
We use cookies to ensure our website works properly and to personalise your experience. Cookies policy
R.G Sapkal College of Pharmacy, Sapkal Knowledge Hub, Kalyani Hills, Anjaneri, Trimbakeshwar Rd, Nashik, 422213, Maharashtra, India.
Rifaximin is a poorly absorbed rifamycin antibiotic widely used in the treatment of gastrointestinal disorders such as Traveler's Diarrhea, Irritable Bowel Syndrome with Diarrhea (IBS-D), Hepatic Encephalopathy, and Small Intestinal Bacterial Overgrowth (SIBO). Due to its localized action within the gastrointestinal tract, targeted delivery of rifaximin to the small intestine can improve therapeutic efficacy and reduce premature drug release in the stomach. The present study aimed to formulate, develop, and evaluate enteric-coated rifaximin pellets for targeted small intestinal delivery using a multiparticulate drug delivery approach. Preformulation studies including organoleptic evaluation, solubility study, melting point determination, Fourier Transform Infrared Spectroscopy (FTIR), and calibration curve preparation were carried out to assess the physicochemical characteristics and compatibility of rifaximin with selected excipients. Drug-loaded pellets were prepared by layering rifaximin onto sugar spheres using Hydroxypropyl Methylcellulose (HPMC E5) as a binder in a fluidized bed processor. A barrier coating was subsequently applied using HPMC E5 to prevent interaction between the drug layer and enteric coating polymer. Enteric coating was performed using Eudragit® L30D-55 as the enteric polymer, Diethyl Phthalate as a plasticizer, Tween 80 as a surfactant, and Talc as an anti-tacking agent. Formulation optimization was carried out through the preparation of multiple trial batches, and the optimized formulation was selected based on assay, acid resistance, and dissolution performance. Quality by Design (QbD) principles were applied to identify Critical Quality Attributes (CQAs), Critical Material Attributes (CMAs), and Critical Process Parameters (CPPs) affecting product quality. The prepared pellets were evaluated for percentage yield, particle size distribution, bulk density, tapped density, Carr's Index, Hausner Ratio, angle of repose, friability, moisture content, drug content, assay, enteric resistance, and in-vitro dissolution behavior. The optimized formulation exhibited satisfactory physicochemical properties, excellent flow characteristics, low friability, high drug content uniformity, and acceptable assay values. The enteric-coated pellets demonstrated excellent resistance in acidic medium with minimal drug release during the acid stage and more than 80% drug release in phosphate buffer pH 6.8, confirming successful intestinal targeting. The results of the study indicated that Eudragit® L30D-55-based enteric-coated rifaximin pellets can effectively protect the drug from gastric conditions and provide targeted drug release in the small intestine. Therefore, the developed multiparticulate pellet system represents a promising approach for improving the therapeutic performance of rifaximin intended for intestinal delivery.
Oral drug delivery system (ODDS) is the most commonly used and preferred route for administration of drugs through the mouth for local or systemic action. It is considered the most convenient route because of its ease of administration, patient compliance, safety, cost-effectiveness, and flexibility in formulation development. The majority of pharmaceutical products available in the market are designed for oral administration.
In an oral drug delivery system, the drug is administered through the gastrointestinal tract (GIT), where it undergoes disintegration, dissolution, absorption, and finally reaches the systemic circulation to produce the desired therapeutic effect. Oral dosage forms include tablets, capsules, pellets, powders, granules, suspensions, emulsions, and solutions.
The oral route is widely accepted because it is non-invasive and does not require specialized personnel for administration. It also offers better patient compliance compared to parenteral dosage forms. Oral formulations can be designed to provide immediate release, sustained release, delayed release, controlled release, or targeted drug delivery depending on the therapeutic requirement.
Modified Release Drug Delivery System
Modified Release Drug Delivery Systems (MRDDS) are pharmaceutical formulations designed to alter the rate, time, and/or place of drug release compared to conventional immediate-release dosage forms. These systems are developed to improve therapeutic efficacy, enhance patient compliance, reduce dosing frequency, and minimize adverse effects associated with fluctuations in drug concentration.
In conventional dosage forms, the drug is released immediately after administration, resulting in rapid absorption and fluctuations in plasma drug concentration. Modified release systems are specifically designed to maintain drug concentration within the therapeutic window for a prolonged period, thereby improving treatment outcomes and reducing side effects.
Modified release formulations can be classified into sustained-release, controlled-release, delayed-release, extended-release, repeat-action, and targeted-release systems. Sustained-release formulations release the drug slowly over an extended period, whereas controlled-release systems release the drug at a predetermined rate. Delayed-release systems, such as enteric-coated formulations, release the drug after a specific lag time or at a particular site within the gastrointestinal tract.
Multiparticulate Drug Delivery System
Multiparticulate Drug Delivery Systems (MDDS) are oral dosage forms composed of numerous small, discrete units such as pellets, granules, beads, microspheres, or mini-tablets. These individual units are administered together in a capsule, sachet, or compressed tablet and function as multiple drug delivery entities within the gastrointestinal tract.
Unlike single-unit dosage forms, multiparticulate systems distribute uniformly throughout the gastrointestinal tract after administration. This uniform distribution reduces the risk of local irritation, minimizes dose dumping, and provides more consistent drug absorption. As a result, multiparticulate systems often exhibit improved therapeutic performance compared to conventional tablets and capsules.
Pellets Definition
Pellets are small, free-flowing, spherical or semi-spherical solid particulate dosage forms typically ranging in size from 500 to 1500 μm. They are composed of active pharmaceutical ingredients (APIs) and excipients and are produced using techniques such as Pelletization layering, balling, or spray drying. Pellets can be filled into capsules or compressed into tablets and are widely used for immediate-release, sustained-release, delayed-release, and targeted drug delivery systems.
Pelletization is a process that converts fine powders or granules into spherical units with uniform size and shape. Due to their excellent flow properties and uniform distribution in the gastrointestinal tract, pellets have become one of the most preferred multiparticulate drug delivery systems in pharmaceutical formulation development.
1. Materials used
The materials, chemicals, and reagents used in the formulation development and analytical work of the present study, along with their respective grades and sources, are summarized in table
|
Sr. No. |
Material, Chemical |
Grade, Purity |
Source, Manufacturer |
|
1 |
Rifaximin |
API, Pharmaceutical Grade |
Lupin, Sun Pharma |
|
2 |
Microcrystalline Cellulose (MCC PH101/102) |
Pharmaceutical Grade |
FMC Bio Polymer |
|
3 |
Sugar Spheres |
Pharmaceutical Grade |
Colorcon |
|
4 |
PVP K30 |
Pharmaceutical Grade |
SD Fine-Chem |
|
5 |
HPMC E5 |
Pharmaceutical Grade |
Colorcon |
|
6 |
Eudragit L100-55 |
Enteric Coating Grade |
Evonik |
|
7 |
Triethyl Citrate |
Plasticizer |
Merck |
|
8 |
Talc |
Pharmaceutical Grade |
SD Fine-Chem |
|
9 |
Isopropyl Alcohol (IPA) |
AR Grade |
Merck |
|
10 |
Methanol |
HPLC Grade |
Merck |
|
11 |
Ethanol |
AR Grade |
Merck |
|
12 |
Hydrochloric Acid (0.1 N HCl) |
AR Grade |
Merck |
|
13 |
Phosphate Buffer pH 6.8 |
Prepared in Laboratory |
In- house |
|
14 |
Potassium Bromide (KBr) |
Spectroscopic Grade |
Merck |
|
15 |
Purified Water |
Analytical Grade |
In- house |
Table no. 1 Materials used
2. Instruments and Equipment
All instruments and equipment used during the study were calibrated and qualified prior to use, and equipment qualification records were maintained throughout. The complete list of instruments and equipment.
|
Sr. No. |
Instrument, Equipment |
Make, Model |
Application |
|
1 |
UV-Visible Spectrophotometer |
Jasco V-550, with Spectra manager software |
UV spectroscopic analysis, Drug estimation |
|
2 |
FTIR Spectrophotometer |
Shimadzu IRAffinity-1 |
FTIR spectroscopic, Drug-excipient compatibility |
|
3 |
Melting point Apparatus |
Open capillary method Apparatus |
Malting point determination of rifaximin |
|
4 |
Analytical Balance |
Shimadzu/Labman |
Accurate weighing |
|
5 |
Digital pH Meter |
Systronics |
pH measurement |
|
6 |
Magnetic Stirrer with Hot Plate |
Remi |
Solution preparation |
|
7 |
Fluidized Bed Processor/Coater |
Gansons/Equivalent |
Enteric coating |
|
8 |
Tray Dryer |
Laboratory Model |
Drying of pellets |
|
9 |
Sieve Shaker |
Standard Sieves |
Pellet size analysis |
|
10 |
Digital Vernier Caliper |
Mitutoyo |
Pellet diameter measurement |
|
11 |
Friability Tester |
Roche |
Pellet strength evaluation |
|
12 |
USP Dissolution Test Apparatus Type II |
___ |
In vitro drug release |
|
13 |
USP Disintegration Apparatus |
___ |
Disintegration study |
|
14 |
Stability Chamber |
40±2°C/75±5% RH |
Stability studies |
|
15 |
Bulk Density Apparatus |
Laboratory Model |
Flow property evaluation |
|
16 |
Design Expert Software |
Version 13/11 |
QbD and statistical optimization |
Table no.2 Instruments and Equipment
EXPERIMENTAL WORK
1. Organoleptic Properties
The organoleptic properties of rifaximin were evaluated to confirm the identity and physical characteristics of the drug sample. The drug was found to be an orange-red crystalline powder with a characteristic appearance and no objectionable odour. The observed properties were in agreement with the reported literature values.
|
Parameter |
Observation |
|
Colour |
Orange-Reddish |
|
Odour |
Characteristic |
|
Appearance |
Crystalline Powder |
Table no.3 Organoleptic Properties of Rifaximin
Solubility Study
The solubility of rifaximin was determined in various solvents. The drug exhibited poor aqueous solubility and was found to be practically insoluble in water, confirming its BCS Class IV nature.
|
Solvent |
Observation |
|
Water |
Practically Insoluble |
|
Methanol |
Slightly Soluble |
|
Ethanol |
Slightly Soluble |
|
Acetone |
Soluble |
|
DMSO |
Freely Soluble |
|
Phosphate Buffer pH 6.8 |
Slightly Soluble |
Table no. 4 Solubility Profile of Rifaximin
The poor aqueous solubility of rifaximin justified the development of a specialized pellet-based delivery system for targeted intestinal drug release.
Melting Point Determination
The melting point of rifaximin was determined using the capillary method and compared with the reported literature value.
|
Parameter |
Value |
|
Reported Melting Point |
198–202°C |
|
Observed Melting Point |
200 ± 2°C |
Table no.5 Melting Point of Rifaximin
The observed melting point was found to be within the reported range, indicating purity of the drug sample.
UV spectrophotometric analysis
The UV-Visible spectrophotometric analysis of Rifaximin was carried out using a Jasco Corporation, Japan, V-550 spectrophotometer with Spectra Manager software. Methanol was used as the solvent system for both the blank and the sample preparations. A 20 µg/mL solution of Rifaximin was scanned, and the wavelength of maximum absorption (max) was found to be 290 nm.
The UV absorption spectrum of Rifaximin was obtained using a Jasco Corporation, Japan, V-550 UV-Visible Spectrophotometer equipped with Spectra Manager software. All glassware used was thoroughly cleaned with double distilled water and dried before use. Analytical grade reagents were used throughout the study, and methanol was selected as the solvent due to the solubility of Rifaximin.
For the determination of the UV spectrum, 10 mg of Rifaximin was accurately weighed and dissolved in methanol, and the volume was made up to 10 mL to obtain a stock solution of 1000 µg/mL. From this stock solution, 0.2 mL was withdrawn and diluted to 10 mL with methanol to obtain a working solution of 20 µg/mL. The solution was scanned over the wavelength range of 200–400 nm to determine the wavelength of maximum absorbance (λmax). The λmax of Rifaximin was found at approximately 290 nm.
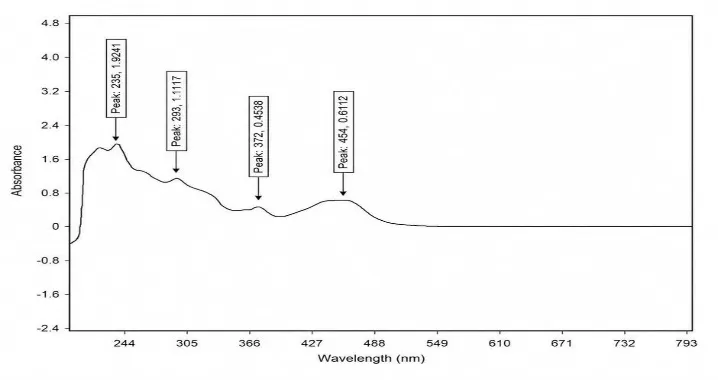
Figure no.1 UV spectrophotometric of Rifaximin drug
This figure presents the UV absorption spectrum of pure methanol, scanned over the relevant wavelength range and used as the reference blank for all subsequent spectrophotometric
measurements. The spectrum shows a flat baseline with negligible absorbance across the scanned range, confirming the absence of any interfering absorption from the solvent itself in the region of interest around 290 nm.
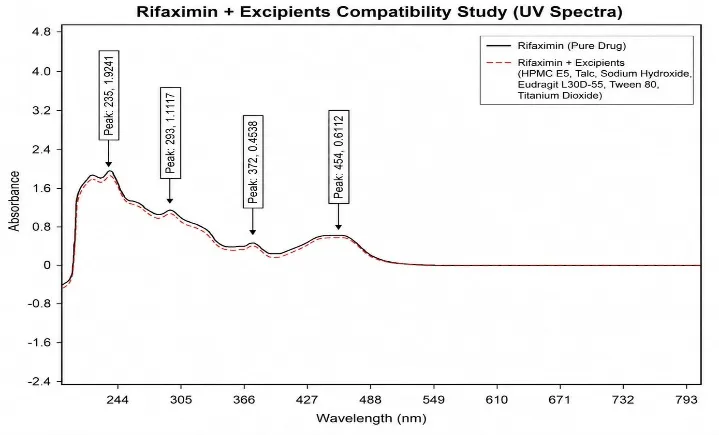
Figure no.2 UV spectrophotometric of Rifaximin drug + Excipients
Calibration Curve of Rifaximin in Methanol
A calibration curve of Rifaximin was prepared in methanol. A stock solution containing 1000 µg/mL was prepared by dissolving 10 mg of Rifaximin in 10 mL of methanol. From this stock solution, 1 mL was transferred into a 10 mL volumetric flask and diluted to volume with methanol to obtain Solution A (100 µg/mL).
Aliquots of 0.5, 1.0, 1.5, 2.0, and 2.5 mL were withdrawn from Solution A and diluted to 10 mL with methanol to obtain concentrations of 5, 10, 15, 20, and 25 µg/mL (ppm), respectively. The absorbance of each solution was measured at 290 nm against methanol as a blank. A calibration curve was plotted by taking concentration (µg/mL) on the X-axis and absorbance on the Y-axis. The calibration curve showed good linearity over the selected concentration range
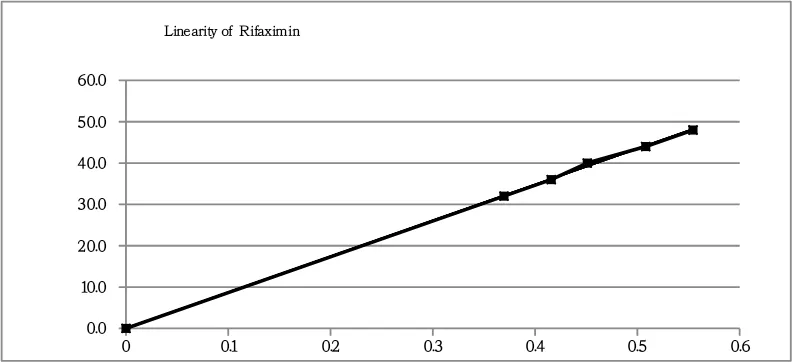
Figure no.3 Calibration Curve of Rifaximin in Methanol
FTIR Analysis of Rifaximin
The Fourier Transform Infrared (FTIR) spectrum of Rifaximin was recorded using a Shimadzu IRAffinity-1 FTIR spectrophotometer. The spectrum was recorded using the potassium bromide (KBr) pellet method, with KBr used as the blank. The spectrum was scanned over the range of 4000–400 cm⻹ at a resolution of 4 cm⻹. The characteristic absorption peaks obtained for Rifaximin were compared with the reported reference spectrum to confirm the identity, purity, and integrity of the drug. The FTIR analysis was also performed to evaluate the compatibility of Rifaximin with the selected excipients used in the formulation of enteric-coated pellets by comparing the spectra of the pure drug, excipients, and their physical mixture.
Saturation Solubility of Rifaximin in Methanol, Water, 0.1 N HCl and Phosphate Buffer pH 6.8
The saturation solubility of Rifaximin in methanol, distilled water, 0.1 N hydrochloric acid (HCl), and phosphate buffer pH 6.8 was determined by the shake-flask method. An excess amount of Rifaximin (approximately 50–100 mg) was added separately into glass vials containing 10 mL of each solvent. The vials were tightly sealed, labelled, and placed in an orbital shaker maintained at 25 ± 0.5°C with continuous shaking at 100 rpm for 48 hours to achieve equilibrium.
After equilibrium was attained, 1 mL of the supernatant solution was withdrawn from the middle layer of each vial and centrifuged at 5000 rpm for 10 minutes. The clear supernatant was filtered through a 0.45 µm syringe filter (PTFE filter for methanol and Nylon/PES filter for aqueous media). The filtrates were suitably diluted, wherever required, and analyzed using the validated UV–Visible spectrophotometric method at 290 nm. The concentration of dissolved Rifaximin was calculated from the calibration curve, and the saturation solubility in each solvent was expressed as mg/mL.
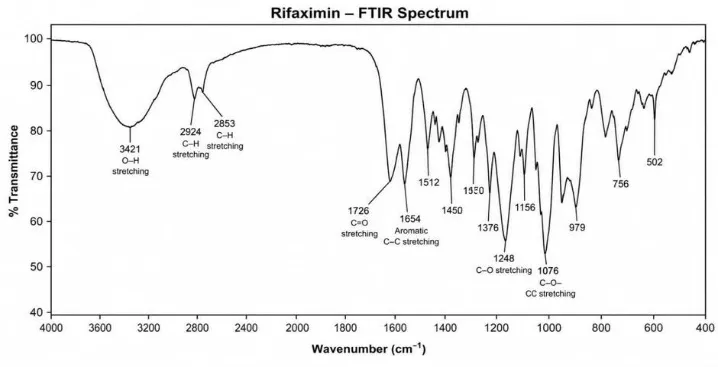
Figure no. 4 FTIR Analysis of Rifaximin
FTIR spectroscopy was performed to investigate possible interactions between rifaximin and formulation excipients. The characteristic peaks of rifaximin were retained in the optimized formulation, indicating the absence of significant drug-excipient interactions
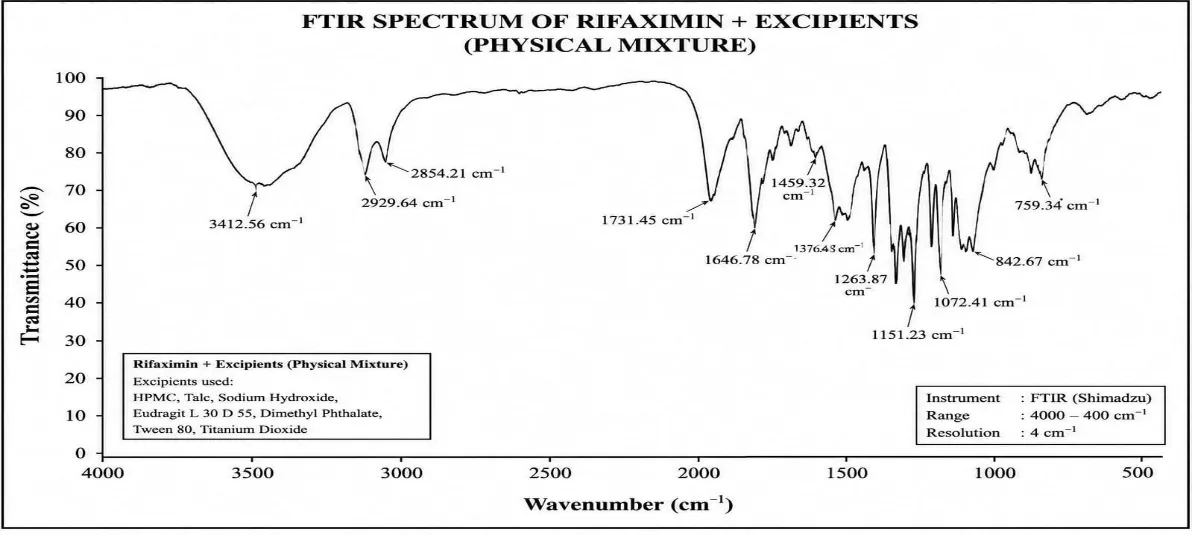
Figure no. 5 FTIR Analysis of Rifaximin + Excipients
FTIR spectra of pure rifaximin, physical mixtures of rifaximin with excipients, and the optimized enteric-coated pellet formulation were recorded using an FTIR spectrophotometer. The samples were prepared by the KBr pellet method and scanned over the spectral range of 4000–400 cm⻹. The obtained spectra were analysed for the presence of characteristic functional group peaks and any possible drug–excipient interactions.
|
Functional Group |
Characteristic Peak (cm⻹) |
Rifaximin + Excipients (cm⻹) |
|
O–H Stretching |
3412–3500 |
3400,2930,1650,1600,1240,1050 |
|
C–H Stretching |
2920–2950 |
2950,1730,1450 |
|
C=O Stretching |
1731–1770 |
1725,1600,1280,1120 |
|
Aromatic C=C Stretching |
1664–1680 |
1640,1600 |
|
CH bending |
1450–1460 |
1450.76 |
|
C–O Stretching |
1100–1300 |
1200,1100 |
|
C–O–C Stretching |
1050–1160 |
1050,1040,100 |
|
C–H Stretching |
2800–3000 |
2890.72 |
Table no. 6 FTIR Analysis of Rifaximin + Excipients
RESULTS
FORMULATION DEVELOPMENT RESULTS
Trial Batch Observations
Nine trial batches (F1–F9) were prepared by varying the concentration of enteric coating polymer and coating composition. The prepared pellets were evaluated for acid resistance, drug release, assay, and physical appearance.
|
Batch |
Assay (%) |
Acid Resistance (%) |
Drug Release at 6 h (%) |
Observation |
|
F1 |
91.42 |
76.85 |
96.52 |
Poor acid resistance |
|
F2 |
92.85 |
81.36 |
95.20 |
Insufficient coating |
|
F3 |
94.10 |
85.72 |
94.18 |
Moderate protection |
|
F4 |
96.24 |
89.65 |
93.42 |
Acceptable |
|
F5 |
97.36 |
93.28 |
91.85 |
Good performance |
|
F6 |
98.12 |
95.84 |
90.74 |
Improved protection |
|
F7 |
99.05 |
97.26 |
89.63 |
Better coating integrity |
|
F8 |
99.42 |
98.15 |
88.24 |
Slightly delayed release |
|
F9 |
99.84 |
99.12 |
87.56 |
Optimum performance |
Table no.7 Trial Batch Observations
The results demonstrated that increasing the concentration of Eudragit® L30D-55 improved acid resistance and reduced premature drug release in acidic media.
Optimized Batch (F9)
|
Parameter |
Result |
|
Assay (%) |
99.84 |
|
Drug Content (%) |
99.52 |
|
Acid Resistance (%) |
99.12 |
|
Drug Release in Acid Stage (%) |
1.20 |
|
Drug Release in Buffer Stage (%) |
87.56 |
|
Friability (%) |
0.38 |
|
Moisture Content (%) |
2.58 |
Table no.8 Optimized Batch (F9)
F9 can be justified as the optimized batch because it shows:
1. Drug loading result
Drug loading was successfully performed on sugar spheres using a fluidized bed processor equipped with a Wurster insert. The prepared drug-loaded pellets exhibited uniform appearance, smooth surface morphology, and satisfactory flow characteristics. No agglomeration or sticking was observed during the drug layering process. The percentage yield of drug-loaded pellets ranged from 91.25% to 99.12%, indicating efficient processing conditions.
|
Batch |
% Yield |
Drug Content (%) |
Observation |
|
F1 |
91.25 |
91.45 |
Uniform Layering |
|
F2 |
92.14 |
92.38 |
Uniform Layering |
|
F3 |
93.42 |
94.12 |
Good Layering |
|
F4 |
94.36 |
95.24 |
Good Layering |
|
F5 |
95.12 |
96.85 |
Uniform Layering |
|
F6 |
96.04 |
97.54 |
Smooth Surface |
|
F7 |
97.25 |
98.26 |
Smooth Surface |
|
F8 |
98.15 |
99.05 |
Excellent Layering |
|
F9 |
99.12 |
99.72 |
Excellent Layering |
Table no. 9 Drug loading result
The results confirmed successful deposition of rifaximin onto the sugar sphere surface with acceptable content uniformity.
2. Barrier Coating Results
Barrier coating was applied to prevent direct interaction between rifaximin and the enteric coating polymer. The HPMC E5-based barrier coating produced a smooth and uniform film around the drug-loaded pellets. No cracking, peeling, or agglomeration was observed during the coating process.
|
Batch |
Weight Gain (%) |
Coating Uniformity |
Observation |
|
F1 |
3.5 |
Good |
Uniform Coating |
|
F2 |
3.8 |
Good |
Uniform Coating |
|
F3 |
4.0 |
Good |
Smooth Surface |
|
F4 |
4.2 |
Very Good |
Uniform Surface |
|
F5 |
4.5 |
Very Good |
Smooth Coating |
|
F6 |
4.8 |
Very Good |
Uniform Coating |
|
F7 |
5.0 |
Excellent |
Smooth Surface |
|
F8 |
5.2 |
Excellent |
Uniform Film |
|
F9 |
5.5 |
Excellent |
Optimum Coating |
Table no.10 Barrier Coating Results
The barrier coating layer effectively separated the drug layer from the enteric coating and improved overall coating integrity.
3. Enteric Coating Results
Enteric coating was successfully applied using Eudragit® L30D-55. The coated pellets exhibited excellent appearance, smooth surface, and adequate coating integrity. Acid resistance improved with increasing enteric polymer concentration.
|
Batch |
Coating Weight Gain (%) |
Acid Resistance (%) |
|
F1 |
10.2 |
76.85 |
|
F2 |
11.4 |
81.36 |
|
F3 |
12.6 |
85.72 |
|
F4 |
13.8 |
89.65 |
|
F5 |
15.0 |
93.28 |
|
F6 |
16.2 |
95.84 |
|
F7 |
17.4 |
97.26 |
|
F8 |
18.6 |
98.15 |
|
F9 |
20.0 |
99.12 |
Table no. 11 Enteric Coating Results
The results demonstrated that increasing enteric coating level improved gastric resistance and minimized premature drug release in acidic media.
4. Dissolution Results
The dissolution study was performed in two stages consisting of an acid stage (0.1 N HCl for 2 hours) followed by a buffer stage (pH 6.8 phosphate buffer). The enteric-coated pellets exhibited excellent resistance to acidic conditions and released the drug predominantly in intestinal pH
|
Batch |
Drug Release in Acid Stage (%) |
Drug Release in Buffer Stage (%) |
|
F1 |
1.08 |
98.98 |
|
F2 |
3.17 |
98.97 |
|
F3 |
1.19 |
96.49 |
|
F4 |
1.66 |
96.22 |
|
F5 |
2.91 |
96.11 |
|
F6 |
2.55 |
98.61 |
|
F7 |
1.59 |
98.82 |
|
F8 |
3.10 |
98.02 |
|
F9 |
0.45 |
100.70 |
Table no.12. Dissolution Results
In-Vitro Dissolution Study
The in vitro dissolution study of rifaximin enteric-coated pellets was carried out using the USP Dissolution Apparatus Type II (Paddle) to evaluate the drug release behavior under simulated gastrointestinal conditions.
A quantity of pellets equivalent to the required dose of rifaximin was placed in the dissolution vessel containing 900 mL of 0.1 N hydrochloric acid (pH 1.2) maintained at 37 ± 0.5°C and stirred at 50 rpm. The pellets were exposed to the acidic medium for 2 hours to assess the integrity of the enteric coating and acid resistance.
|
Batch |
Drug Release in Acid Stage (%) |
Drug Release in Buffer Stage (%) |
|
F1 |
1.08 |
98.98 |
|
F2 |
3.17 |
98.97 |
|
F3 |
1.19 |
96.49 |
|
F4 |
1.66 |
96.22 |
|
F5 |
2.91 |
96.11 |
|
F6 |
2.55 |
98.61 |
|
F7 |
1.59 |
98.82 |
|
F8 |
3.10 |
98.02 |
|
F9 |
0.45 |
100.70 |
Table no. 13 In-Vitro Dissolution Study
Overall Performance of Optimized Batch (F9)
Ased on all evaluation parameters, formulation F9 was identified as the optimized batch. The formulation demonstrated excellent processability, superior acid resistance, acceptable assay, satisfactory dissolution profile, and desired intestinal targeting characteristics.
QUALITY BY DESIGN (QBD)
Quality by Design (QbD) is a systematic, science-based, and risk-based approach to pharmaceutical product development introduced by the International Council for Harmonisation (ICH Q8 guideline). QbD emphasizes building quality into the product during development rather than relying solely on end-product testing. The approach begins with predefined objectives and focuses on understanding the relationship between formulation variables, manufacturing processes, and product performance.
The fundamental principle of QbD is that product quality should be designed and developed into the formulation from the beginning. It involves identification of Quality Target Product Profile (QTPP), Critical Quality Attributes (CQAs), Critical Material Attributes (CMAs), Critical Process Parameters (CPPs), risk assessment, design of experiments (DoE), establishment of design space, and implementation of a control strategy.
Application of QbD in the development of enteric-coated rifaximin pellets helps in achieving robust formulation performance, consistent product quality, improved process understanding, reduced variability, and regulatory flexibility. The systematic optimization of formulation and process variables ensures targeted drug release in the small intestine and reproducible manufacturing performance
1. Quality Target Product Profile (QTPP)
The Quality Target Product Profile defines the desired quality characteristics of the final product that are necessary to ensure safety and efficacy.
|
QTPP Element |
Target |
|
Dosage Form |
Enteric Coated Pellets |
|
Route of Administration |
Oral |
|
Drug Release |
Intestinal Release |
|
Assay |
90–110% |
|
Acid Resistance |
NMT 10% |
|
Dissolution |
NLT 80% |
Table no. 14. Quality Target Product Profile (QTPP)
2. Critical Quality Attributes (CQAs)
Critical Quality Attributes are the physical, chemical, biological, or microbiological properties that must remain within predefined limits to ensure product quality
|
CQA |
Target |
|
Assay |
90–110% |
|
Drug Content Uniformity |
Uniform |
|
Dissolution |
NLT 80% |
|
Pellet Size |
Desired Range |
|
Acid Resistance |
Pass |
Tablet no. 15 Critical Quality Attributes (CQAs)
3. Risk Assessment
Risk assessment was performed to identify formulation and process variables that could significantly affect the quality of enteric-coated rifaximin pellets. The assessment was carried out using Ishikawa (Fishbone) analysis.
The major sources of variability were categorized into:
4. Critical Material Attributes (CMAs)
|
CMA |
Impact |
|
Rifaximin |
High |
|
HPMC E5 |
Medium |
|
Eudragit L30D-55 |
High |
|
Talc |
Low |
Table no. 16 Critical Material Attributes (CMAs)
5 Critical Process Parameters (CPPs)
|
CPP |
Impact |
|
Spray Rate |
High |
|
Inlet Temperature |
Medium |
|
Atomization Pressure |
High |
|
Product Temperature |
High |
Table no.17 Critical Process Parameters (CPPs)
DESIGN OF EXPERIMENT (DOE)
Design of Experiment was employed to evaluate the influence of critical formulation and process variables on product performance and to establish an optimized formulation
1. Independent Variables
|
Factor |
Low (-1) |
Medium (0) |
High (+1) |
|
X1 = Eudragit L30D-55 Level (%) |
20 |
25 |
30 |
|
X2 = Spray Rate (g/min) |
2 |
4 |
6 |
Table no.18 Independent Variables
2. Dependent Variables (Responses)
Y2 = MOISTURE CONTENT
|
Source |
Sum of Squares |
df |
Mean Square |
F-value |
p-value |
|
|
Model |
6.12 |
2 |
3.06 |
70.44 |
< 0.0001 |
significant |
|
A-Eudragit |
4.47 |
1 |
4.47 |
102.75 |
< 0.0001 |
|
|
B-diethyl pharate |
1.66 |
1 |
1.66 |
38.12 |
0.0008 |
|
|
Residual |
0.2608 |
6 |
0.0435 |
|
|
|
|
Cor Total |
6.38 |
8 |
|
|
|
|
3. Design Space
Design space represents the multidimensional combination of formulation variables and process parameters that consistently provide the desired product quality.
The optimized design space was established based on response surface analysis and contour plot interpretation. Operating within the design space ensures consistent quality, robust process performance, and regulatory flexibility
|
Run |
Eudragit (%) |
Diethyl Phthalate (%) |
Y1: Moisture Content (%) |
|
1 |
32.0711 |
15.0000 |
2.12 |
|
2 |
20.0000 |
10.0000 |
4.25 |
|
3 |
25.0000 |
7.9289 |
3.98 |
|
4 |
30.0000 |
10.0000 |
3.12 |
|
5 |
20.0000 |
20.0000 |
3.56 |
|
6 |
25.0000 |
15.0000 |
2.86 |
|
7 |
25.0000 |
22.0711 |
2.65 |
|
8 |
17.9289 |
15.0000 |
4.48 |
|
9 |
30.0000 |
20.0000 |
2.05 |
Table no.19 Design Space
A control strategy was developed to ensure consistent manufacturing and maintenance of product quality throughout the production process.
4. Control Strategy
|
Parameter |
Operating Range |
|
Inlet Temperature |
40–45°C |
|
Spray Rate |
2–6 g/min |
|
Atomization Pressure |
1.5–2.0 bar |
|
Product Temperature |
30–35°C |
Table no.20 Control Strategy
The established control strategy ensures reproducible pellet quality, effective enteric coating performance, desired acid resistance, and targeted intestinal drug release.
Stability Studies
Evaluation of the optimized formulation (F9) under stress conditions to ensure shelf-life and efficacy.
ICH Q1A (R2) GUIDELINES The stability study was conducted to evaluate the physical and chemical integrity of the optimized enteric-coated Rifaximin pellets.
Batch: Optimized Formulation (F9)
Conditions: 40°C ± 2°C / 75% RH ± 5% RH
|
Parameters |
Initial (O Month) |
After 1 Month |
After 3 Months |
|
Appearance |
Orange-Red Pellets |
No Change |
No Change |
|
Assay (%) |
99.84 ± 0.12 |
99.62 ± 0.21 |
99.45 ± 0.18 |
|
Acid Resistance (%) |
99.12 ± 0.05 |
98.95 ± 0.11 |
98.72 ± 0.14 |
|
Drug Content (%) |
99.52 ± 0.15 |
99.30 ± 0.08 |
99.18 ± 0.22 |
|
Friability (%) |
0.38 ± 0.02 |
0.40 ± 0.03 |
0.42 ± 0.01 |
Table no.21 Stability study
CONCLUSION
The present investigation successfully accomplished the formulation, development, optimization, and evaluation of enteric-coated rifaximin pellets intended for targeted small intestinal drug delivery.
Preliminary characterization studies confirmed the purity and suitability of rifaximin for formulation development. Drug-excipient compatibility studies established the absence of significant interactions between the drug and selected formulation components, supporting
their use in the preparation of enteric-coated pellets.
The implementation of the Quality by Design (QbD) approach facilitated the systematic identification and control of critical formulation and process variables. Design of Experiments (DoE) and statistical optimization using Design-Expert software enabled the development of an optimized formulation with reproducible quality attributes.
The pellet formulation process, including drug layering, barrier coating, enteric coating with Eudragit® L30D-55, drying, and curing, was successfully optimized to obtain pellets with desirable pharmaceutical properties.
The optimized enteric-coated rifaximin pellets exhibited satisfactory flow characteristics, acceptable mechanical strength, uniform particle size distribution, low friability, high drug content, efficient coating, and excellent acid resistance. The enteric coating effectively protected the drug from gastric conditions and ensured targeted drug release in the intestinal environment.
In vitro dissolution studies demonstrated the successful achievement of delayed and site-specific drug release, while drug release kinetic analysis confirmed a controlled release mechanism suitable for intestinal targeting. Comparative evaluation with the marketed rifaximin formulation indicated comparable pharmaceutical performance and dissolution behaviour.
The stability studies conducted according to ICH guidelines demonstrated that the optimized formulation remained stable under both long-term and accelerated storage conditions without significant changes in physical appearance, drug content, coating efficiency, or dissolution profile.
Overall, the developed enteric-coated rifaximin pellets fulfilled the predetermined Quality Target Product Profile and successfully achieved the intended objective of targeted small intestinal drug delivery. The multiparticulate pellet system offers advantages such as improved gastrointestinal distribution, effective gastric protection, controlled intestinal release, reduced risk of dose dumping, enhanced local therapeutic action, and improved patient compliance.
Therefore, it can be concluded that the developed enteric-coated rifaximin pellet formulation represents a robust, stable, and promising multiparticulate drug delivery system for targeted small intestinal therapy and provides a potential platform for the delivery of other drugs requiring site-specific intestinal release.
REFERENCES

Rutuja Baburao Shinde*, Sachin S. Shinde, Formulation, Development And Evaluation Of Enteric Coating Rifaximin Pellets For Small Intestinal Delivery, Int. J. Sci. R. Tech., 2026, 3 (6), 1751-1768. https://doi.org/10.5281/zenodo.21061102
 10.5281/zenodo.21061102
10.5281/zenodo.21061102