
We use cookies to ensure our website works properly and to personalise your experience. Cookies policy
Desh Bhagat University, Mandi Gobindgarh, Punjab (India)
Recently, sustained and controlled drug delivery has become the demand, and research has been undertaken in achieving much better drug product effectiveness, reliability and safety. The in situ polymeric system has gained much attention, to develop a controlled release system. It has been used as a vehicle for local and systemic drug delivery. Nowadays, it has created much interest, because of its characteristics of high vascularization, high permeability, rapid onset of action, low enzymatic degradation, and avoidance of hepatic first pass metabolism. The main aim of this review is to provide knowledge of different mechanisms of nasal absorption and approaches for nasal drug delivery.
For the past few decades, most of the routine drugs are being administered by parenteral and oral routes (1). Although the oral route is convenient and cheap, sometimes inefficiencies such as low solubility of drug, and the first pass effect (orally absorbed drugs are transported via liver to the general circulation where they metabolized) (2), may cause it to suffer from poor bioavailability (e.g. Griseofulvin) (3). The greater first pass effect of the drug (the rate and extent of the drug reaching systemic circulation), the lower the bioavailability. This route is also not suitable for unconscious patients (4). Therefore, to solve this problem, the parenteral route is proposed, which is accurate, and enables immediate onset of reaction and 100% bioavailability, but it is unacceptable if the drug is proposed for the treatment of chronic disease, because this route also has a risk of embolism and attaining high concentrations, rapidly leading to greater risk of adverse effects. Therefore, a different route is preferred (5). Also, the percutaneous (transdermal) route is used for controlled delivery of drug (stable blood levels) and does not suffer from first pass metabolism, but its use is limited due to low permeability of the skin to many drugs (6). To control these issues, non-parenteral routes, also called transmucosal routes, including the nasal, buccal, pulmonary, rectal and vaginal routes, are used. These routes have few benefits or advantages, such as the possibility of self-administration. The nasal mucosal route of administration achieves faster and higher level of drug absorption. This route has attained great attraction for drug delivery of various drugs. This highlights pathways and mechanisms of therapeutic agents transporting across nasal mucosa and latest developments on novel DDSs using various formulation strategies to improve the intra drug delivery to brain. Colloidal carriers such as various types of nanocarriers (NPs, micelles, nanogels, nano emulsions and liposomes) and microspheres as potential DDSs to brain are main focus of discussion. Patented technology-based drug delivery devices for efficient nasal delivery of drugs are highlighted in this review. Moreover, limitations as well as future prospects of such brain targeted DDSs are also discussed in details. (7)
2) NASAL ANATOMY AND PHYSIOLOGY OF THE NOSE
The human nasal cavity has a total volume of about 16 to 19 mL, and a total surface area of about 180 cm2, and is divided into two nasal cavities via the septum (8). The volume of each cavity is approximately 7.5 mL, having a surface area around 75 cm2 (8-9). Post drug administration into the nasal cavity, a solute can be deposited at one or more of three anatomically distinct regions, the vestibular, the respiratory or the olfactory region.
The vestibular region is located at the opening of nasal passages (9-10), and is responsible for filtering out the air borne particles. It is considered to be the least important of the three regions with regard to drug absorption (11). The respiratory region is the largest having the highest degree of vascularity and is mainly responsible for drug absorption. The olfactory region is of about 10 cm2 in surface area, and it plays a vital role in transportation of drugs to the brain and the CSF. The three distinct anatomical regions present in the nasal cavity and its cross-sectional sketch is shown in (Fig. 1)
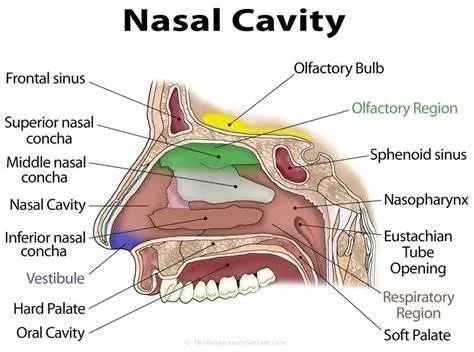
Figure. 1; Anatomy of nose: cross sectional sketch illustrating (A) vestibular, (B) respiratory, and (C) olfactory region.
The epithelium of the nasal passage is covered by a mucus layer, which entraps particles. The mucus layer is cleared from the nasal cavity by cilia, and is renewed every 10 to 15 minutes (12). The pH of the mucosal secretions ranges from 5.5 to 6.5 in adults and 5.0 and 6.7 in children (13) which entraps particles and is cleared from the nasal cavity by cilia. The mucus moves through the nose at an approximate rate of 5 to 6 mm/min. resulting in particle clearance within the nose every 15 to 20 minutes (8, 14). To study nasal drug absorption and the pathways molecules need to penetrate before reaching the brain, it is crucial to get to know its function and the anatomical and cellular structure of the nasal cavity. The nose is responsible for multiple physiological functions such as olfaction and respiration. It is comprised of two symmetric cavities, divided by the septum which lies along the midsagittal plane (15). Researchers became interested in the nasal route for the systemic delivery of medication due to a high degree of vascularization and permeability of the nasal mucosa (16). In humans and other animal species the major functions of the nasal cavity are breathing and olfaction. However, it also affords an important protective activity once it filters, heat and humidity the inhaled air before reaching the lowest airways. Passage of the nasal cavity which runs from nasal vestibule to nasopharynx has a depth of approximately 12-14cm. The total surface area of the nasal cavity in human adult is about 150 cm2 and total volume is about 15 ml (17). Each of two nasal cavities can be subdivided into different regions: nasal vestibule, inferior turbinate, middle turbinate, superior turbinate, olfactory region, frontal sinus, sphenoidal sinus, and cribriform plate of ethmoid bone. The nasal cavity also contains the nasal associated lymphoid tissue (NALT), which is mainly situated in the nasopharynx. Nasal cavity is lined with mucus layer and hairs which are involved in those functions are trapping inhaled particles and pathogens. Moreover, mucociliary clearance, immunological activities and metabolism of endogenous substances are also essential functions of nasal structures (18). The nasal cavity is covered with a mucous membrane which can be divided into two areas; nonolfactory and olfactory epithelium, in this non-olfactory area includes the nasal vestibule which is covered with skin-like stratified squamous epithelium cells, whereas respiratory region, which has a typical airways epithelium covered with numerous microvilli, resulting in a large surface area available for drug absorption and transport (19).
3) MECHANISM OF DRUG ABSORPTION
The first step in the absorption of drug from the nasal cavity is passage through the mucus. Small, uncharged particles easily pass through this layer, though large or charged particles may find it more difficult to cross. The principle of protein in the mucus is mucin, which has the potential to bind to solutes, hindering diffusion (20). Structural changes in the mucus layer are possible as a result of environmental changes (i.e. pH, temperature, etc.) subsequent to a drug's passage through the mucus. Different mechanisms for absorption through mucosa exist (21). They include transcellular (simple diffusion across the membrane) and paracellular transport (movement between cell and transcytosis by vesicle carriers) (figure 2). Drug absorbed can potentially be metabolized before reaching the systemic circulation, and has limited residence time in the cavity (22). Different mechanisms, such as passive diffusion (transcellular), passive diffusion (paracellular), carrier-mediated transport, transcytosis, absorption, and efflux transport have been used for drug transport through the nasal epithelium (23). Table 1 discusses some important comparisons between the two mechanisms, which are widely used in drug transport through the nasal epithelium.
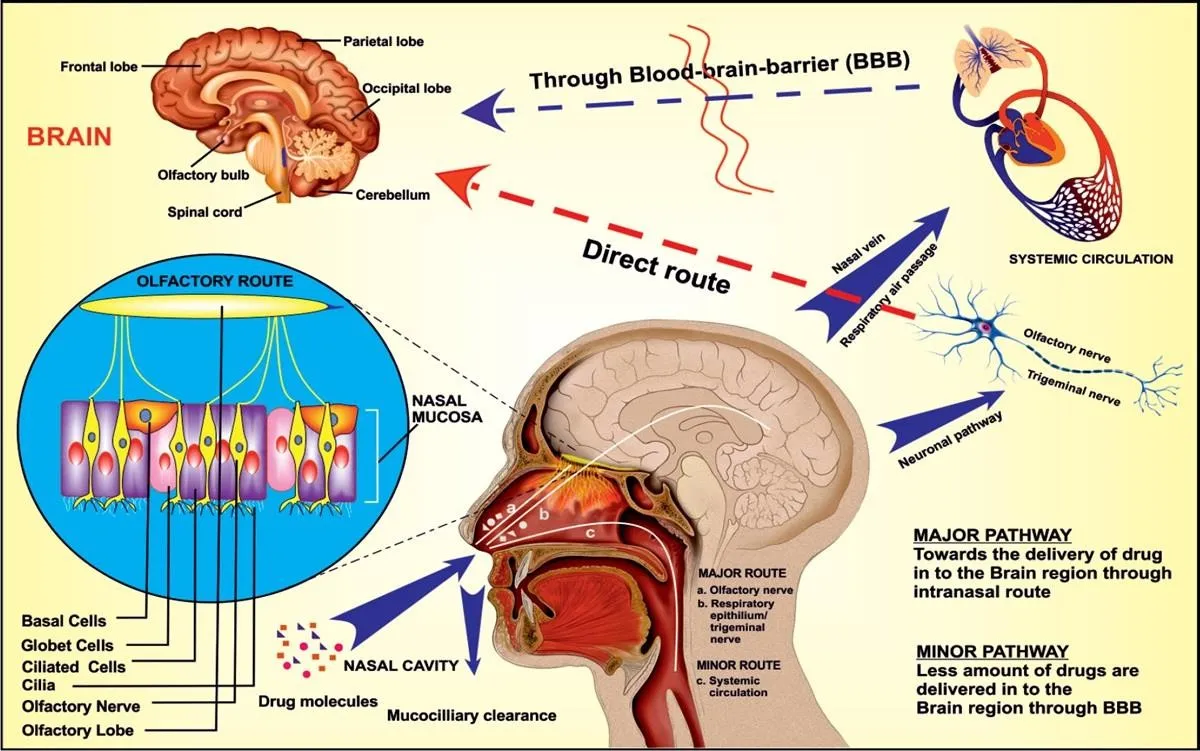
Figure 2: Mechanism of drug absorption.
|
First mechanism (Paracellular process) |
Second mechanism (Transcellular process) |
|
|
Table I. Mechanism of drug passage through the mucus.
Traditionally, the medication for local diseases, such as rhinitis and nasal congestion, has not been administered through the nasal cavity. However, over the last few decades, intranasal (IN) delivery has been gaining much more attention as a promising route of drug administration for systemic therapy (24). Presently, it is being recognized for the delivery of therapeutic compounds including biopharmaceuticals, and for topical nasal treatments such as antihistamines and corticosteroids, and also for systemic delivery of analgesics, sedatives, hormones, vaccines, and cardiovascular drugs by means of the nasal mucosa (25). This is because of the anatomy and physiology of the nasal passage, such as the highly vascularized epithelium, ready accessibility, large surface area, permeable endothelial membrane, high total blood flow, and the prevention of first-pass metabolism (26). IN administration is a “needleless” and non- invasive method of drug delivery through the nose to the brain, and hence an alternative for systemic drug delivery (27). Therapy through IN administration has been an accepted as a form of treatment in the ayurvedic system of Indian medicine, and is called “Nasya Karma”. Drug delivery through the nose is uncomplicated and convenient, and can include the delivery of solutions, suspensions, powders, in situ gel, and ointments (28).
The avoidance of first pass metabolism, quick onset of action, and lowered systemic exposure to drug are the main advantages of IN delivery. Nose-to-brain delivery of drug moieties are possible through the olfactory region, by neuronal and extracellular pathways located at the roof of the nasal cavity, whose neuroepithelium is the only part of the central nervous system (CNS) that is directly exposed to the external environment
(29). The therapeutic agents are carried to the CNS through the olfactory neuroepithelium by the trigeminal nerve systems and olfactory nerve pathways (30). In both intravenous as well as oral administration, the blood-brain barrier (BBB) restricts the brain's access to the drug. However, the intranasal route of delivery can also provide a route of entry to the brain that circumvents the BBB, because the olfactory receptor cells are in direct contact with the CNS (31).
Recently, the nasal mucosa has been examined as a possible route of administration to achieve a faster and higher level of drug absorption (32). The nasal cavity provides a number of distinctive benefits, such as ease of access, good permeability mainly for lipophilic and low molecular weight drugs, low proteolytic activity, prevention of harsh environmental conditions and hepatic first pass metabolism, and potential direct delivery to the brain. Significantly, a number of invasive techniques in drug carrier systems, like the use of nanoparticles, liposomes, nano emulsions, chemical modifications, the prodrug approach, and other invasive strategies like intraparenchymal, intraventricular, and intrathecal delivery are used to increase the CNS-targeting of drugs (33). Large investigative studies have shown that when administered intranasally, vaccines can encourage both local and systemic immune responses. Tables II and III show the advantages and limitations of intranasal delivery along with their respective associated factors.
|
Advantages |
Factors |
|
Improving patient compliance |
Trained person not required Needle-free(painless) Non-invasive User-friendly Self-medication possible |
|
Rapid absorption and onset of pharmacologic action |
|
|
Good penetration |
|
|
Direct delivery of drug to CNS system |
|
|
Avoids harsh environment |
|
Table II. Limitations (associated factors) of intranasal delivery (34)
|
Limitations |
Factors |
|
Reduced capacity of nasal absorption means low bioavailability |
Due to pathologic conditions such as cold or allergies, which may significantly alter the nasal bioavailability |
|
Sometimes, the drugs cause irritation and irreversible damage of the cilia on nasal mucosa |
Due to constituents added in dosage forms |
|
Defense mechanisms such as muco-ciliary clearance influence permeability of drug |
Enzymatic barrier to permeability of drug |
|
Disrupt and dissolve nasal membrane |
Due to high concentration of absorption enhancers |
|
High molecular weight compounds cannot be supplied (mass cut off - 1 kDa) |
Volume of 25–200 l that can be distributed into the nasal cavity is inadequate |
Table III. Limitations (associated factors) of intranasal delivery (29).
Low bioavailability, muco-ciliary clearance, and enzymatic degradation act as major barriers for nasal drug delivery. Some important characteristics of various barriers which mainly affect the nasal drug delivery are discussed below.
Low bioavailability (35)
Polarity lipophilic:
Muco-ciliary clearance (35)
It is an essential factor which involves the combined action of the mucus and cilia, which defend against inhaled foreign particles in the respiratory tract.
Enzymatic degradation (36)
Molecular weight
Scientists concluded that the permeation of drugs less than 300 Da is not significantly influenced by the physicochemical properties of the drug (like molecular weight, size, formulation pH, and p K a of molecule). As molecular weight increases, nasal absorption of drug increases (37).
Chemical form
The chemical form of the drug is an important factor for absorption. Conversion of the drug into a salt or an ester form can change its absorption; for example, in situ absorption of carboxylic acid esters of L-tyrosine was significantly greater than that of unmodified L-Tyrosine (38).
Polymorphism
Polymorphism affects the rate of drug dissolution, solubility, and absorption through biological membranes (39).
Solubility & dissolution rate
Both are important factors in determining nasal absorption of drugs from powders and suspensions. In the nasal cavity, the deposited particles need to be dissolved prior to absorption. No absorption takes place if particles remain in the nasal cavity. The mucosa in nasal cavity is insufficient for dissolution of drug particles, when compared to gastrointestinal fluid available in the case of oral drug delivery (40).
Lipophilicity
On increasing lipophilicity, the permeation of the compound through the nasal mucosa increases because of high lipophilicity, though it has some hydrophilic character. Lipophilic compounds easily cross biological membranes through the transcellular route, since they are fit to partition into the lipid (bilayer) of the cell membrane and diffuse into and traverse the cell in the cell cytoplasm. Systemic bioavailability is decreased due to the hydrophilic nature of many drugs (41).
Partition coefficient and pKa
The pH partition theory states that non ionized species are absorbed well, when compared with ionized species, and hence it is the same in the case of nasal absorption as well.
pH and mucosal irritation
In addition to the properties of the nasal surface, the pH of the formulation can affect a drug's permeation. Both the pH and pKa of drug are considered to rationalize systemic absorption. To avoid nasal irritation, the pH of the nasal formulation should be adjusted to 4.5–6.5. Avoiding irritation results in obtaining efficient drug permeation and prevents the growth of bacteria. Nasal secretions contain lysozyme, which, at acidic pH, destroys certain bacteria. Under alkaline conditions, lysozyme is inactivated and the nasal tissue is susceptible to microbial infection (42).
Osmolarity
Isotonic solutions are administered for shrinkage of the nasal epithelial mucosa, because of the effect of osmolarity on the absorption. This results in increased permeation of the compound because of structural changes. Isotonic solutions also known to inhibit or cease ciliary activity (43).
Viscosity
A higher viscosity of the formulation increases contact time between the drug and the nasal mucosa, thereby increasing permeation time. At the same time, highly viscous formulations interfere with the normal functions like ciliary beating or muco-ciliary clearance, and thus alter the permeability of drugs (44).
Buffer capacity
Nasal formulations are administered in small volumes ranging from 25 to 200 μL. Therefore, nasal secretions may alter the pH of the administrated dose, which can affect the concentration of nonionized drug available for absorption. Hence, an adequate formulation buffer capacity may be required to maintain the pH in situ (45).
Drug concentration, dose, & dose volume
These are three interrelated parameters that impact the performance of the nasal delivery.
Effect of deposition on absorption
Deposition of the formulation in the anterior portion of the nose provides a longer nasal residence time and better absorption, and this is an area of low permeability, whereas in the posterior portion of the nose, where the drug permeability is generally higher, the deposited drug is eliminated by muco-ciliary clearance and therefore has a shorter residence time. (47.).
Nasal blood flow
The nasal mucosal membrane is very rich in vasculature and plays an important role in thermal regulation and humidification of the inhaled air, and therefore the drug absorption will depend upon the vasoconstriction and vasodilatation of the blood vessels (48).
Effect of enzymatic activity
Many enzymes might affect the stability of drugs which are present on the nasal mucosa. For example, proteins and peptides are subjected to degradation by proteases and amino-peptidases at the mucosal membrane (49).
Effect of muco-ciliary clearance
The muco-ciliary clearance is inversely related to the residence time, and therefore inversely proportional to the absorption of drugs administered. It is important to maintain the nasal clearance mechanism to perform normal physiological functions like removal of dirt, allergens, and bacteria (50).
Effect of pathological conditions
Intranasal pathologies such as infections, nasal surgery, cold, and allergic rhinitis may affect the nasal muco-ciliary transport process and/or capacity for nasal absorption. Nasal pathology also alters mucosal pH, and thus affects the absorption of drugs (51).
Permeation enhancers
A variety of permeation enhancers have been investigated to improve the nasal absorption, like fatty acids, bile salts, phospholipids, surfactants, cyclodextrin, etc., which act via different mechanisms such as inhibition of enzyme activity, reduction of mucus viscosity, decreasing muco-ciliary clearance, opening tight junctions, and solubilizing or stabilizing the drug (52).
Prodrug approach
Prodrugs are the inactive chemical moiety which become active at the target site. This approach is mainly used to improve the physicochemical properties such as taste, solubility, and stability of formulation. This approach includes derivatization of C and N termini, esters, and cyclic prodrugs (53).
In situ gel
The conversion into gel by the influence of stimuli including temperature, pH, and ionic concentration, is possible with substances like Carbopol, cellulose derivatives, lecithin, chitosan, etc. (54). These formulations generally control the problems of administration.
Nasal enzyme inhibitors
Enzyme inhibitors like protease and peptidase are used as inhibitors for the formulation of peptide and protein molecules. Other examples are bile salts, amastatin, bestatin, boroleucine, fusidic acids, etc. (55).
Structural modification
Drug structure can be modified without changing the pharmacologic activity, to improve nasal absorption. Chemical modifications are mainly used to modify the physiochemical properties of the drug such that they lead to improved nasal absorption of drug (56).
Mucoadhesion
Mucoadhesion can be defined as the state in which two materials are held together for a long period. Mucoadhesive polymers make intimate contact with the biological membrane, and after the establishment of contact, they penetrate into the tissue surface. Natural polymers can be easily obtained from natural sources, and require an environmentally-friendly method of processing with low cost. Some examples include potato starch, rice starch, maize starch, wheat starch, guar gum, tragacanth, xanthan gum, etc. Synthetic polymers produce environmental pollution during synthesis, and have a high cost of production. These polymers include poly ethylene oxide, poly vinyl alcohol, methyl cellulose, ethyl cellulose, hydroxyl propyl methyl cellulose, etc. (57).
Various nasal formulations such as nasal drops, nasal sprays, nasal gels, nasal powders, nasal inserts, nasal ointments, and so on, are used to deliver the drug into the target site that is brain (figure 3) (58). Among these formulations, in situ gelling systems are widely used for brain targeting.
The physicochemical properties of the drug and its potency are crucial factors when a molecule is formulated in a solution for nasal delivery. In case of small lipophilic molecules, passive diffusion plays an important role in the nose-to-brain delivery as reported by (59). The size of the molecules to be delivered via nose to the brain is also important factor as reported by (60).The absorption of dopamine (Mw 153 Da) was compared to that of the NGF (Mw 27 kDa) by(61). They found that brain concentrations were five-fold higher for the small molecule dopamine than the secreted protein NGF when dosed at the same concentration (62). On the other hand, the larger molecules take longer time to get transported from the nasal cavity to the brain. Following intranasal administration, the brain concentrations were higher in the case of small lipophilic drugs, but they often showed larger improvement in the brain compared to other routes of administration. A hydrophilic small molecule with a log P of 0.98, for brain levels following intranasal and intravenous administration. They showed a fold increase in the area under the curve (AUC) in the brain (depending on the section of the brain) after intranasal administration compared to intravenous route in rats (63). They performed similar experiments with methotrexate, which is also a hydrophilic drug. Here, they found that it provided greater than 13fold higher CSF AUC after nasal administration compared to intravenous administration (64)

Figure 3. Various forms of nasal formulations (58).
In addition to DDSs, another strategy for direct transport of drug from nose to brain is to deposit the drug on olfactory epithelium or region of nose innervated by trigeminal nerves so that more drug is transported to brain via olfactory/trigeminal pathway. For this purpose, many effective and efficient novel nasal drug delivery devices were studied by the researchers and some were patented. Among these devices, pressurized olfactory delivery devices, nebulizers, atomizers, pressurized meter dose inhalers and Breathe Powered Bi-directional nasal devices gained access in the clinical settings Table 4. Nasal drug delivery devices were categorized into three classes, liquid, powder and semisolid formulations containing devices for brain targeted devices (65).
|
Name of product |
Pharmaceutical firm |
Type of delivery device |
Active ingredients |
Disease |
|
Merck's Nasonex® |
Apotex Inc. |
Nasal spray |
Mometasone furoate monohydrate |
Nasal congestion |
|
Advancia® |
Nemera |
Multidose Nasal spray pump |
Corticosteroid |
Allergic rhinitis |
|
Narcan® |
Adapt Pharma |
nasal spray |
Naloxone hydrochloride |
Opoid overdose |
|
Onzetra™ Xsail™ |
Optinose Inc. |
Breath Powered Delivery Device |
Sumatriptan nasal powder |
Migraine |
|
Dymista® |
Meda Pharmaceuticals Inc. |
Nasal spray |
Azelastine hydrochloride/fluticasone propionate |
Seasonal allergic rhinitis |
|
Astelin® |
Meda Pharmaceuticals Inc. |
Nasal spray |
Azelastine hydrochloride |
Seasonal allergic rhinitis |
|
Zomig® |
AstraZeneca Pharamaceuticals |
Nasal spray |
Zolmitriptan |
Acute migraine |
|
Rhinocort® |
McNeil Consumer Healthcare |
Nasal spray |
Budesonide |
Nasal congestion |
|
Triamist® |
Cipla Medpro |
Metered spray |
Triamcinolone acetonide |
Allergic rhinitis |
Table 4; FDA approved products based on nasal drug delivery device.
Powder devices
Powder based formulations are more suitable for IN drug delivery. Powder particles are not easily dissolved in the nasal mucosa and remained in contact with mucosa for long period of time. Powder dosage forms are free from preservatives, enable large doses of drug administration, prevent microbial contamination and improve patient compliance, made them potential candidates for nasal delivery. Powder formulations of macromolecular drugs such as peptide and nonpeptide based drugs have been designed and successfully investigated for nasal delivery. Metered dose insufflators containing mucoadhesive powder polymers delivered polymers in nasal cavity. Polymers formed thick gel on contact with mucosa and decreased mucociliary clearance (66).
Dry powder inhaler
Dry powder inhalers (DPI) enable powdered drug delivery via nasal route. They are single use devices containing drug particles suspended or dissolved in propellant or drug is dissolved when come in contact with nasal mucosa. Very small doses in milligram are delivered to avoid cough associated with large size particles. Unit and multi-dose powder inhalers ensure accurate dosing of drug. Mono-dose inhaler resembles single unit syringe. DPIs are used in asthmatic, bronchitis, COPD patients and also effective in the therapy of diabetes mellitus. Patients hold mouthpiece in the mouth after actuation. Patients inhale deeply and hold breath for 5–10s. Teijin Puvlizer Rhinocort is oldest dry powder inhaler and available in the world market. Rhinocort Turbohaler, Rhinicort Puvlizer and Erizas are three nasal dry powder-based inhalers available for local treatment of rhinitis (67)
Rhinocort use capsule filled device and Erizas use multidose device activated by the patient's breath. Pulvizer works on the airflow generated by the squeeze bottle or patient activated pump. It consists of capsule inserted stem and lower body is soft plastic bulb. Body is pressed to generate air blow, forces the powder particles to expel from capsule into nasal cavity through stem. Eight inhalations are required to empty the capsule (67). DPI should deliver constant amount of drug to the airstream that depends on total contents in container and discharge during exhalation. DPIs are cheap and compatible with MDI. They have commercial access to capsule filing equipments and availability of novel technology to formulate dry powder form of potent drugs. DPIs are not effective for high doses due to cohesive forces between particles. Twin caps are DPI devices suitable for delivering high doses and chronic dosing. It has simple design and automatically operating without medical supervision especially in emergency conditions. It has two capsule shaped cavities filled with dose range from μg to mg.
Nasal powder sprayers
Shin Nippon Biomedical Laboratories designed novel drug delivery technology, System, based on mucoadhesive powder drug carrier. Carrier technology promotes drug absorption and Fit Lizer is nasal device for dry powder formulation delivery. Carriers increase drug absorption, decrease dose requirement and provide quick onset of action. It could be applied for local and systemic delivery, low molecular weight and high molecular weight drugs. It works without absorption enhancers and proven safety in clinical trials. Powder carriers prolong contact time with mucosa and enhance drug absorption (68). Fit-lizer is patient operated device for delivery of dry powder formulations. In multiple-use capsule device, single dose capsule is loaded at each use and alternative to multiple dose capsules of DPI for therapy of chronic diseases. Capsule chamber is pulled to open and filled with Fig. 7. Cross sectional view of human nose with normal dimension during soft palate elevation and bidirectional flow of the air with Bi-Directional device. Reproduced from (69). Pump is squeezed and air blown through capsule delivered the drug. Portable and light weight single use device is effective technology for acute conditions. Tab is pinched and broken. Pump is squeezed to deliver prefilled drug to the nozzle and nasal cavity (70). Bespak developed Unidose resembling Flit Lizer technology. This device comprises sealed container capable of delivering single shot of drug. Unidose device has consistency between doses. Among 95% of the dose delivered to the nasal passage, 60–70% reached to nasal vestibular region limited use of this device for IN brain targeted delivery (71). Upon actuation compressed air in the container forced the pin to rupture the membrane and drug is released. Antibody IgG has been delivered via Unidose device and guided through MRI imaging technique is powder- based delivery device comprises a plunger that exerts pressure on membrane and forces the powdered drug to come out of device into nasal cavity. Vaccines have been delivered through this device (72). Monopowde device designed by the Aptar group worked on the same mechanism of SoluVent. When plunger is pushed, positive pressure is created that ruptured the membrane and drug is emitted. Animal studies using this device were conducted but clinical studies on human are not available.
Instillation and rhinyle Catheter
Catheter delivers drugs to specific region of the nasal cavity. The simplest way of drug delivery to nasal cavity is to insert catheter or squirt tube in nostril and deliver liquid in defined site under visual supervision. This technique is commonly used to anesthetize or sedate the animals. Human mucosa is sensitive to mechanical injury and deposition site and inconsistency in dosing are major concerning issues. One side of the tube is inserted in the nostril and air is blown in the other end through mouth to expel solution filled in the tube to the nostril. Although this technique is valid only for experimental purposes but desmopressin rhinyle catheters are available in some countries for treatment of diabetes inspidus, nocturnal enuresis and Von Willebrand disease (73)
Drops
Drops are being used from decades for nasal drug delivery of liquid formulations. They are cost effective and have easy manufacturing process. Drops have risk of microbial contamination and chemical instability. Mode of administration is important factor to decide fate of formulations in nasal cavity. Previously, glass dropper with elongated neck was used to administer liquid drop formations. Dropper filled with liquid is inserted in nostril and rubber top is pressed to release the drug in nostril. Dropper is feasible for single dose administration and metered-dose spray pumps have taken their place for multidose administration. Spray pumps are expensive and replaced by economical disposable pipette for some clinical conditions. Pipettes are manufactured through “blow-fill-seal” methodology and commonly used for nasal decongestion and irrigation purposes. Fluticasone nasal delivery based on spray pump is ineffective for treatment of nasal polyps. Nasal drops formulations of fluticasone administered through pipette had got place in European market. Nasal drop should deposit drug to the middle meat us, region where polyps emerge (74). Nasal drops delivered through pipette have uncontrollable volume of administration and risk of contamination. Head is downed during drops administration and large volume is rapidly cleared to the laryngopharynx(75). Drops have limitations of discomfort, unacceptable to the patient and cause headache. Squeeze bottle Importance of squeeze bottles is in local nasal drug delivery of topical decongestants.
Pressurized olfactory device (POD)
The olfactory epithelium located between nose and brain accounts for only 3–10% of the surface area of the nasal cavity in human. Its location in the upper part of the nose with turbinate restriction made consistent delivery of therapeutic molecules to this region challenging (76,77). POD has the ability to deposit a majority of drug at olfactory region. These devices contain suitable tank, compressed air or nitrogen, chlorofluorocarbon (CFC) or hydrofluoroalkane (HFA) as propellant and air chamber as shown in Fig. 8. The air chamber is in connection with the device via an internal compartment. Air chamber discharged an aerosol spray into the nasal cavity through an applicator with an orifice. When patient took the dose, the pneumatic solenoid is activated and the compressed air is distributed through tubing to the air chamber and then from chamber into the gas inlet of the housing. Pressurized gas is rotated inside the spin chamber with circumferential helical velocity or vortex-like velocity (78). When the solenoid is triggered, the elongated needle is displaced from the orifice to allow the fluid within the fluid reservoir to escape. Pressurized gas passed through the orifice created partial vacuum to force the fluid out of the reservoir through the orifice (78).
Nebulizers and atomizers
Nebulizers are intended to enable the drug deposition- the upper part of the nose, housing the neural connection between nose and brain. Nebulizers break up liquid solution or suspension into small aerosol droplets with the help of compressed gas or ultrasonic power. Compared to traditional spray pumps, droplets produced from nebulizer, upon nasal inhalation deposited to the upper posterior region of the nasal cavity, thus promoted nose to brain targeting (79,80). Chen et al. explored a novel, hands free nebulizer device for brain tumor targeted delivery. Initial phase I/II clinical trial was conducted on 37 patients of recurrent glioblastoma. Effect of perillyl alcohol (POH) delivered intranasally via nebulizer on recurrent glioblastoma was studied. They used light weight, portable, patients operated and rechargable battery powered device. This study had shown positive clinical effects and improved patient compliance up to 95% (81). Further work reported that long-term IN POH chemotherapy was a safer and effective approach for patients with recurrent glioblastoma. Kurve Technology Inc., (Lynnwood, WA, USA) introduced Via Nasa, a pocketsized advanced electronic atomizer incorporated Controlled Particle Dispersion Technology. This technology has the ability to deliver wide variety of solutions and suspensions with varying surface tension and viscosity. Via Nase targeted the upper part of nose and sinus and thus its potential could be utilized for nose to brain drug delivery (82,83). IN insulin was administered by Via Nase V atomizer for treatment of Alzimers disease and positive outcomes were reported (84). Reduction in pulmonary function was concerning issue, limited the benefits of this technology (85). Wolfe Tory Medical designed "MAD Nasal IN Mucosal Atomization Device". They utilized this novel atomizer to intranasally deliver neuroprotective agents during cryonics to prevent cavity and strictly deposit drug only at olfactory region without systemic exposure. Clinical and preclinical trials of nasal DDSs and devices should be conducted to ensure specificity for brain tissues using novel targeting moieties. Thus, to further explore potential of novel IN DDSs and devices for an efficient and effective delivery of potential drugs to brain more efforts are required. Recently, many drugs have been sucessfully delivered to brain via nasal administration and products based on novel nasal nanoformulations for brain targeting will be available in market. This route is predicted to be utilized not only for therapeutic but also diagnostic purposes. (86.)
Alzheimer disease
Age progression causes irreversible loss of nerve cells in the brain. This may result in difficulty remembering things, with slight confusion, thinking and responding slowly, etc. but severe memory loss, cognition and learning disability, difficulty in speech, abnormal behavior, and disturbing daily activity are the common signs of Alzheimer disease (AD) (87,88). Alzheimer is a progressive, irreversible neurodegenerative disorder that slowly destroys the brain cells responsible for memory, learning, cognition, and other routine activities (89). AD is mostly seen in old age but also sometimes observed in young people, known as the younger stage AD. AD is the most common cause of dementia, around 60%e70% of all cases noticed worldwide. As per the Alzheimer Association Report 2017, around 47 million in the world population were suffering from dementia, of which 37 million were reported to have AD. It is considered the sixth major cause of death in the United States, and the statistics are supposed to reach to 131 million people by 2050 (90). AD was first discovered by the German doctor Alois Alzheimer in 1906, during the treatment of his patent named August D. who was suffering from behavioral abnormalities and memory loss. He observed shrinkage in the brain of the patient in the autopsy. Afterward, in 1910, a psychiatrist Dr. Emil Kraepelin, a colleague of Dr. Alzheimer, named the disease as “Alzheimer’s Disease” to honor his discovery. Then, in 1994, after a very long time, the U.S. Food and Drug Administration (FDA) approved “Cognex” as the first AD drug. From then, until now, we have had only have five FDA-approved drugs, including donepezil, galantamine, tacrine (Cognex), rivastigmine, and memantine. Although, there are various natural and synthetic compounds available that are reported to have a promising anti-AD effect, others are still 2. Common brain disorders 177 under research such as curcumin, quercetin, piperine, S14G-Humanin, nerve growth factor (NGF), insulin, a-mangosteen, tarenflurbil, deferoxamine, risperidone, etc. Based on their mechanism of action, the anti-AD drugs are of two types;
Migraine
Migraine is a headache disorder in which the patient is suffering from recurrent, pulsating, moderate to severe headache starting from either half of the brain, which may migrate to the other half or the whole brain and lasts from 2 h to 3 days. Sometimes it may be associated with vomiting, nausea, and light, sound, or smell sensitivity (91). Moreover, about one-third of migraine patients experience auras, which are visual disturbances that signal the headache. Genetic and environmental factors are believed to be the two major cause of migraine. It is reported that about two-thirds of migraine cases are genetically based. The occurrence of migraine also varies with gender; females are more prone to the disease in comparison to males, and this ratio increases after puberty. The study shows that around 75% of migraine patients are females (92). Migraines have been well known from since early human civilization. In the ancient world (7000 BCE) trepanation (drilling a hole in the skull) was the preferable treatment for migraine. The people at that time believed this procedure let the evil spirits escape from the mind. In the 17th century, William Harvey also recommended trepanation as effective migraine therapy. It was 1868 when a fungus “ergot” was first used in the treatment of migraine. Afterward, in 1918, ergotamine was successfully isolated from ergot and used in the treatment of migraine. Then, in 1959, methysergide was synthesized, and sumatriptan (the first triptan) was developed in 1988 (93). Migraine is generally divided into two types: (1) migraine with aura, and (2) migraine without aura. The pathophysiology of migraine disease is not well known; some researchers believe that the CNS is primarily responsible for the pain, whereas others believe that the peripheral system including sensory neurons and blood vessels play an important role in disease initiation. The primary treatment utilizes regular analgesics like paracetamol, ibuprofen for the headache, and common medicines for nausea. If these are ineffective, the triptans and ergotamines are prescribed. Sometimes, caffeine may also be used for severe pain. Current research on migraine therapy focusses on the use of calcitonin gene related peptides (CGRPs), such as telcagepant and olcegepant, which claim to act on the pathophysiology of the pain. Unfortunately, the phase III clinical trial conducted by Merck on telcagepant failed in 2012 (94).
While current research indicates the existence of an exciting, novel technique for treatment of CNS diseases, more studies must be done –particularly regarding human pharmacokinetics –before therapeutics can be brought to market. As of now, relatively little is known regarding the distribution pattern about the brain, and especially regarding the exchange between CSF and the parenchyma. Since specific drugs will be effective in specific regions due to variable expression of the target receptor, In the last few decades, the attention of various research groups has shifted to the development of novel drug delivery systems to circumvent the BBB. This is due to the significant challenges faced by researchers, academicians and industrialists looking at effective treatment strategies for increasing incidence of brain disorders in the elderly population. Present review embodies the fact that many of the drug delivery systems like polymeric micro- and nanoparticles, nanoemulsions, polymeric micelles, liposomes, etc. are potential carriers for delivery of drugs across the BBB for treatment of CNS disorders. However, there are still a stack of challenges, as most of the potent CNS acting drugs are hydrophilic in nature which makes it difficult for them to cross the BBB. Surface modification of drug delivery carriers serves as one of the promising approaches to circumvent this budding problem. Considering the potential benefits of nasal drug delivery systems (patient compliance and risk--benefit ratio), utilization of this noninvasive method of drug delivery offers a potential alternative to invasive methods and could be exploited, in the near future, for development of novel drug delivery systems. No doubt, this direct nose to brain drug delivery system would have a bright future in the pharmaceutical industry and would definitely bring a large number of commercial products to the pharmaceutical market in near future.
CONCLUSION
There is a long list of drugs that have been developed for various CNS disorders, that have been discarded because they did not pass through the blood-brain barrier. Majority of research and development projects have, therefore, been focusing on the development of new molecules that are able to pass through BBB. Little focus has been on the delivery systems and searching for routes to bypass the BBB. Recently another factor has made this field, “drug delivery to the brain” more complex, is the discovery of efflux mechanisms in the brain and other membranes. Studies have shown that there are many molecules that may have access into the brain, such as imatinib, but are removed from the brain almost immediately. This leaves us with the question: How do we bypass the blood-brain barrier and keep the drug inside brain? In this review the focus is on one delivery route, that has been shown to bypass the BBB and allows a direct access to the brain. The so-called nose-to-brain pathway. It requires that the molecules get absorbed by the nerves inside the nasal cavity, either the olfactory nerves or even the trigeminal nerve. There is a growing demand for new and more potent CNS drugs and with increasing knowledge in the pathways and functions inside the brain, the need for new therapeutics increases as well. One field where there has been an increased demand is within neurodegenerative disorders. Here, the pathogenesis of these diseases is not enough clarified, but also that the drug molecules are not able to reach the target tissue in the brain at an appropriate concentration level. By using intranasal administration, a proper drug concentration in the brain parenchyma may be reached. This show the importance of finding routes that are able to bypass the blood-brain barrier. Numerous research groups have been looking at the absorption of the drugs from the nasal cavity and how they are transported via intercellular (extracellular) or transcellular by endocytosis into the olfactory sensory neurons. After the neuronal uptake, the molecules move away along the axons to the synapse where they are exocytosed onto the olfactory bulb and transported further into the brain via various neuronal pathways. There is also another possibility, since the olfactory mucosa is the only site where the central nervous system is in a direct contact with a mucosal surface. Here, a compound may be absorbed to the lamina propria trough the paracellular space of the olfactory mucosa. From the lamina propria, is transported through the perineural space to the subarachnoid space from where it can reach directly the brain tissue. Besides the direct nose-to-brain pathways, there are other routes for the drugs to penetrate the brain. Namely from the respiratory route they can be transported partially to the circulation and reach the brain by the “nose-to-blood-to-brain” pathway. Today, one of the factors that need to be respected is the role of drug transporters. New drugs must be studied with respect to their ability to be removed by these efflux transporters or if it possible to use specific inhibitors that may improve the therapeutic efficacy and pharmacokinetic profile inside the brain of CNS targeted drugs following intranasal or intraolfactory administration. There are also possibilities to use pharmaceutical and technological approaches to improve the CNS access of the therapeutics, such as formulation factors, additives, nanoformulations, co-administration with vasoconstrictors, lipophilicity and permeability enhancement techniques etc. Taken together, drug research and development in the field of intranasal or intraolfactory administration to the brain is a rapidly growing area. Several potential drugs have been described that require nose-to-brain transport since they do not pass the blood-brain barrier such as oxytocin, IGF-1, insulin, glutathione, and many more. In order to reach the CNS, all these compounds will benefit from intranasal application, compared with the classical delivery routes. As our understanding of the brain, the pathways inside the brain and the pathophysiology of CNS diseases increases, there will be more demands for new therapeutic targets in the brain, where more specific delivery systems will be required. The olfactory route, trigeminal route (and vomeronasal route) may provide direct access to certain regions of the brain, that will otherwise not be reachable. There is still need for optimization of this route(s) as well as full understanding of dosing and safety following nasal drug administration focusing on reaching the neurons for a direct CNS targeted therapy.
This study has been conducted in view of prevalent interest in intranasal mucosal delivery, which provides a needle-free, non- invasive method of targeting the brain by passing the BBB and avoiding hepatic first-pass metabolism in delivering the drug to the brain. This method allows drug direct delivery to the CNS by the olfactory pathway through the mucosa, and provides benefits such as patient compliance and comfort, low exposure, and fewer side effects. It is predictable that intranasal formulations will go on to achieve market potential. The nasal mucosa offers controlled-release drug delivery, but due to certain limitations, the use of the intranasal route for administration of drugs is limited. To decrease these limitations, the mucoadhesive polymeric system is used. The first requirement for controlled drug delivery is to focus on patient comfort, which is offered here by the in- situ gelling system. In situ gels also offer a number of other advantages, such as prolonged or sustained release of drug. For the past few decades, extraordinary and novel research on pH-induced, temperature-sensitive, and ion-induced gel-forming formulations have been described in literature.
REFERENCES


Faisal Ahmad Bhat*, Mohita Thakur, Intranasal Drug Delivery System: A Noval Approach For Brain Targetting, Int. J. Sci. R. Tech., 2026, 3 (7), 35-53. https://doi.org/10.5281/zenodo.21131270
 10.5281/zenodo.21131270
10.5281/zenodo.21131270