused mainly due to NSAID’S and antibiotics characterised by swelling on skin and deeper in the skin termed as angioedema. In outpatient depatments it affects 9% of patients more prevalent in adults and children. This case report is validated based on the probability assessment of ADR by Naranjo’s Scale.
Table 2. Naranjo Scale: Probability assessment of Doxycycline induced urticaria.
|
Question |
Yes |
No |
Do Not Know or Not Done |
Score In Our Case |
|
Are there previous conclusive reports on this reaction? |
+1 |
0 |
0 |
+1 |
|
Did the adverse event appear after the suspected drug was given? |
+2 |
-1 |
0 |
+1 |
|
Did the adverse reaction improve when the drug was discontinued, or a specific antagonist was given? |
+1 |
0 |
0 |
+1 |
|
Did the adverse reaction appear when the drug was re administered? |
+2 |
-1 |
0 |
0 |
|
Are there alternative causes that could have caused the reaction? |
-1 |
+2 |
0 |
+2 |
|
Did the reactions reappear when a placebo was given? |
-1 |
+1 |
0 |
0 |
|
Was the drug detected in any body fluid in toxic concentrations? |
+1 |
0 |
0 |
0 |
|
Was the reaction more severe when the dose was increased or less severe when the dose was decreased? |
+1 |
0 |
0 |
0 |
|
Did the patient have a similar reaction to the same or similar drugs in any previous exposure? |
+1 |
0 |
0 |
0 |
|
Was the adverse event confirmed by objective evidence? |
+1 |
0 |
0 |
+1 |
|
Total score |
|
6 |
||
Probability depicts the likelihood that a suspected drug is responsible for the occurrence of an ADR. For Doxycycline induced urticaria the score obtained was 6 falling into category of Probable type of ADR.(9) The management of ADR was achieved by symptomatic approach of therapeutics where combination of short systemic corticosteroid therapy along with antihistamine drugs was found to likely improve urticarial activity and provide relief from itching and wheals in patient.(10) Standard treatment is generally not available for drug induced liver injury and management is usually based on withdrawal of suspected drug but some studies show that Ursodeoxycholic acid shows promising benefits to prevent further damage to liver hence empirical use in DILI appears to be safe clinical practice. The expected outcomes pertaining to patient recovery were aligned with actual outcomes and the patient had shown good prognosis over the time and the intensity of the reaction has shown a decline on a daily basis. The serum electrolyte levels and CBP reports were normal and here was a slight decline in abnormal liver enzyme levels along with patient showing improved symptoms such as reduction in facial puffiness, reduction in angioedema around mouth, eyes and feet and lupus like flare ups on the skin especially around the nose region. Furthermore as the patient recovered from the ADR and there was no prolonged hospitalization, serious complications or irretrievable issues as a result of reported ADR the patient was discharged from the hospital after providing proper education on medication compliance and its potential benefits.
CONCLUSION:
Doxycycline induced urticarial is a rare but serious adverse event when not given timely medical attention. Diligent monitoring of ADR is essential to understand the safety of the drugs. Urticaria usually has multiple causes hence differential diagnosis and through proper assessment is crucial to prevent serious adverse events. We are reporting the current case as many drug induced urticaria cases go unreported and hence we aim to create clinical awareness among healthcare professionals. It is essential to carry future research in understanding the mechanism behind drug induced urticaria that will provide evidence based clinical practice along with enhancement of Spontaneous reporting of such ADR’s in the future.
Abbreviations:
CHIKV-Chikungunya Virus, IgE-Immunoglobulin-E, ADRs-Adverse Drug Reactions, OPD-Outpatient department, CAD-Coronary artery disease, CVA-Cerebrovascular accident, HTN-Hypertension, T2DM-Type2 diabetes mellitus, NSAIDs- Non steroidal anti-inflammatory drugs, DILI-Drug Induced Liver Injury.
ACKNOWLEDGEMENT:
Nil
Conflict of interest:
The authors declare no conflict of interest.
Funding support:
The authors declare that no funding was received for this case report.
Declaration of patient consent:
The authors ensured that they have obtained appropriate patient consent forms. The patient is ensured that their names and initials will not be published and efforts will be made to conceal their identity and any information revealing their identity shall not be disclosed.
REFRENCES



Karan A. S.*, M. Senthilkumar, Loganantham, Mukesh V., Celcia S., Mohanapandiyan S., Fathimathul Nusaira T., Harshad M. K., Knowledge, Attitudes, and Practices (KAP) of Antibiotic Use and Resistance Among Pregnancy Women in Coimbatore, Int. J. Med. Pharm. Sci., 2026, 2 (3), 68-77. https://doi.org/10.5281/zenodo.18964906
 10.5281/zenodo.11109715
10.5281/zenodo.11109715