
We use cookies to ensure our website works properly and to personalise your experience. Cookies policy
1School of Pharmacy and Life Sciences, Centurion University of Technology and Management, Odisha, India,752050, 0009-0008-5012-6644.
2Arya college of pharmacy, SP-40, RIICO Industrial Area, Delhi Road, Kukas, Jaipur, Rajasthan 302001, .
3Gitanjali college of Pharmacy, Maulana Abul Kalam Azad University of Technology, West Bengal, India, 731237, 0009-0004-6586-7024.
A person having diabetes, also referred to as diabetes mellitus (DM), has elevated levels of glucose in their blood because of either insufficient insulin production by the pancreas or an inefficient cell response to insulin. The overall aim of this research is to conduct a comparative evaluation of Imeglimin, Glimepiride, and Linagliptin anti-diabetic drugs in the management of Type-II diabetes induced by a high-fat diet (HFD) combined with low-dose streptozotocin (STZ) on Albino Wistar rats. 30 rats are divided into 5 groups. Start treatment with the Anti-diabetic drugs in the respective treatment group after confirmation of diabetes. The doses of Imeglimin, linagliptin, and glimepiride are 150 mg/kg/day, 5mg/kg/day, and 1mg/kg/day, respectively, administered orally to the respective groups. the challenged group receives no therapy, while the control group receives vehicle treatment. The biggest improvement in blood glucose control was seen by Imeglimin, which significantly lowered both fasting and postprandial glucose levels. Furthermore, it did not allow gaining of weight which is associated with diabetes and also refined lipid profiles. On the other hand, Linagliptin though enhanced renal protection, it showed not much impact on lowering of cholesterol and glucose levels. Glimepiride was the least effective in lowering cholesterol levels and causing weight changes. This study shows that, in comparison to Imeglimin and glimepiride, linagliptin is excellent in kidney protection, while Imeglimin is most effective for controlling glucose levels and lipid profile. All three drugs have therapeutic potential for the management of Type 2 diabetes and its complications.
Diabetes, often known as diabetes mellitus (DM) or just diabetes, is a type of metabolic condition in which a person has excessive blood glucose levels due to either insufficient insulin synthesis by the pancreatic beta cells or insulin resistance. Polydipsia, Polyphagia, Polyuria, impaired vision, and weight loss are typical symptoms of diabetes mellitus [1]. Ketoacidosis or a non-ketotic hyperosmolar condition may manifest in severe forms, resulting in stupor, coma, and, without appropriate intervention, death.Type 2 Diabetes Mellitus (T2DM) constitutes the bulk of diabetes mellitus cases (90-95%), occurring more frequently than Type 1 diabetes [2].Type 2 diabetes mellitus (T2DM) is a complex, multifaceted condition marked by hyperglycemia and a progressive deterioration in insulin efficacy (insulin resistance), succeeded by the incapacity of beta (β)-cells to compensate for insulin resistance (pancreatic β-cell dysfunction). Diabetes mellitus is one of the most common chronic diseases in both developed and developing countries, accounting for a significant portion of morbidity and mortality [3]. According to a recent assessment, there are currently an estimated 382 million individuals with diabetes, and by the year 2035, there will be 592 million people with the disorder. Hyperglycemia and diabetes are caused by insufficient insulin production (absolute or relative to the body's requirements), defective insulin production (rare), or cells' inability to use insulin properly. Insulin resistance results from the latter condition, which mostly affects fat and muscle cells. This is the main difficulty with type 2 diabetes [3,4]. The primary issue in type 1 diabetes is a complete lack of insulin, which is usually caused by a mechanism that damages the pancreatic beta cells that make insulin. In addition to the slow loss of beta cells, type 2 diabetes produces elevated blood sugar levels. In essence, if a person suffers from insulin resistance, the body can, to some extent, increase insulin production while decreasing resistance [5,6]. Hyperglycemia develops over time when Insulin is not produced as well as not released properly in time. Insulin is very much essential for monitoring glucose uptake into the cells by GLUT-1 and GLUT-2 transporters and for the purpose of maintaining glucose level too. Genetic predispositions, sedentary lifestyles, poor dietary habits, obesity, and other environmental factors are all part of the complex pathophysiology of Type 2 Diabetes. Muscles, liver and adipose tissues often exhibit insulin resistance, a feature of Type 2 Diabetes that leads to decreased glucose absorption and increased hepatic glucose production [7]. Persistent hyperglycemia and related issues arise when pancreatic β cells are unable to adjust to resistance over time. Adequate preclinical models are required for effective therapeutic approaches that would accurately replicate the pathophysiology of human T2DM [8,9,10]. One such model includes administration of rodents with a high-fat diet (HFD) alongwith a low dosage of streptozotocin (STZ). The dual induction approach is important because it explains partial β cell dysfunction due to STZ and insulin resistance produced by excess eating. In these models, Rats given a high fat diet for many weeks develop insulin resistance, and simultaneous injection of STZ (typically 30-35 mg/kg, i.p.) along with nicotinamide causes mild β-cell cytotoxicity, which results in a diabolic phenotype resembling Type 2 Diabetes in humans[11]. Blood glucose levels, lipid profiles, renal biomarkers, weight changes, and pancreatic histology are some of the metabolic and histological aspects of diabetes that can be studied using these experimental method. Prior to clinical trials , these models are essential for assessing the potency, safety and effectiveness of antidiabetic drugs [12,13].Anti-diabetic drugs currently available fall into several pharmacological types, including insulin secretagogues, insulin sensitizers, dipeptidyl peptidase-4 (DPP-4) inhibitors, and new mitochondrial modulators. The current study examines three marketed medications with different modes of action [14].Imeglimin is a novel oral antidiabetic drug from the Tetrahydro triazine (glimin) class that works by improving mitochondrial function its oxidative phosphorylation blocker, decreasing hepatic gluconeogenesis, increasing insulin secretion, and increasing muscle glucose absorption. It addresses a wide range of T2DM pathophysiological abnormalities [15].Glimepiride, a second-generation sulfonylurea, stimulates insulin release by binding to ATP-sensitive potassium channels in pancreatic β-cells. Although effective, its use may increase the risk of hypoglycemia and weight gain.Linagliptin is a DPP-4 inhibitor that prolongs the effect of incretin hormones (GLP-1 and GIP), increasing glucose-dependent insulin production while reducing glucagon release [16]. Linagliptin is particularly notable for its renal safety profile, as it is primarily eliminated through the bile.Imeglimin, glimepiride, and linagliptin therapeutic efficacy in an HFD/STZ-induced type 2 diabetes model in Albino Wistar rats is the main goal of this study. among the particular goals are: Evaluating variations in postprandial and fasting as well as HbA1c blood glucose levels. Assessing lipid profiles, such as HDL, LDL, VLDL, triglycerides, and total cholesterol. evaluating nephroprotective effects by measuring renal biomarkers such creatinine, uric acid, and blood urea [17,18,19]. to ascertain tissue-level alterations and medication-mediated protective effects, histological examination of pancreatic and renal tissues is carried out. Contrasting the three medication regimens' overall effectiveness, safety, and metabolic results [20].Although there are many anti-diabetic drugs available, issues like patient heterogeneity, drug induced side-effects, and the development of comorbidities often hamper the treatment plan. Three different anti-diabetic medications are systematically evaluated in this study, with an emphasis on their metabolic effects, potential for organ protection , and applicability in a model that reflects the pathophysiological complexity of human T2DM. Furthermore, finding pharmaceuticals that provide both organ protection and glycemic management is crucial given the rising prevalence of diabetes-related kidney and cardiac problems[21]. Glimepiride’s strong insulinotropic impact , Linagliptin’s renal safety, and Imeglimin’s unique method of action make them excellent choices for comaparative investigation[22].By utilizing a robust and clinically relevant animal model, this research aspires to contribute to a deeper understanding of anti-diabetic drug efficacy and inform future directions in diabetes pharmacotherapy and as well as combination therapy [23,24].
MATERIALS AND METHODS:
Materials required: All chemicals used for the experimental purpose were of analytical grade. Imeglimin HCl (moll wt. 191.66), Glimepiride (moll wt.490.62), Linagliptin (moll wt.472.54),Streptozotocin (moll wt.265.22), EDTA sodium, RectifiedSpirit denatured (99.99%), Extra pure methanol ware purchased from Sigma Aldrich (St, Louis, MO, USA).Butterfly needle (22x3/4, 0.70x19mm)for blood sample collection was purchased from BD medical,Eppendorf Tube (5ml) from Lab India Pvt Ltd.
Animals Required: Our Institutional animal house is CPCSEA (Regulatory Body of the Government) approved having registration number (1726/PO/Re/S/14/CPCSEA)For our study we have taken30 Albino Wistar rats of either sex (150–220 g) were obtained from the animal house and kept at room temperature at (22-28 ºC)with 45-65% relative humidity,12 hrs. dark and light cycles and given standard laboratory feed and water ad-libitum.after that rats are divided into 5 groups, the normal control group is fed a regular diet that includes protein, carbohydrates, fats, minerals, and fiber (soybean, wheat, oats, etc.); the challenged group is given a high-fat diet and a low dose of STZ. The remaining three test groups are fed HFD+STZ and the appropriate medication for each group [25,26].
Induction of Type 2 Diabetes Mellitus (T2DM):Feed rats a high-fat diet (40-60% fat) for 12-15
weeks to induce insulin resistance. Control group normal diet.after HFD feeding, rats receive an
intraperitoneal (i.p.) injection of low-dose STZ (30-35 mg/kg) dissolved in citrate buffer (pH 4.5),
to induce partial beta-cell destruction, nicotinamide (100-110) mg/kg administer 15 min prior STZ
administered [27,28]. confirmation of diabetes: measure fasting blood glucose (FBG) levels after
48-72 hours post-STZ injection using glucometer (Accu-check), rats with FBG > 160-250 mg/dL, with other symptoms of diabetes mellitus such as polyphagia, polydipsia, polyuria are considered as diabetic [29,30].
|
Particulars |
Details of Protocol/steps to be followed |
|
|
Animal Model |
Albino Wistar Rats (male/female), 150–200 g |
|
|
Group Division |
Control Group: Normal Pellet Diet (NPD) |
|
|
HFD Composition (per 1 kg) |
Fructose (60%): 175 g |
|
|
HFD Feeding Duration |
12–15 weeks |
|
|
STZ Dose |
Streptozotocin (STZ) 30–35 mg/kg, i.p., dissolved in citrate buffer (0.1 M, pH 4.5) |
|
|
Nicotinamide Dose |
|
|
|
Post-STZ Evaluation |
Measure Fasting Blood Glucose (FBG) after 48–72 hours |
|
|
Diabetes Confirmation |
FBG > 160–250 mg/dL, with clinical signs: polyphagia, polydipsia, polyuria |
|
|
Glucose Monitoring Tool |
Glucometer (Accu-Chek or equivalent) |
Table 1: Details of daily feeds, challenging agent induction, and intense monitoring schedule
Drug Administration: Animals are distributed into 5 groups, group 1 is control, group 2 is challenged, and group 3 is Imeglimin treated group, group 4 is Linagliptin treated, and group 5 is Glimepiride treated [30,31]. initiate treatment with the anti-diabetic drug to respective group after diabetes confirmation. give the drug, route: oral (gavage) frequency: once daily. duration: 4 weeks. the Imeglimin dose is 150 mg/kg/day oral administration to group 3, the Linagliptin dose is 5mg/kg/day oral administration to group 4, and the glimepiride dose is 1mg/kg/day oral administration to group 5. the challenged group is not treated, whereas the control group is treated with the vehicle [32,33,34].
Biochemical Assessments: Blood sample from the experimental rats were taken from Retro-orbital plexus in the anticoagulants bottles and were centrifuged within 2 hours. Separated plasma of blood samples which were collected and stored in a freezer at -20°C for fasting blood glucose (FBG) and post prandial (PP) weekly analysis [35,36]. Perform an HbA1c test post-treatment. take body weight and Food Intake, Lipid Profile: Measure serum cholesterol, triglycerides, HDL, LDL and VLDL levels. Kidney function test: Measure Urea, uric acid, creatinine levels, using autoanalyzer for this test and using Robonik Test Kit [37,38,39].
Histopathological Analysis: To look for any structural alterations, the pancreatic and renal tissues were taken from the experimental rat after it had been put to sleep with a CO2 chamber.
Statistical analysis: One-way ANOVA and the Dunnet test were used to do statistical analysis, and the findings were displayed as the average plus or minus the standard deviation.
The information was prepared for statistical analysis.
Results and Discussion: After inducing a high-fat diet, the blood glucose level of rats increased significantly from days 15 to 90. After inducing STZ, the fasting blood glucose level was higher than 250 mg/dL.The fasting and postprandial (PP) blood glucose levels of three treatment group rats were highly significantly decreased, ** P<0.01 compared to the (HFD + STZ) challenged group at day 14th and from day 28th. Three treatment group rats' fasting and postprandial (PP) blood glucose levels were highly significantly decreased, ** P< 0.01, compared to the (HFD + STZ) challenged group and Imeglimin treated group, seen as highly significantly decreased ***P<0.001 compared to the (HFD + STZ) challenged group. HbA1c report Glimepiride and Linagliptin treated group rats were highly significantly decreased, ** P<0.01, compared to the (HFD + STZ) challenged group at day 28th and Imeglimin treated group seen ***P<0.001 compared to the (HFD + STZ) challenged group. In terms of blood glucose control, the ranking was: Imeglimin > Glimepiride > Linagliptin.TC, TG, LDL, and VLDL levels of Glimepiride and Linagliptin-treated group rats were highly significantly decreased ** P<0.01, and HDL levels were highly significantly increased ** P<0.01, compared to the (HFD + STZ) challenged group. and the Imeglimin-treated group seen TC, TG, LDL, and VLDL levels were highly significantly decreased ***P<0.001, and HDL levels were highly significantly increased ** P<0.001, compared to the (HFD + STZ) challenged group. The ranking for lipid levels was: Imeglimin > Linagliptin > Glimepiride.like the Matrix structure restored as compared to challenged, Bowman’s capsule, PCT, DCT, and other parts were restored moderately. The Pancreatic Duct is restored normally. Cells of the islets are visible with just slight changes to the cell density. Small signs of cells developing disorganized or shrinking.
Study for blood glucose level estimation:In this below graph and table, we can see that the blood glucose level of three treatment group rats was significantly increased.The blood glucose level increases in a standard pattern till the 90th day due to effect of high fat diet, but after STZ administration it spike up more than as usual way.
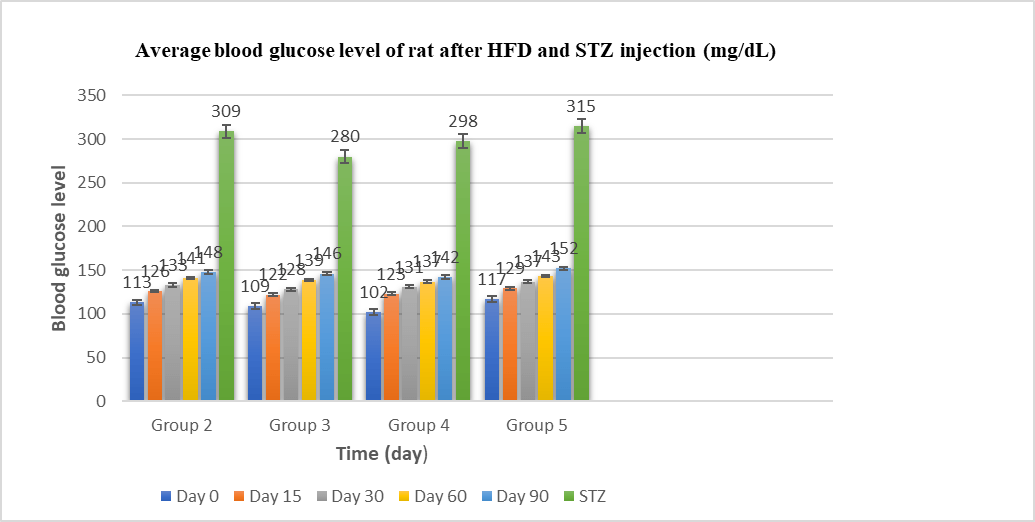
Fig. 1: Avg. blood glucose level of Albino Wistar rats (mg/dL) after HFD and STZ induce.
Study for body weight gain estimation: In this below graph and table, we can see that the body weights of three treatment group rats were significantlydecreased as compared to the (HFD + STZ) challenged group at day 14th and from day 28th day three treatment group rats body weights were highly significantly decreased.
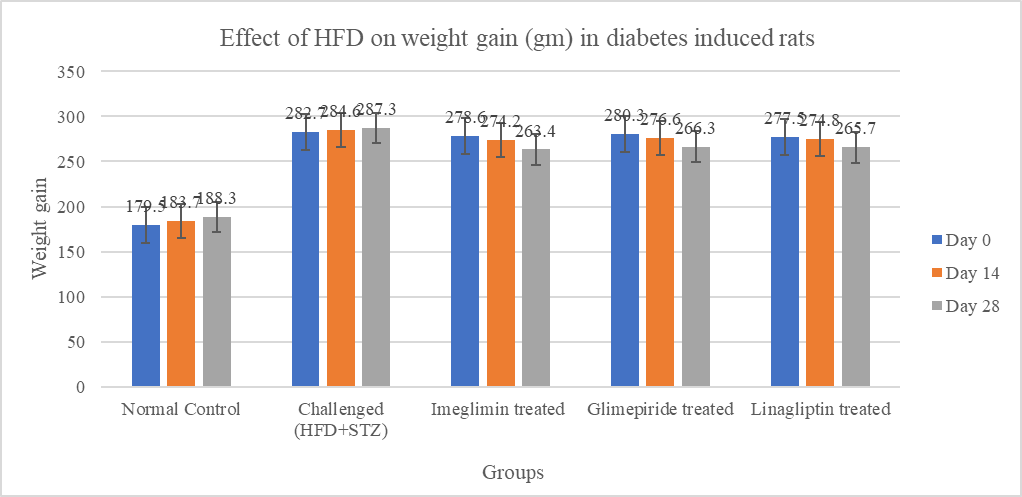
Fig. 2: Effect of HFD on weight gain in diabetes induced rats.
Study for drug treatment & blood glucose level estimation: In this below graph and table,we can see that the fasting and postprandial(PP) blood glucose levels of three treatment group rats were highly significantly decreased as compared to the (HFD + STZ) challenged group at day 14th and from day 28th day three treatment group rats'fasting and postprandial(PP) blood glucose levelwere highly significantly decreasedas compared to the (HFD + STZ) challenged group and Imeglimin treated group seen highly significantlydecreased as compared to the (HFD + STZ) challenged group.

Fig. 3: Effect of anti-diabetic drug on blood glucose level of diabetic rats
Study for drug treatment on HbA1c level estimation: In this graph and table, we can see that the blood glucose levelsHbA1c report Glimepiride and Linagliptin treated group rats were highly significantlydecreased,
Table 8: Effect of anti-diabetic drug on blood glucose HbA1c test (mmol/L) of diabetic rats.
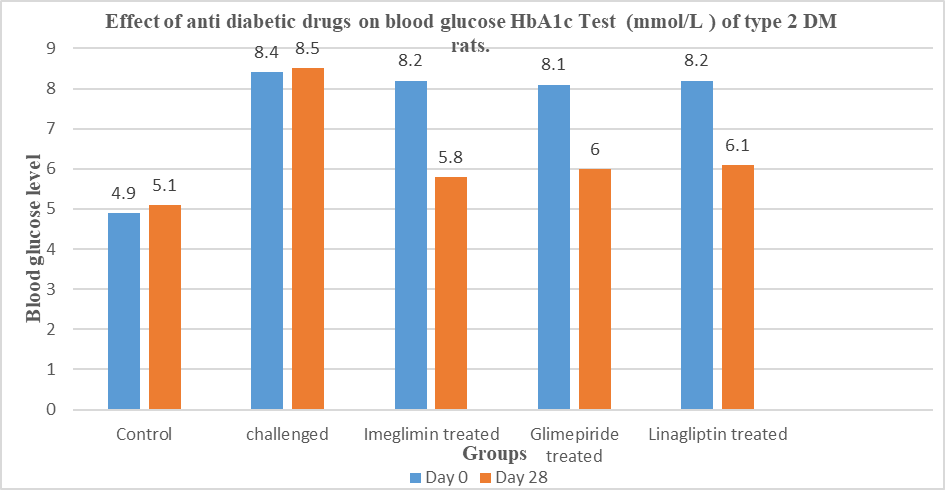
Fig. 4: Effect of anti-diabetic drug on blood glucose HbA1c test (mmol/L) of diabetic rats.
Study for drug treatment on lipid profile estimation:In this graph and table, we can see that the TC, TG, LDL and VLDL levels of Glimepiride and Linagliptin-treated group rats were highly significantlydecreased, and HDL levelsare highly significantly increased, compared to the (HFD + STZ) challenged group. and Imeglimin-treated group seen TC, TG, LDL and VLDL levels werehighly significantlydecreased, and HDL level were highly significantly increased, compared to the (HFD + STZ) challenged group.
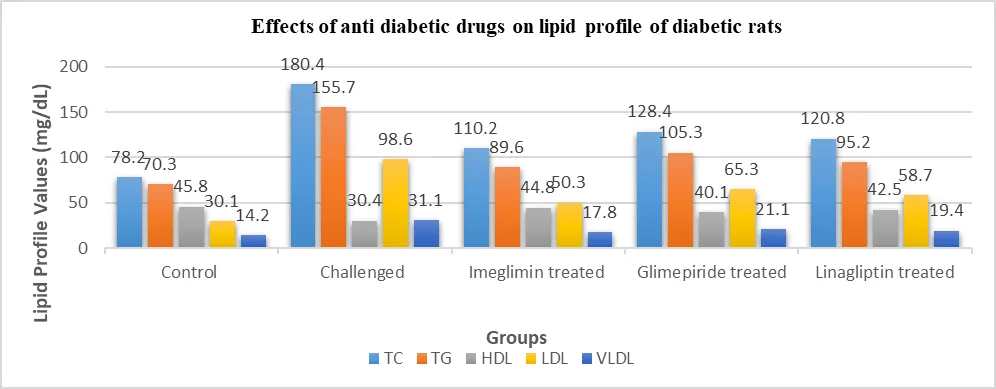
Fig. 5: Effects of anti-diabetic drugs on Lipid profile (mg/dL) TC, TG, HDL, LDL, VLDL level of diabetic rats.
Study for drug treatment on kidney biomarkers estimation:In this graph and table, we can see that the urea, uric acid and Creatinine levels of Glimepiride and Imeglimin -treated group rats were highly significantlydecreased, compared to the (HFD + STZ) challenged group. and the Linagliptin-treated group seen urea, uric acid and Creatinine levels werehighly significantlydecreased, compared to the (HFD + STZ) challenged group.
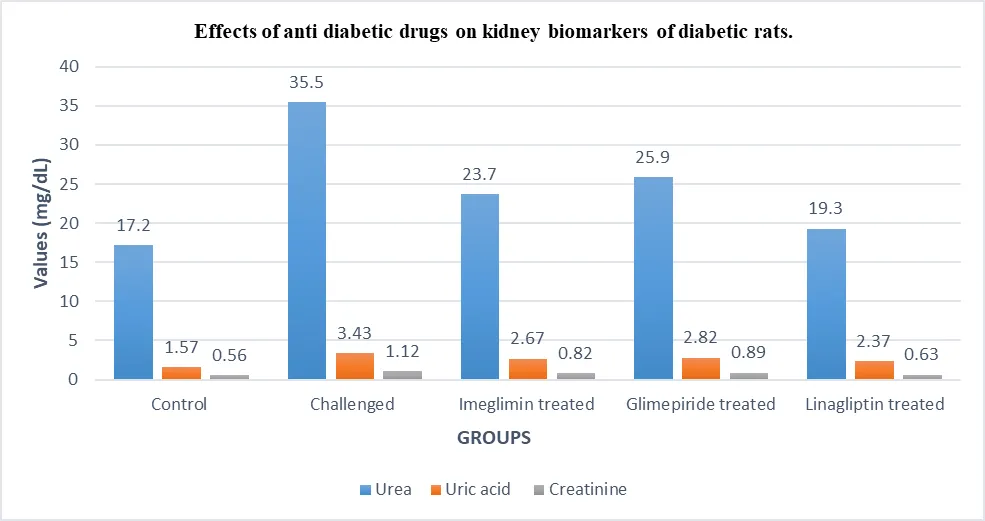
Fig. 6: Effects of anti-diabetic drugs on kidney biomarkers (mg/dL) of diabetic rats.
Histopathological Analysis: A histopathological evaluation was performed following the successful completion of the blood tests. The animal was humanely put to sleep in a carbon dioxide room prior to the tissues being collected. After that, the pancreatic and kidney sections were taken out and put in a 10% formalin solution. Following dehydration with varying ethanol concentrations, the tissue samples were cleaned with xylene, embedded in paraffin wax, and sliced thinly into 4–5 micrometre pieces. Haematoxylin and Eosin (H&E) was used to stain these slices so they could be examined under a microscope.
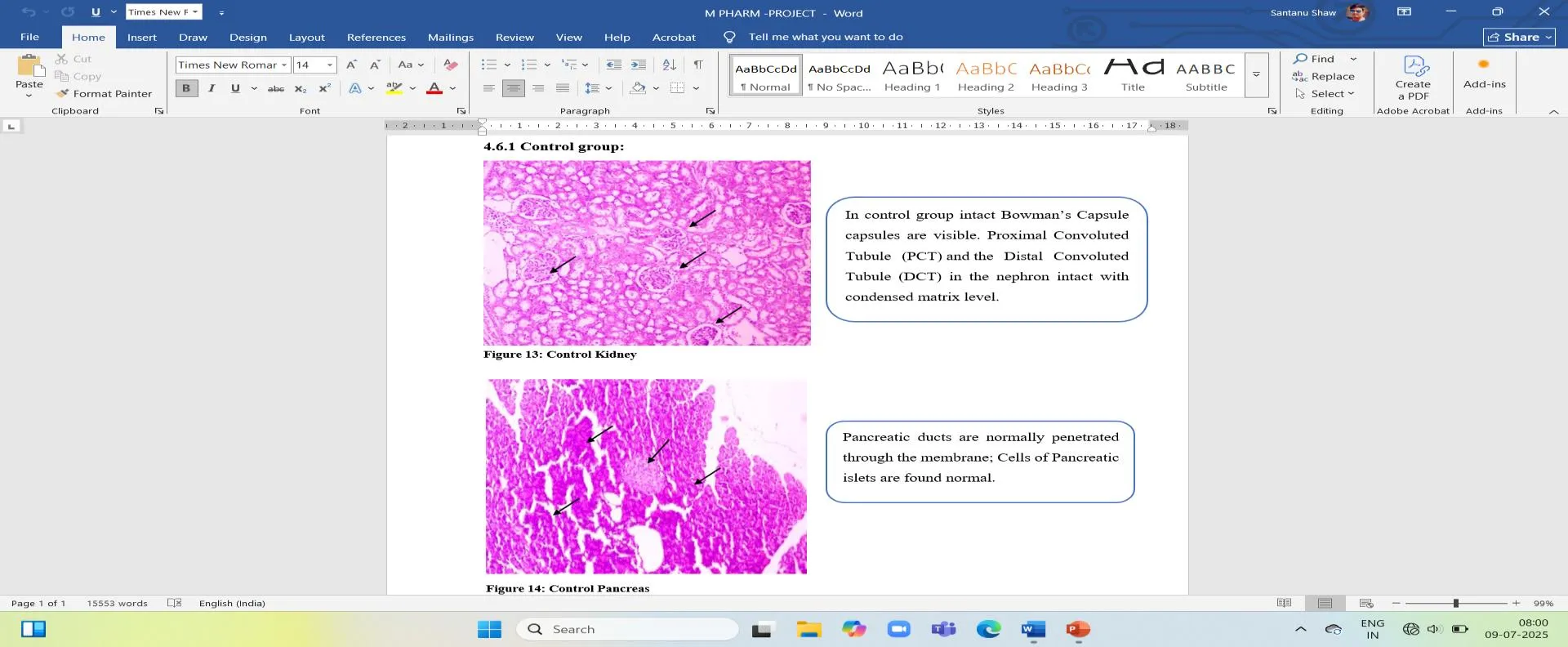
Fig.7: Control group kidney, in control group intact Bowman’s Capsule capsules are visible. Proximal Convoluted Tubule (PCT) and the Distal Convoluted Tubule (DCT) in the nephron intact with condensed
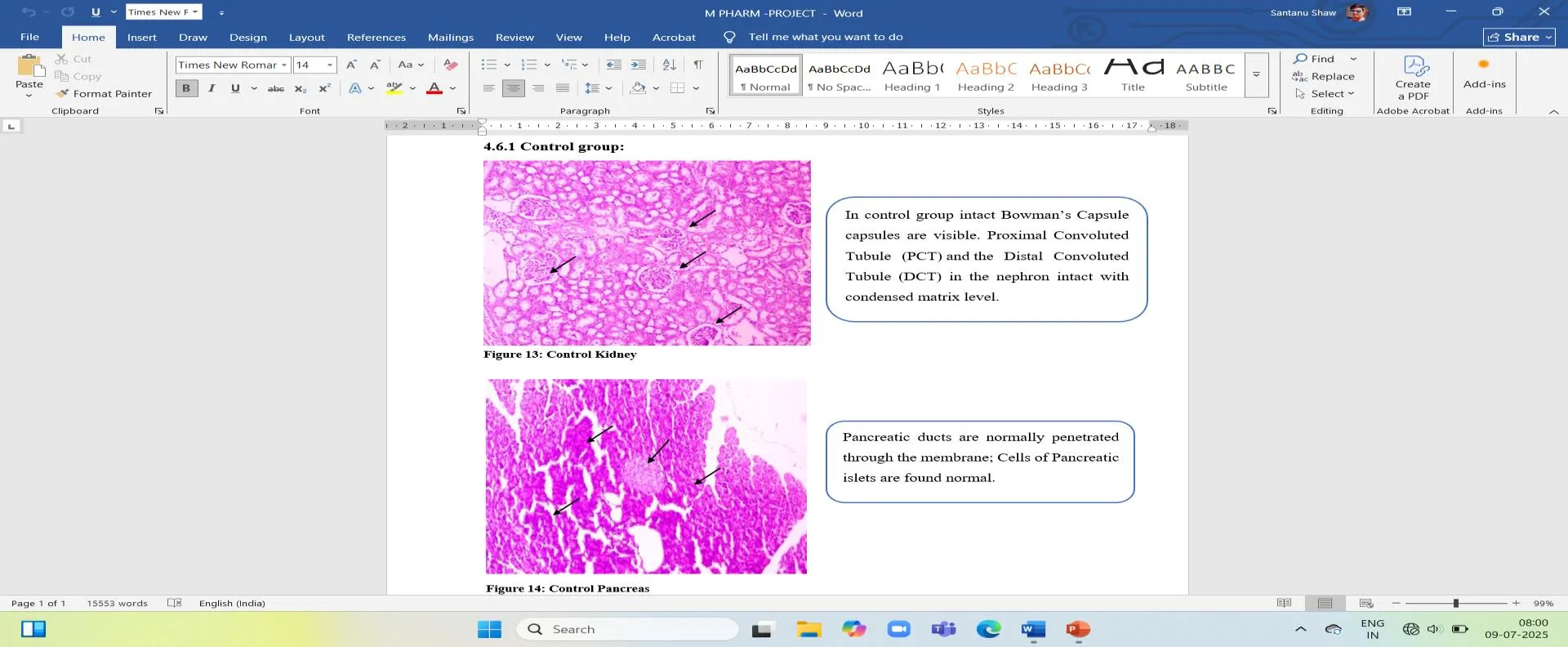
Fig 8: Control group pancreas, Pancreatic ducts are normally penetrated through the membrane; Cells of Pancreatic islets are found normal.
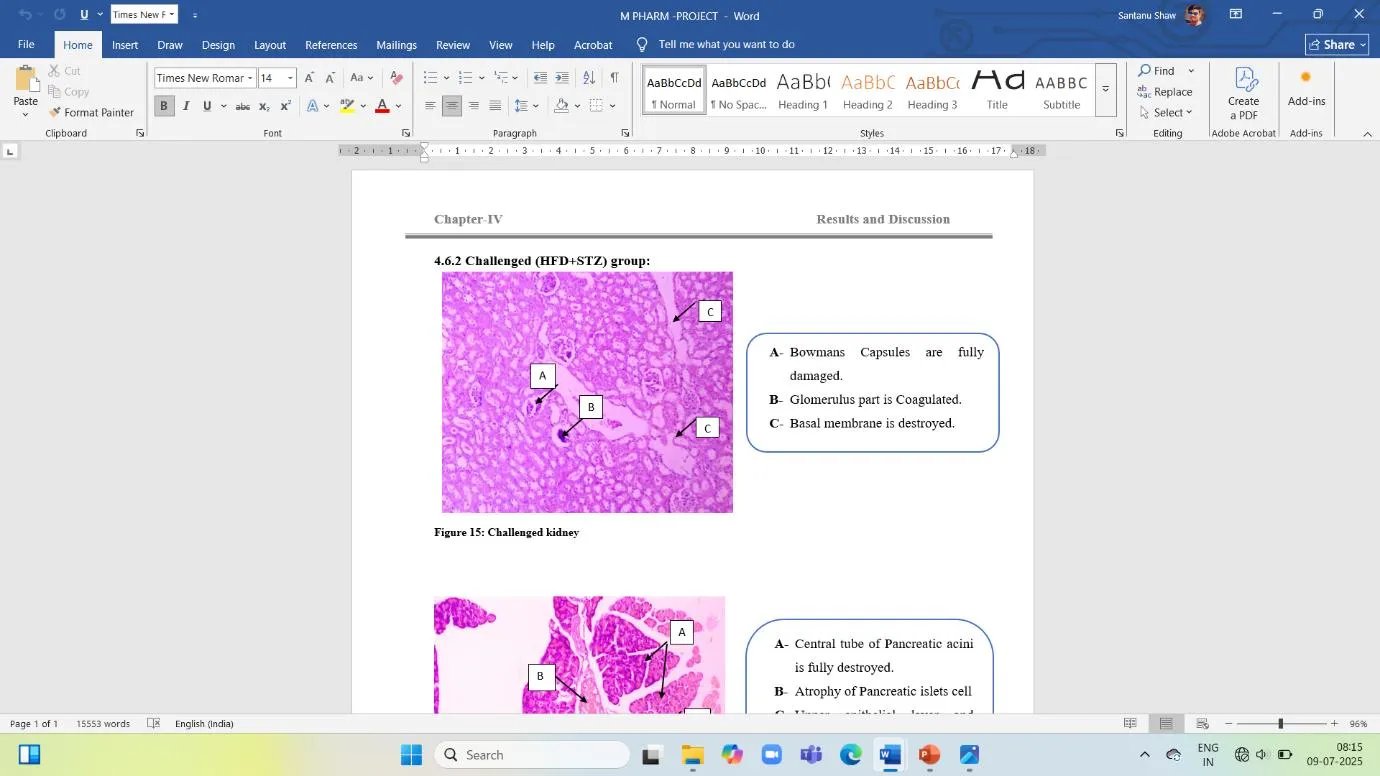
Fig. 9: Challenged group kidney,
A- Bowmans Capsules are fully damaged.
B- The Glomerulus part is Coagulated.
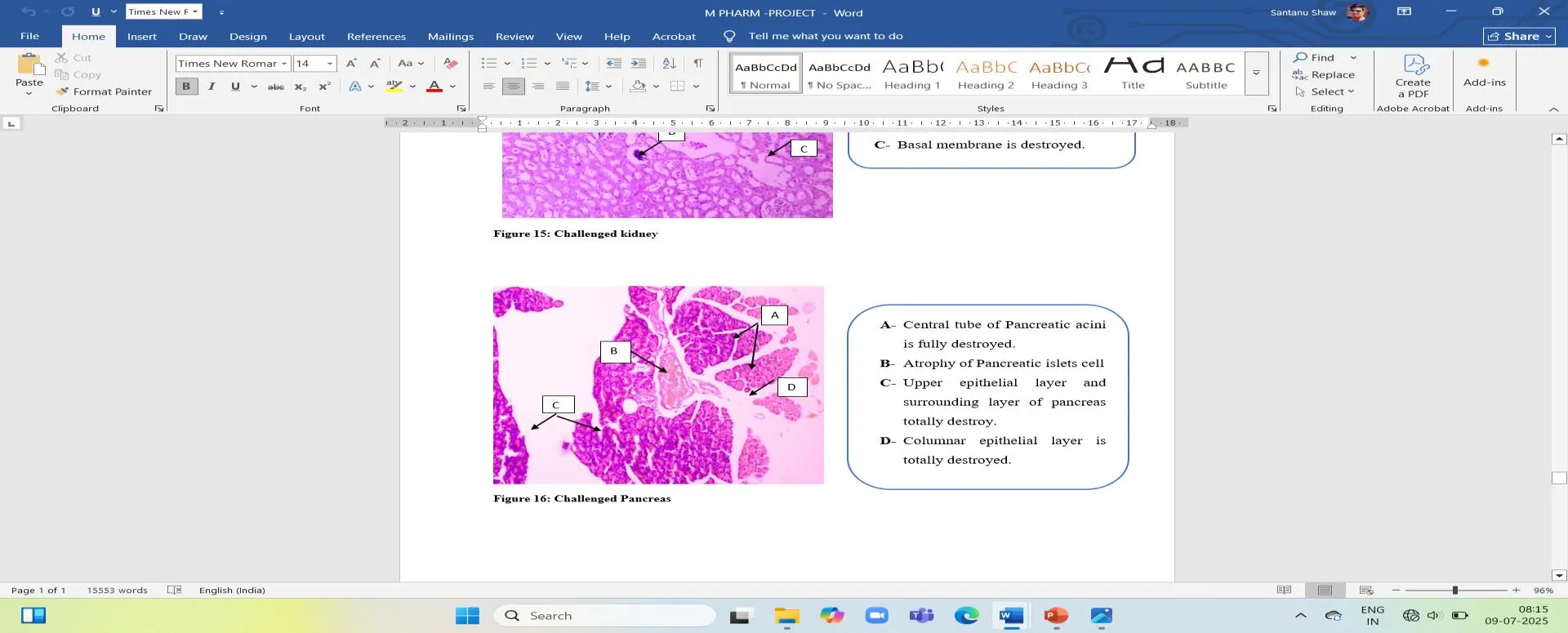
Fig. 10: Challenged group pancreas,
A- Central tube of Pancreatic acini is fully destroyed.
B- Atrophy of Pancreatic islets cells.
C- Upper epithelial layer and surrounding layer of pancreas totally destroy.
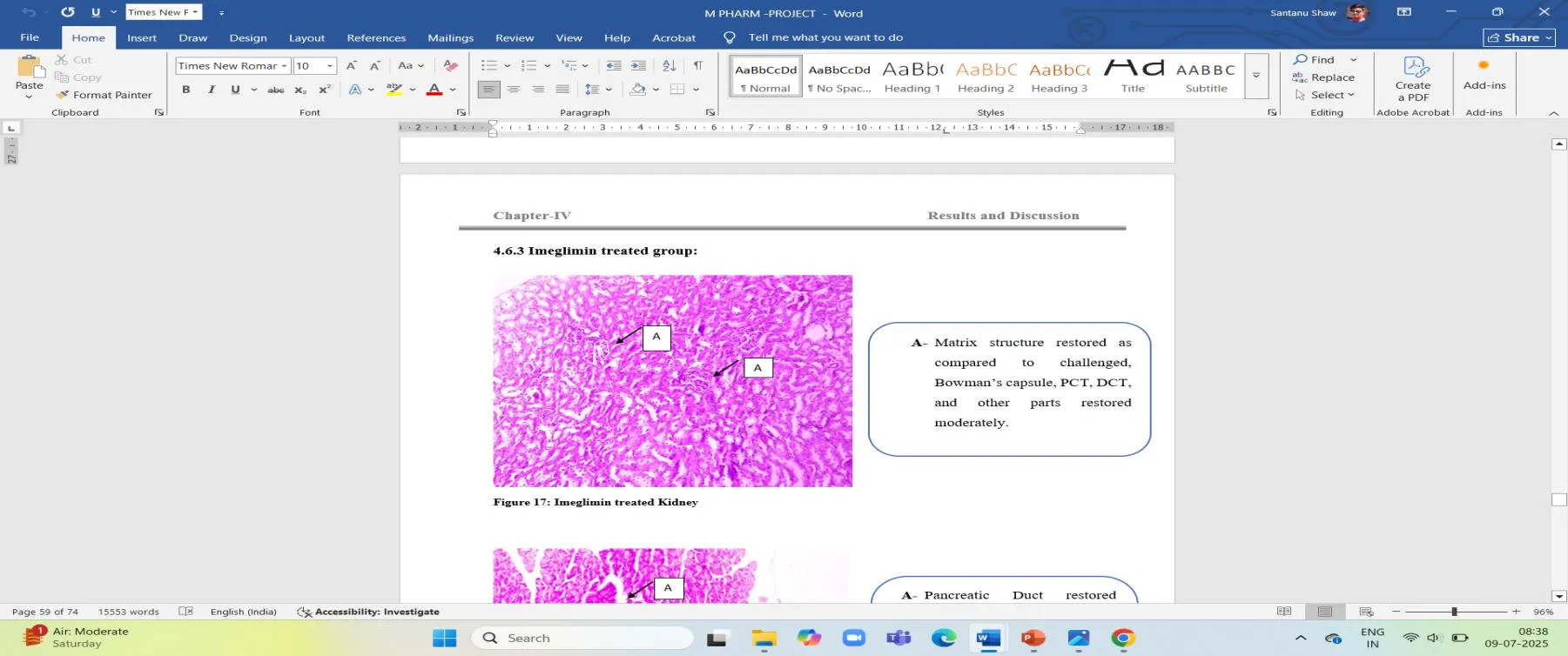
Fig. 11: Imeglimin treated group kidney,
- Matrix structure restored as compared to challenged, Bowman’s capsule, PCT, DCT, and other parts restored moderately.
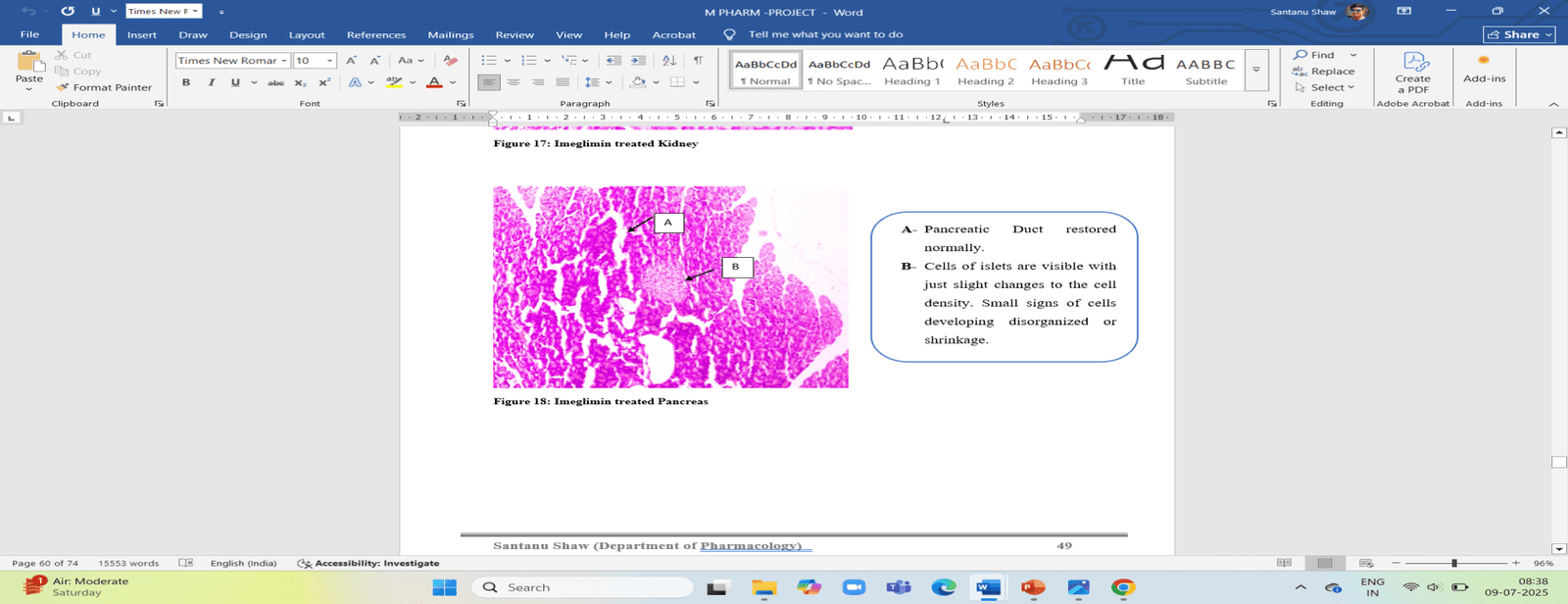
Fig. 12: Imeglimin treated group pancreas,
- Pancreatic Duct restored normally.
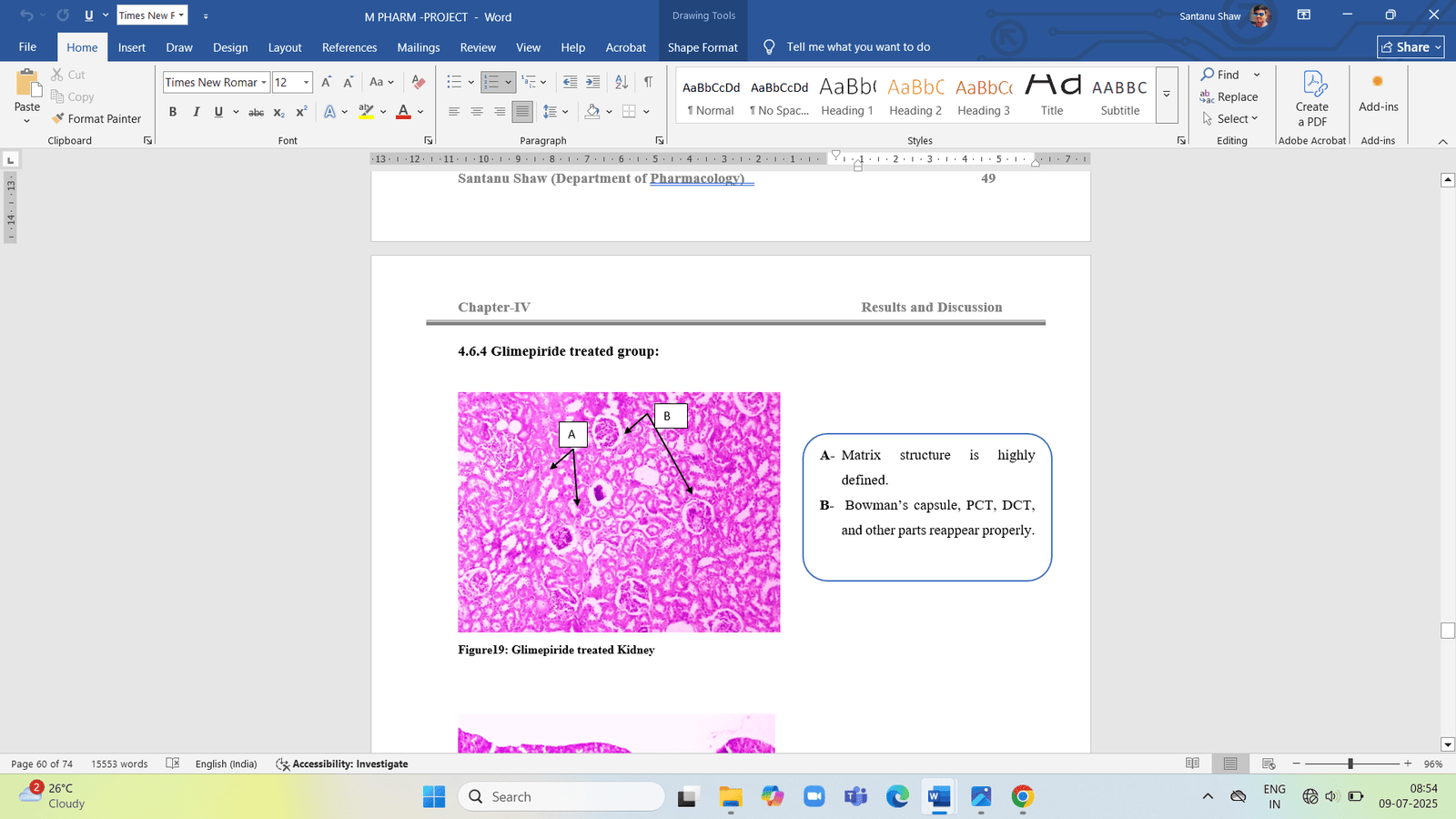
Fig. 13: Glimepiride treated group Kidney,
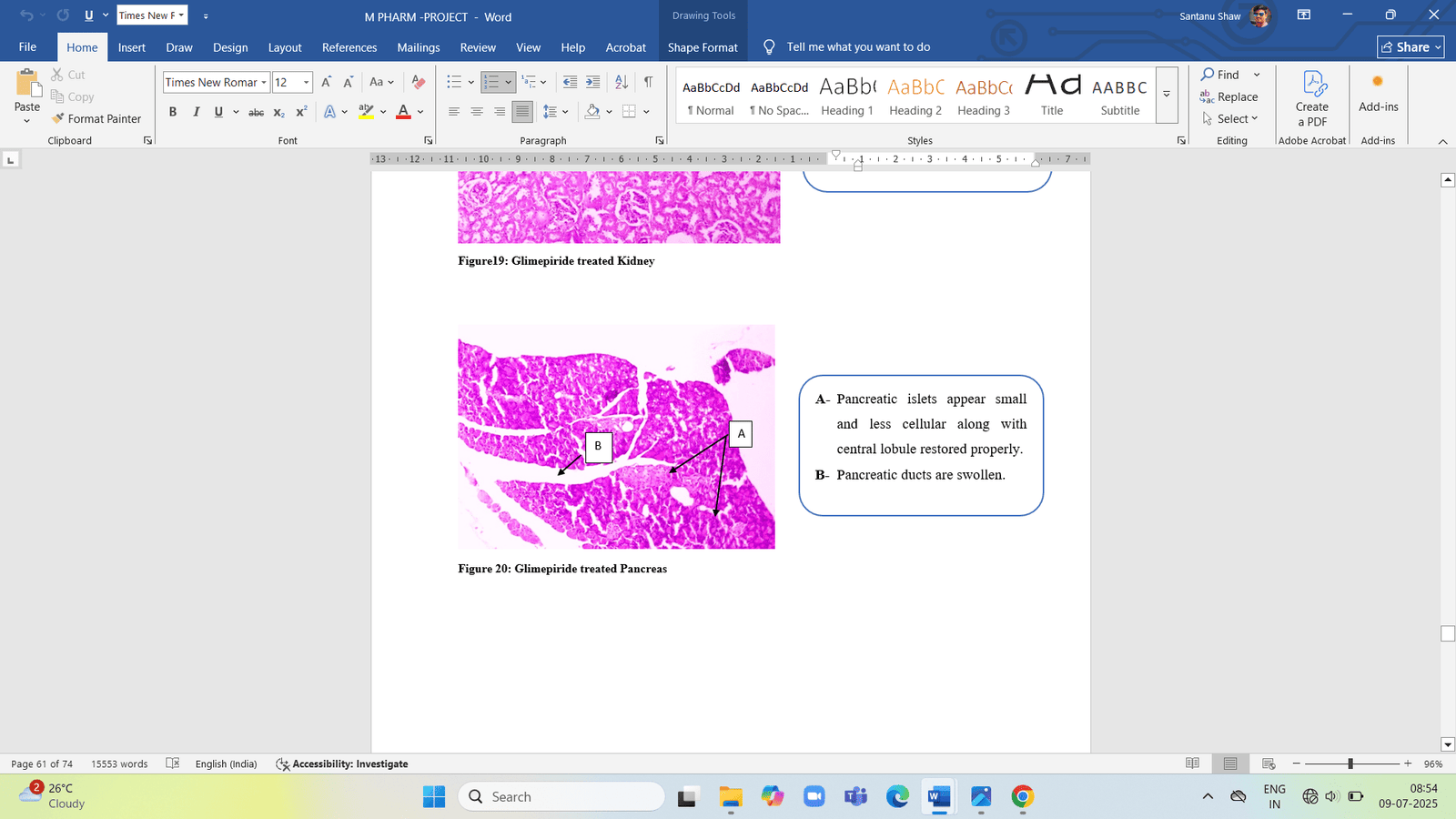
Fig. 14: Glimepiride treated group pancreas,
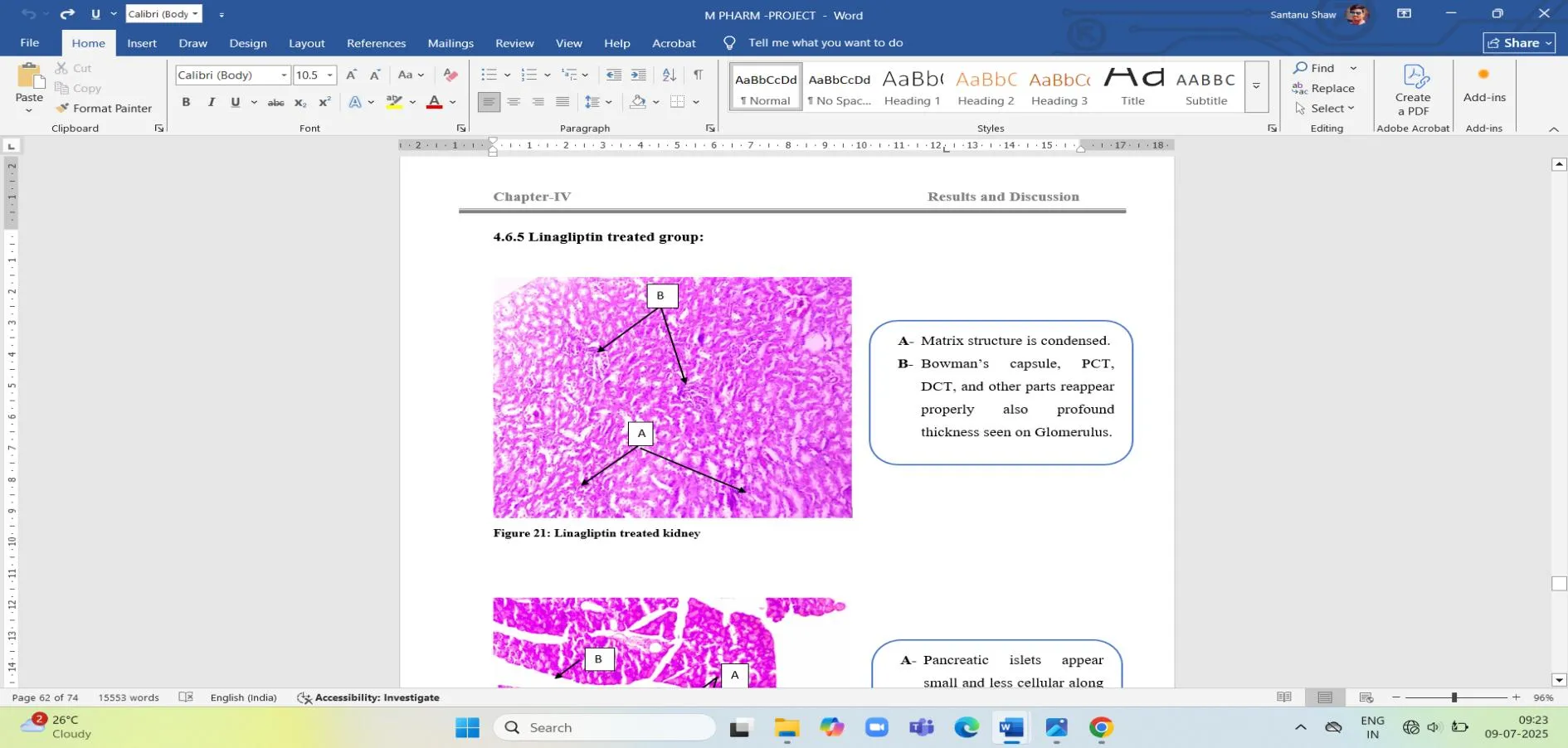
Fig. 15: Linagliptin treated group Kidney,
- Bowman’s capsule, PCT, DCT, and other parts reappear properly also
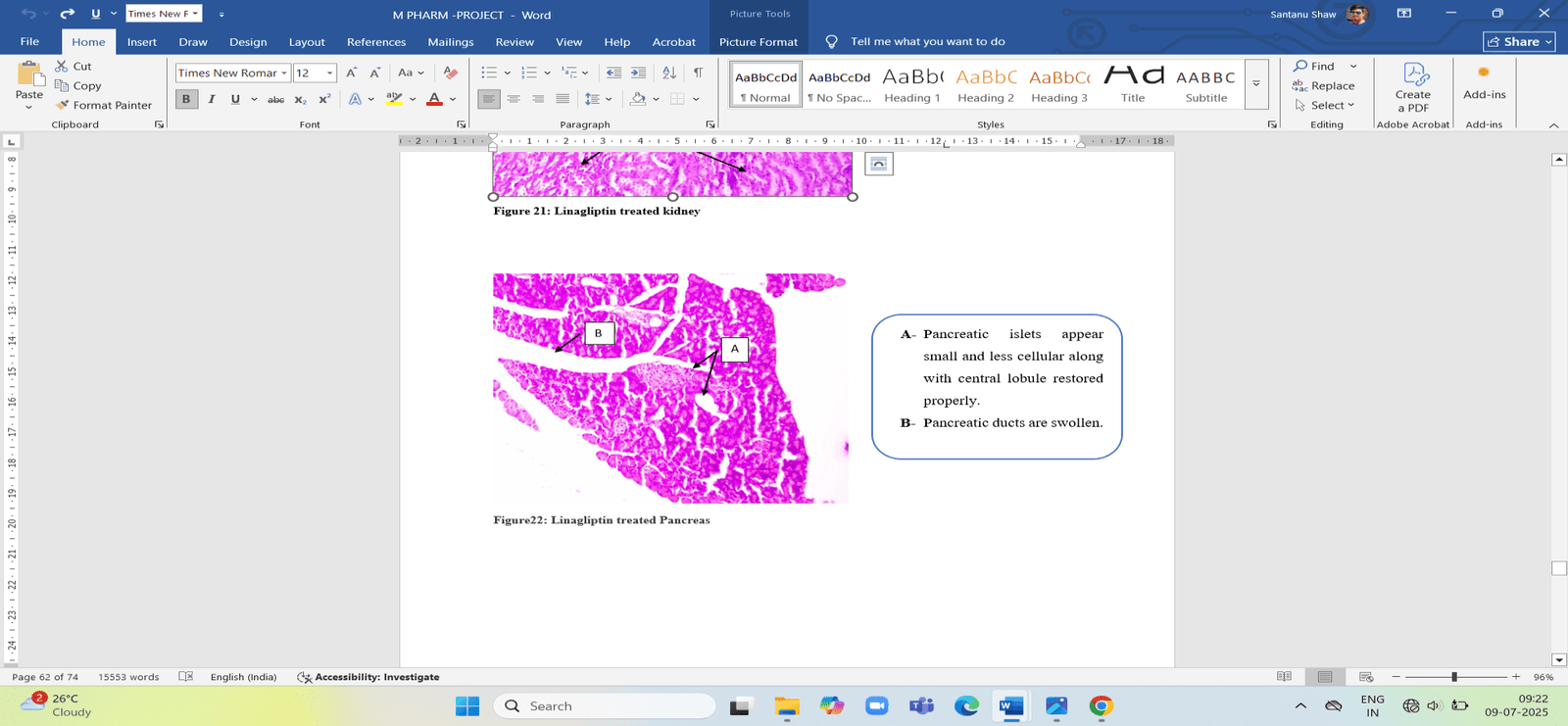
Fig. 16: Linagliptin treated group pancreas,
DISCUSSION: During this study, rats that were fed a high-fat diet for three to four months showed higher body weight and blood glucose levels, along with changes in kidney and cholesterol markers, which are linked to health issues. After receiving an injection of 35 mg/kg streptozotocin (STZ) into the abdomen, their fasting blood glucose rapidly increased to more than 250 mg/dl. The rats then showed signs like increased eating, drinking, and urination, and were classified as diabetic. Once type 2 diabetes was successfully induced, a diabetic model was created to test the effects of anti-diabetic drugs. Imeglimin dramatically reduced both fasting and post meal glucose levels, indicating that it was the most successful blood glucose regulator. Despite its effectiveness, Glimepiride primarily increases synthesis of insulin, which might lead to dangerously low blood glucose levels. Although Linagliptin has superior metabolic effects , it only slightly reduces blood sugar and improves HbA1c levels. The order for blood glucose management was: Imeglimin > Glimepiride > Linagliptin. Data on body weight revealed variations amongst the treatment groups. The body weight of the rats with diabetes caused by HFD and STZ was significantly higher than that of the control group. Body weight data showed differences between the treatment groups. The rats that were made diabetic through HFD and STZ had much higher body weight than the normal group. Imeglimin may help preventing weight gain in people with diabetes because it induced a moderate amount of weight loss. Glimepiride-treated rats initially put on weight before losing it indicating that it gradually made up with time. Similar weight loss was likewise brought on by Linagliptin. These findings imply that while all three medications assisted in managing weight, Imeglimin consistently controls weight, perhaps because it enhances insulin sensitivity. The lipid profile was best affected by Imeglimin. While increasing HDL, it dramatically reduced VLDL, LDL, trigyclerides and total cholesterol. Though Linagliptin had a small impact but still improved lipid matrices. On the other hand, Glimepiride showed the least improvement. The ranking for lipid levels was: Imeglimin > Linagliptin > Glimepiride. Tests of kidney function revealed that linagliptin had significant protective effects, lowering levels of urea, creatinine, and uric acid. While Glimperide had slight impact, Imeglimin was less successful than Linagliptin but still improved kidney function, while glimepiride had a modest effect. The order based on kidney health was: Linagliptin > Imeglimin > Glimepiride. After diabetes was brought on by HFD and STZ, there were significant alterations in kidney and pancreatic tissues; however the drug-treated groups showed differing degrees of improvement. These results declare that while Linagliptin is superior for kidney protection, Imeglimin is the best choice for blood glucose control, maintaining cholesterol levels and weight management. Further studies and clinical trials are required to test these findings in humans. Overall the entire study suggests that while Imeglimin is superior for lowering blood sugar and cholesterol, Linagliptin is an appropriate treatment for diabetes related kidney problems.
CONCLUSION
In this investigation, Wistar rats with type 2 diabetes caused by HFD + STZ were used to evaluate the effects of glimepiride, imeglimin, and linagliptin on organ and metabolic functioning. In addition to structural damage to the kidney and pancreatic tissues, diabetes induction causes high blood glucose, lipid abnormalities, and renal dysfunction. Overall, this study concluded that linagliptin is the greatest choice for kidney protection in diabetic conditions, whereas imeglimin is the best choice for improving lipid profiles and regulating blood glucose. The results demonstrate the therapeutic usefulness of these medications in the management of various type 2 diabetes symptoms and associated consequences. Further study, including clinical trials, is required to explore the long-term advantages of these medicines and validate these findings in human subjects. Imeglimin was found to have the greatest improvement in lipid indicators, which may indicate that it could help treat the dyslipidemia linked to type 2 diabetes. Linagliptin demonstrated the strongest nephroprotective effects due to its anti-inflammatory and antioxidative characteristics. Imeglimin is the most effective at promoting metabolic recovery and preventing weight loss, which demonstrates its importance in energy balance and mitochondrial function.
ACKNOWLEDGEMENT: The authors are thankful to the Management of Bengal School of Technology, Delhi Road, Sugandha, Hooghly-712102, for the financial support to carry this work. I am thankful to Mr. Biswanath Das Lab assistant. Also thankful to Mrs. Samina Banu for procurement of lots of chemicals and thankful to my beloved research mates. I also thankful to my supervisorsfor pursuing this titled work.
CONFLICT OF INTEREST: This research work is ethically permitted by IAEC-CPCSEA Bengal School of Technology, West Bengal, India. The authors declare that there is no conflict of interest.
FUNDING SOURCE: The whole work is funded by Bengal School of Technology, West Bengal, India.
REFERENCES




Santanu Shaw1, Sayantika Kundu2, Debkantha Gope2*, Sayani Debnath3, Comparative Evaluation Of Imeglimin, Glimepiride & Linagliptin In The Management Of Type-II Diabetes Induced By A High-Fat Diet (HFD) Combined With Low-Dose Streptozotocin (STZ) On Albino Wistar Rats., Int. J. Sci. R. Tech., 2026, 3 (6), 1515-1527. https://doi.org/10.5281/zenodo.20846387
 10.5281/zenodo.20846387
10.5281/zenodo.20846387