
We use cookies to ensure our website works properly and to personalise your experience. Cookies policy
Department of Pharmacognosy And Phytochemistry, K. V. N. Naik S. P. Sanstha’s, Institute of Pharmaceutical Education & Research, Canada Corner, Nashik, 422002, Maharashtra, India.
Phytopharmaceuticals are medicinal products derived from plant sources and developed according to defined standards of quality, safety, and efficacy. Globally, these products occupy a complex regulatory position between conventional pharmaceuticals and traditional herbal medicines. Growing public demand for plant-based therapies, together with increasing scientific interest in natural products, has highlighted the need for robust and harmonised regulatory systems. This review critically compares the regulatory frameworks governing phytopharmaceuticals in India, the United States (US), the European Union (EU), China, and Japan. It analyses the legislative basis, regulatory authorities, approval pathways, and documentation requirements for quality, safety, and efficacy in each jurisdiction. India introduced a dedicated phytopharmaceutical category under the Drugs and Cosmetics Rules in 2015, creating a pathway intended to combine traditional knowledge with pharmaceutical standards. The US Food and Drug Administration regulates botanical drugs through its Botanical Drug Development Guidance, which applies pharmaceutical-level evidence requirements while recognising the challenges of multi-constituent products. The EU operates a structured Traditional Herbal Medicinal Products Directive (THMPD), allowing simplified registration for products with established traditional use. China regulates phytopharmaceuticals primarily through the Traditional Chinese Medicine (TCM) framework under the National Medical Products Administration (NMPA), while Japan relies on the highly standardised Kampo medicine system under the Ministry of Health, Labour and Welfare (MHLW). Although these systems differ considerably, all jurisdictions face common challenges, including variability of botanical raw materials, quality standardisation, herb-drug interactions, insufficient pharmacovigilance, and balancing traditional knowledge with evidence-based medicine. Regulatory convergence remains limited because of differing cultural, historical, and scientific approaches to traditional medicine. The review concludes that future progress requires harmonised quality standards, improved analytical technologies, stronger pharmacovigilance systems, and evidence models better suited to multi-component botanical medicines.
Medicinal plants have been used for centuries in traditional healthcare systems across the world. In recent decades, however, increasing attention has been directed toward evaluating these products using modern scientific and regulatory standards. Phytopharmaceuticals differ from traditional herbal remedies because they are expected to demonstrate consistent quality, safety, and therapeutic value through defined manufacturing and evaluation processes.
Regulating phytopharmaceuticals is challenging because botanical medicines are chemically complex. Unlike conventional pharmaceuticals that generally contain a single active molecule, botanical products contain multiple constituents acting through several mechanisms simultaneously. This complexity complicates quality control, safety assessment, and efficacy evaluation.
Global use of herbal medicines remains extremely high. According to the World Health Organization (WHO), nearly 80% of the global population relies on traditional or herbal medicine for some aspect of primary healthcare [1]. The global herbal medicine market has expanded rapidly, driven by public interest in natural therapies, rising healthcare costs, and dissatisfaction with some conventional medicines [2]. However, increasing commercialisation has also raised concerns regarding adulteration, contamination, misleading claims, and herb-drug interactions [3,4].
Several plant-derived medicines have achieved acceptance within mainstream medicine. Artemisinin from Artemisia annua revolutionised malaria treatment, while paclitaxel from Taxus brevifolia remains a major anticancer drug [5]. Other botanicals, such as Hypericum perforatum (St John’s Wort) and Withania somnifera (Ashwagandha), have generated growing scientific evidence for therapeutic benefits [6,7]. These examples demonstrate the importance of developing regulatory systems capable of supporting both innovation and public safety.
Different jurisdictions have adopted distinct regulatory approaches. India created a specific phytopharmaceutical category within pharmaceutical legislation. The US regulates botanical drugs through conventional pharmaceutical pathways with special guidance. The EU uses a structured traditional-use registration system. China integrates TCM into national healthcare policy, while Japan regulates Kampo medicines through pharmacopoeial standardisation. Understanding these systems is important for researchers, manufacturers, clinicians, and policymakers involved in botanical medicine development.
2. AIM AND OBJECTIVES
The aim of this review is to compare the regulatory frameworks governing phytopharmaceuticals in India, the United States, the European Union, China, and Japan.
The objectives are:
3.OVERVIEW OF PHYTOPHARMACEUTICALS
Phytopharmaceuticals occupy a unique position between conventional pharmaceuticals and traditional herbal preparations. Unlike crude herbal remedies used historically in traditional systems of medicine, phytopharmaceuticals are expected to meet scientifically established standards for quality, safety, efficacy, and manufacturing consistency. Regulatory agencies increasingly recognise that plant-derived products cannot simply be treated as dietary supplements when therapeutic claims are made.
The scientific interest in phytopharmaceuticals has grown considerably due to advances in natural product chemistry, pharmacognosy, molecular biology, and analytical technology. Several modern drugs, including anticancer and antimalarial agents, originated from medicinal plants. Consequently, there is renewed global interest in exploring botanical products as sources of new therapeutic agents and adjunct therapies.
At the same time, increasing commercialisation of herbal medicines has intensified concerns regarding product quality, contamination, misleading advertising, and irrational use. Variability in cultivation conditions, harvesting procedures, and extraction methods may significantly influence therapeutic outcomes. Therefore, regulatory oversight has become essential for ensuring reproducibility and patient safety.
Different jurisdictions interpret the term phytopharmaceutical differently depending on historical and legal context. Some countries emphasise pharmaceutical evidence and clinical trials, while others place greater weight on traditional use documentation and pharmacopoeial standardisation. These differences strongly influence global trade, research investment, and patient access to botanical medicines.
3.1 Definition and Scope
The term “phytopharmaceutical” is interpreted differently across jurisdictions. In India, it refers to purified and standardised plant-derived products with proven therapeutic value regulated under pharmaceutical law [8]. The EU uses the broader term “herbal medicinal products”, while the US FDA defines botanical drug products as medicines containing plant materials as active ingredients [9].
Phytopharmaceuticals are distinct from crude herbal preparations because they require standardisation and controlled manufacturing processes. Products may include extracts, fractions, or purified mixtures standardised using marker compounds or active constituents.
3.2 Pharmacological Characteristics
The pharmacology of botanical products differs substantially from that of conventional drugs. Instead of acting through a single active ingredient, phytopharmaceuticals often contain numerous compounds acting synergistically or additively [10]. This multi-target activity may provide therapeutic advantages but complicates mechanistic and regulatory evaluation.
For example, many botanical extracts exhibit antioxidant, anti-inflammatory, immunomodulatory, and antimicrobial activities simultaneously. These combined effects may contribute to therapeutic benefit in chronic diseases where multiple pathological pathways are involved. However, identifying the precise contribution of each constituent remains scientifically difficult.
Another challenge is reproducibility. The concentration of phytochemicals within medicinal plants may vary considerably depending on environmental conditions and processing methods. Even when the same plant species is used, differences in cultivation location, climate, harvesting season, storage, and extraction procedures can significantly alter the chemical profile of the final product.
Quality control also presents difficulties. Standardisation frequently relies on marker compounds selected for analytical convenience rather than confirmed therapeutic relevance [11]. Environmental factors such as climate, soil composition, harvesting season, and extraction conditions can significantly influence phytochemical composition [12]. Consequently, Good Agricultural and Collection Practices (GACP) are essential components of phytopharmaceutical quality assurance.
In recent years, advanced analytical techniques such as high-performance liquid chromatography (HPLC), ultra-performance liquid chromatography (UPLC), and mass spectrometry-based metabolomics have improved the ability to characterise botanical preparations more comprehensively. These technologies may eventually support more sophisticated regulatory standards.
The pharmacology of botanical products differs substantially from that of conventional drugs. Instead of acting through a single active ingredient, phytopharmaceuticals often contain numerous compounds acting synergistically or additively [10]. This multi-target activity may provide therapeutic advantages but complicates mechanistic and regulatory evaluation.
Quality control also presents difficulties. Standardisation frequently relies on marker compounds selected for analytical convenience rather than confirmed therapeutic relevance [11]. Environmental factors such as climate, soil composition, harvesting season, and extraction conditions can significantly influence phytochemical composition [12]. Consequently, Good Agricultural and Collection Practices (GACP) are essential components of phytopharmaceutical quality assurance.
|
Jurisdiction |
Regulatory Authority |
Legal Framework |
Product Classification |
Basis for Approval |
|
India |
Central Drugs Standard Control Organisation (CDSCO) / Drugs Controller General of India (DCGI) |
Drugs and Cosmetics Act 1940 and Drugs and Cosmetics (Amendment) Rules 2015 |
Phytopharmaceutical Drug |
Scientific evidence supported by traditional use |
|
United States |
Food and Drug Administration (FDA) / Center for Drug Evaluation and Research (CDER) |
Federal Food, Drug, and Cosmetic Act (FD&C Act) and DSHEA 1994 |
Botanical Drug |
Full pharmaceutical-level clinical evidence |
|
European Union |
European Medicines Agency (EMA) / Committee on Herbal Medicinal Products (HMPC) |
Directive 2004/24/EC (THMPD) |
Herbal Medicinal Product |
Traditional use with quality and safety evidence |
|
China |
National Medical Products Administration (NMPA) |
Traditional Chinese Medicine Law 2017 and Drug Administration Law |
Traditional Chinese Medicine (TCM) Products |
Traditional evidence and/or clinical evaluation |
|
Japan |
Ministry of Health, Labour and Welfare (MHLW) / Pharmaceuticals and Medical Devices Agency (PMDA) |
Pharmaceutical and Medical Devices Act |
Kampo Medicines |
Pharmacopoeial standardisation and historical use |
Table 1. Global Regulatory Overview of Phytopharmaceuticals
4. REGULATORY FRAMEWORK IN INDIA
4.1 Legislative Basis
India introduced a formal phytopharmaceutical category through the Drugs and Cosmetics (Amendment) Rules 2015 under the Drugs and Cosmetics Act, 1940 [13]. These rules established phytopharmaceuticals as scientifically evaluated plant-derived medicines distinct from traditional AYUSH preparations.
The framework was intended to encourage evidence-based development of botanical medicines while leveraging India’s extensive traditional medicine knowledge and biodiversity resources.
4.2 Regulatory Authority
The Central Drugs Standard Control Organisation (CDSCO), headed by the Drugs Controller General of India (DCGI), regulates phytopharmaceuticals. Approval is mandatory before manufacturing or marketing.
The New Drugs and Clinical Trials Rules 2019 further clarified requirements for clinical trials, safety studies, and post-marketing surveillance [14].
4.3 Approval Pathway
Indian regulations define phytopharmaceuticals as purified and standardised products derived from medicinal plants with demonstrated therapeutic value. The approval process requires submission of a dossier containing:
Traditional use evidence may reduce clinical trial requirements. Products with extensive historical use and published literature may receive waivers for early-phase studies, while novel products generally require full Phase I–III evaluation [15].
4.4 Documentation Requirements
The Chemistry, Manufacturing and Controls (CMC) section must include botanical identification, herbarium voucher specimens, validated analytical methods, and GACP documentation. Stability testing is expected according to ICH guidelines.
Manufacturers must also demonstrate consistency in extraction procedures, solvent systems, marker compound quantification, and finished product specifications. The use of authenticated plant material is particularly important because substitution and adulteration remain common problems in herbal product supply chains.
Safety assessment includes acute and sub-chronic toxicity, genotoxicity, and reproductive toxicity studies where applicable. Efficacy evidence may combine published data, traditional use records, and clinical trials conducted at approved institutions.
Although the Indian framework is progressive, implementation challenges remain. Industry stakeholders have frequently reported delays in approvals, lack of detailed technical guidance, and inconsistencies in interpretation by regulatory reviewers. Nevertheless, the 2015 amendments represented a major shift toward evidence-based regulation of botanical medicines in India.
Post-marketing requirements include adverse event reporting and periodic safety update reports (PSURs).
The Chemistry, Manufacturing and Controls (CMC) section must include botanical identification, herbarium voucher specimens, validated analytical methods, and GACP documentation. Stability testing is expected according to ICH guidelines [16].
Safety assessment includes acute and sub-chronic toxicity, genotoxicity, and reproductive toxicity studies where applicable. Efficacy evidence may combine published data, traditional use records, and clinical trials conducted at approved institutions.
Post-marketing requirements include adverse event reporting and periodic safety update reports (PSURs).
5. REGULATORY FRAMEWORK IN THE UNITED STATES
The United States has one of the most scientifically demanding regulatory systems for botanical products intended for therapeutic use. However, the coexistence of dietary supplement and pharmaceutical pathways has created a fragmented market in which many botanical products are sold with limited oversight while avoiding pharmaceutical approval requirements.
This dual structure has significantly influenced the development of the US herbal medicine industry. Most manufacturers prefer marketing botanical products as dietary supplements because pharmaceutical approval requires extensive investment in clinical trials and manufacturing standardisation. As a result, relatively few botanical products have pursued formal drug approval despite widespread public use.
5.1 Legislative Basis
In the US, botanical products may be regulated either as dietary supplements under the Dietary Supplement Health and Education Act (DSHEA) 1994 or as drugs under the Federal Food, Drug, and Cosmetic Act (FD&C Act) [17].
This distinction is highly significant. Dietary supplements require limited pre-market oversight, whereas botanical drugs must satisfy pharmaceutical-level evidence standards.
5.2 FDA Botanical Drug Guidance
The FDA issued Botanical Drug Development Guidance in 2004 and updated it in 2016 [18]. The guidance recognises the complexity of botanical products and allows flexibility regarding complete chemical characterisation.
Botanical drug applications are reviewed by the Center for Drug Evaluation and Research (CDER).
5.3 Approval Pathways
Botanical drugs may follow:
The FDA generally requires clinical trial evidence for efficacy. Traditional use alone is not accepted as proof of therapeutic effectiveness.
Only a few botanical drugs have obtained FDA approval, including Veregen (sinecatechins) and Fulyzaq (crofelemer) [19]. The small number reflects the high cost and evidentiary burden associated with pharmaceutical approval.
5.4 Documentation Requirements
CMC documentation must include species authentication, manufacturing consistency, analytical fingerprinting, contaminant testing, and validated methods for identifying active or marker compounds [20].
The FDA encourages applicants to use advanced analytical techniques capable of demonstrating batch-to-batch consistency even when complete chemical characterisation is not possible. Fingerprint chromatographic methods and bioassays are commonly used to establish product identity and reproducibility.
Safety requirements include toxicology studies, genotoxicity assessment, and safety pharmacology evaluation. Existing human use data may reduce early-stage study requirements.
Clinical efficacy must be demonstrated through well-controlled trials following international standards. The FDA maintains that historical use alone cannot establish efficacy because traditional experience lacks the controls necessary to exclude placebo effects and bias.
Although scientifically rigorous, this requirement has been criticised for making pharmaceutical development of botanical medicines financially difficult. Consequently, most herbal products in the United States continue to be marketed as dietary supplements rather than approved drugs.
Approved botanical drugs are subject to standard pharmacovigilance and adverse event reporting requirements.
CMC documentation must include species authentication, manufacturing consistency, analytical fingerprinting, contaminant testing, and validated methods for identifying active or marker compounds [20].
Safety requirements include toxicology studies, genotoxicity assessment, and safety pharmacology evaluation. Existing human use data may reduce early-stage study requirements.
Clinical efficacy must be demonstrated through well-controlled trials following international standards. Approved botanical drugs are subject to standard pharmacovigilance and adverse event reporting requirements.
6. REGULATORY FRAMEWORK IN THE EUROPEAN UNION
6.1 Legislative Foundation
The EU regulates herbal medicines through Directive 2004/24/EC, which established the Traditional Herbal Medicinal Products Directive (THMPD) [21]. The directive introduced a simplified Traditional Herbal Registration (THR) pathway.
Products may qualify for simplified registration if they demonstrate at least 30 years of traditional medicinal use, including 15 years within the EU.
6.2 EMA and HMPC
The European Medicines Agency (EMA) hosts the Committee on Herbal Medicinal Products (HMPC), which develops Community herbal monographs summarising quality, safety, and traditional use information [22].
These monographs reduce documentation requirements for applicants and support harmonisation across EU member states.
6.3 Approval Pathways
The EU offers three main pathways:
The THR pathway does not require clinical proof of efficacy. Instead, efficacy is considered plausible based on long-standing traditional use combined with available pharmacological evidence [23].
6.4 Documentation Requirements
Quality requirements include compliance with European Pharmacopoeia monographs, validated extraction methods, and contaminant limits [24].
The European system places strong emphasis on quality consistency and pharmacopoeial standardisation. Manufacturers are expected to define extraction ratios, manufacturing processes, and marker compound specifications in detail. This contributes to comparatively high confidence in product quality within the EU market.
Safety assessment relies largely on traditional use history supplemented by toxicological data. Pharmacovigilance obligations are similar to those applied to conventional medicines.
The THR pathway is especially suitable for products intended for self-medication of minor conditions. Products approved under this pathway are generally limited to indications not requiring medical supervision.
One major criticism of the EU system is that the 15-year EU use requirement disadvantages non-European herbal traditions such as Ayurveda and TCM [25].
Quality requirements include compliance with European Pharmacopoeia monographs, validated extraction methods, and contaminant limits [24].
Safety assessment relies largely on traditional use history supplemented by toxicological data. Pharmacovigilance obligations are similar to those applied to conventional medicines.
One major criticism of the EU system is that the 15-year EU use requirement disadvantages non-European herbal traditions such as Ayurveda and TCM [25].
7. REGULATORY FRAMEWORK IN CHINA
7.1 Legislative Context
China integrates Traditional Chinese Medicine directly into its healthcare system. The Traditional Chinese Medicine Law (2017) and Drug Administration Law provide the main legislative framework [26].
The National Medical Products Administration (NMPA) regulates TCM products.
7.2 Classification of TCM Products
TCM products are classified into several categories, including:
Classical TCM prescriptions documented in historical texts may qualify for simplified approval without full clinical trials [27].
7.3 Approval Process
Innovative TCM drugs require pharmaceutical-quality evidence, including:
China generally requires domestic clinical data, limiting reliance on foreign studies [28]. This requirement is intended to ensure that safety and efficacy are evaluated within the Chinese population and healthcare system. However, it also creates significant barriers for international manufacturers seeking market entry.
The classical prescription pathway represents one of the most distinctive features of the Chinese regulatory system. Preparations documented in recognised classical texts may qualify for simplified approval if they match traditional formulations and manufacturing standards. In such cases, historical evidence and established clinical use may substitute for extensive modern clinical trials.
Supporters argue that centuries of documented medical use provide meaningful evidence regarding safety and therapeutic value. Critics, however, contend that historical records cannot replace modern controlled clinical research. This debate reflects broader disagreements about the role of traditional knowledge in evidence-based medicine.
Innovative TCM drugs require pharmaceutical-quality evidence, including:
China generally requires domestic clinical data, limiting reliance on foreign studies [28].
7.4 Documentation Requirements
Applications must comply with standards in the Chinese Pharmacopoeia, which contains extensive TCM monographs [29].
Quality requirements include identity testing, contaminant limits, chromatographic fingerprinting, and validated analytical methods.
Safety requirements vary depending on historical use. Classical formulations may rely partly on historical safety data, whereas innovative products require full toxicological evaluation.
China has strengthened post-marketing surveillance following safety concerns involving aristolochic acid nephropathy and other adverse reactions associated with traditional medicines [30].
8. REGULATORY FRAMEWORK IN JAPAN
8.1 Historical Context
Japan regulates traditional herbal medicines primarily through the Kampo system. Kampo medicines are integrated into mainstream healthcare and prescribed by physicians under the national health insurance system [31].
The Pharmaceutical and Medical Devices Act forms the legislative basis for regulation.
8.2 Approved Kampo Formulae
Japan maintains a list of approved Kampo formulae regulated under pharmacopoeial standards. Manufacturers of approved formulations do not require full new drug approval if they comply with established quality specifications [32].
However, novel botanical products outside the approved list must undergo the full pharmaceutical approval process.
8.3 Quality Standards
The Japanese Pharmacopoeia includes detailed monographs for crude drugs and Kampo preparations [33].
Japan applies stringent quality standards, including:
These standards contribute to the strong quality reputation of Japanese Kampo products.
Unlike some other systems, the Japanese framework places particularly strong emphasis on reproducible manufacturing methods. Approved Kampo formulations are produced according to tightly defined specifications regarding extraction procedures, ingredient ratios, and dosage forms.
This high level of standardisation helps minimise batch variability and supports clinician confidence in Kampo prescribing. However, some researchers argue that the rigid regulatory structure may limit innovation by discouraging the development of modified or novel formulations.
The Japanese Pharmacopoeia includes detailed monographs for crude drugs and Kampo preparations [33].
Japan applies stringent quality standards, including:
These standards contribute to the strong quality reputation of Japanese Kampo products.
8.4 Safety and Pharmacovigilance
Adverse event reporting for Kampo medicines follows the same system used for conventional pharmaceuticals. The Pharmaceuticals and Medical Devices Agency (PMDA) actively monitor safety signals and updates product labelling when necessary [34].
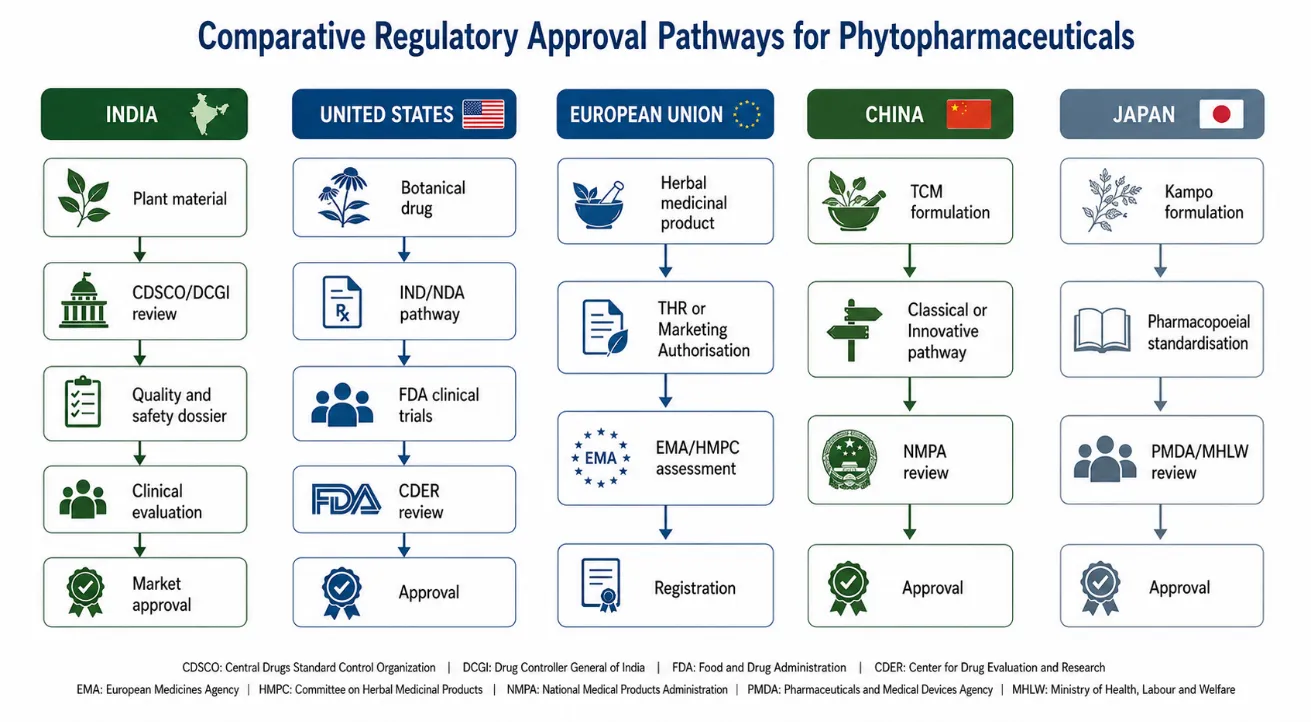
Figure 1. Comparative Regulatory Approval Pathways
9. COMPARATIVE ANALYSIS
The regulatory systems examined in this review demonstrate how historical, cultural, and scientific perspectives shape national approaches to phytopharmaceutical regulation. Although all jurisdictions recognise the importance of ensuring product quality and patient safety, the methods used to achieve these objectives differ substantially.
Countries with strong traditional medicine systems, such as China and Japan, integrate botanical medicines directly into healthcare infrastructure. In contrast, the United States treats botanical drugs primarily through pharmaceutical legislation. India and the European Union occupy intermediate positions by attempting to balance traditional use with modern scientific evaluation.
These differences have important consequences for research investment, market access, product innovation, and international trade. Manufacturers seeking global approval often face the challenge of preparing different evidence packages for different regulatory authorities, increasing development costs and delaying international availability.
9.1 Structural Differences
The five jurisdictions differ substantially in how phytopharmaceuticals are classified and evaluated.
The US framework imposes the strictest efficacy standards because clinical evidence is mandatory for drug approval. In contrast, the EU and China provide greater accommodation for traditional use evidence.
9.2 Quality Standards
Quality control requirements show the greatest convergence internationally. All jurisdictions require:
However, pharmacopoeial coverage differs considerably. The European Pharmacopoeia focuses mainly on European botanicals, while the Chinese Pharmacopoeia extensively covers TCM materials [35]. Japan applies particularly rigorous standardisation through fixed extract ratios and tightly controlled manufacturing practices.
India increasingly emphasises GACP and authenticated raw materials, whereas the FDA relies heavily on analytical fingerprinting and manufacturing consistency. Despite these differences, all systems recognise that botanical quality assurance must address contamination, adulteration, and variability.
The growing adoption of chromatographic fingerprinting and molecular authentication methods represents a major advance in regulatory science. Such technologies improve the ability to distinguish authentic medicinal plants from substitutes or adulterants and may eventually become standard international requirements.
Quality control requirements show the greatest convergence internationally. All jurisdictions require:
However, pharmacopoeial coverage differs considerably. The European Pharmacopoeia focuses mainly on European botanicals, while the Chinese Pharmacopoeia extensively covers TCM materials [35]. Japan applies particularly rigorous standardisation through fixed extract ratios and tightly controlled manufacturing practices.
|
Documentation Component |
India |
United States |
European Union |
China |
Japan |
|
Botanical Authentication |
Required |
Required |
Required |
Required |
Required |
|
Herbarium Voucher Specimen |
Required |
Recommended |
Recommended |
Required |
Required |
|
Manufacturing Information |
Required |
Required |
Required |
Required |
Required |
|
Stability Studies |
ICH guidelines |
FDA requirements |
EMA guidelines |
NMPA guidelines |
PMDA guidelines |
|
Toxicity Studies |
Acute and sub-chronic toxicity |
Full toxicology package |
Traditional safety + toxicology |
Depends on category |
Safety evaluation required |
|
Clinical Evidence |
Traditional + clinical data |
Mandatory clinical trials |
Traditional use evidence acceptable |
Varies by product |
Required for new products |
|
Chromatographic Fingerprinting |
Recommended |
Strongly recommended |
Required |
Required |
Required |
|
Contaminant Testing |
Required |
Required |
Required |
Required |
Required |
|
Post-Marketing Surveillance |
PSURs and ADR reporting |
Mandatory |
Mandatory |
Strengthening |
Strong pharmacovigilance |
Table 2. Documentation Requirements for Phytopharmaceutical Approval
9.3 Efficacy Standards
Efficacy assessment remains the major area of divergence.
These differences reflect contrasting views regarding the evidentiary value of traditional medical knowledge.
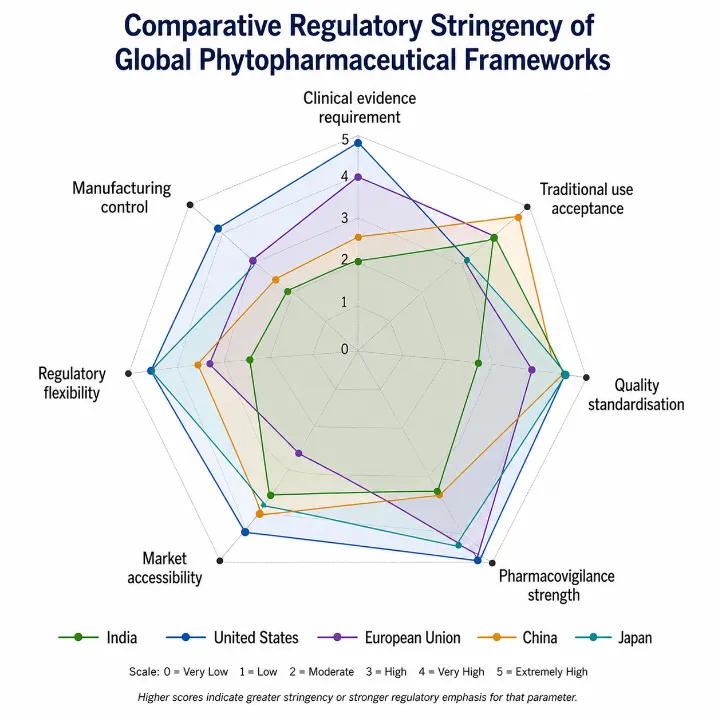
Figure 2. Global Comparison of Regulatory Stringency
10. CHALLENGES AND LIMITATIONS
10.1 Variability of Raw Materials
Biological variability is one of the greatest challenges in phytopharmaceutical regulation. Environmental conditions, cultivation methods, and processing techniques significantly influence phytochemical composition [36].
Medicinal plants are biological materials rather than chemically uniform substances. Consequently, variations in rainfall, temperature, soil nutrients, and agricultural practices can alter the concentration of active constituents considerably.
Although GACP and GMP improve consistency, complete standardisation remains difficult.
This variability complicates the establishment of universal quality standards. Two products derived from the same species may differ substantially in chemical composition and therapeutic activity if cultivation and extraction conditions are not carefully controlled. Therefore, regulators increasingly require detailed documentation of sourcing and manufacturing procedures.
Biological variability is one of the greatest challenges in phytopharmaceutical regulation. Environmental conditions, cultivation methods, and processing techniques significantly influence phytochemical composition [36].
Although GACP and GMP improve consistency, complete standardisation remains difficult.
10.2 Authentication and Adulteration
Adulteration and species substitution continue to threaten product quality and safety. DNA barcoding and molecular identification techniques have improved authentication capabilities, but these technologies are not yet uniformly required [37].
Studies continue to identify undeclared species and contaminants in commercial herbal products [38].
10.3 Herb-Drug Interactions
Herb-drug interactions represent a major safety concern. St John’s Wort is a well-known example because it induces CYP3A4 and can reduce the effectiveness of several conventional drugs [39].
The EU has developed specific guidance on herb-drug interaction studies, whereas other jurisdictions remain less comprehensive in this area.
10.4 Protection of Traditional Knowledge
The commercial development of traditional medicines raises concerns regarding intellectual property and benefit-sharing. India’s Traditional Knowledge Digital Library (TKDL) was created to prevent inappropriate patenting of traditional formulations [40].
However, international regulatory systems still lack effective integration with access and benefit-sharing frameworks such as the Nagoya Protocol.
10.5 Pharmacovigilance Limitations
Pharmacovigilance for botanical medicines remains underdeveloped globally. Underreporting of adverse events, widespread self-medication, and difficulties in causality assessment reduce surveillance effectiveness [41].
Many consumers incorrectly assume that natural products are inherently safe. Consequently, adverse reactions may go unrecognised or unreported. In addition, herbal products are frequently used alongside prescription medicines, making causality assessment more difficult.
Healthcare professionals may also lack sufficient training in herbal pharmacology and herb-drug interactions, reducing the likelihood of accurate reporting and counselling. Strengthening education and integrating phytopharmaceutical monitoring into mainstream healthcare systems are therefore important future priorities.
Historical examples, including aristolochic acid nephropathy, demonstrate the importance of stronger monitoring systems [42].
Pharmacovigilance for botanical medicines remains underdeveloped globally. Underreporting of adverse events, widespread self-medication, and difficulties in causality assessment reduce surveillance effectiveness [41].
Historical examples, including aristolochic acid nephropathy, demonstrate the importance of stronger monitoring systems [42].
11. FUTURE PERSPECTIVES
Future regulation of phytopharmaceuticals will likely be influenced by advances in analytical chemistry, biotechnology, pharmacogenomics, and digital health systems. These developments may help overcome several longstanding challenges associated with botanical product standardisation and evaluation.
Modern analytical tools such as high-resolution mass spectrometry, metabolomics, and chromatographic fingerprinting are improving the ability to characterise complex plant extracts comprehensively. These technologies can support better quality assurance and batch consistency evaluation.
Network pharmacology and systems biology approaches may also improve understanding of multi-component botanical medicines. Unlike conventional reductionist drug discovery models, these approaches recognise that phytopharmaceuticals frequently act through multiple pathways simultaneously.
Advances in analytical chemistry, metabolomics, and bioinformatics are likely to transform phytopharmaceutical regulation.
High-resolution metabolomic profiling can generate comprehensive chemical fingerprints, improving batch consistency assessment and quality control [43]. Network pharmacology may also provide better scientific models for understanding the multi-component activity of botanical medicines [44].
International harmonisation remains limited but increasingly necessary. WHO initiatives and future collaboration between regulatory agencies may support development of globally accepted standards for botanical products [45].
Digital health technologies could also improve pharmacovigilance through mobile reporting systems and real-world safety monitoring.
The COVID-19 pandemic highlighted both the therapeutic potential and regulatory challenges of traditional medicines during public health emergencies. Future frameworks must support rapid evidence generation while maintaining safety and quality standards [46].
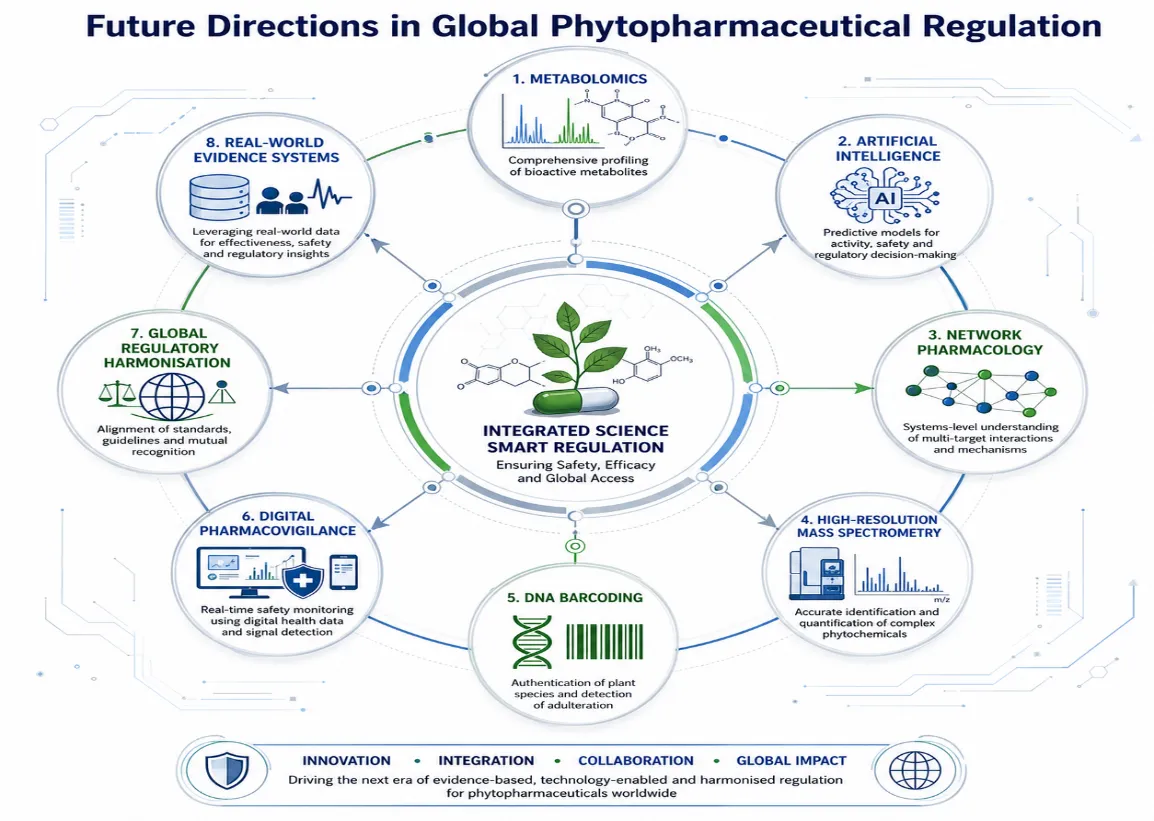
Figure 3. Future Trends in Phytopharmaceutical Regulation
CONCLUSION
The regulatory frameworks governing phytopharmaceuticals in India, the United States, the European Union, China, and Japan differ considerably in their treatment of traditional knowledge, clinical evidence, and quality requirements.
The US system prioritises rigorous clinical evidence but creates major commercial barriers. The EU provides a pragmatic traditional-use pathway but disadvantages non-European medicines. India’s phytopharmaceutical framework represents an important attempt to combine scientific regulation with traditional medicine, although implementation challenges remain. China strongly supports TCM through dedicated legislation, while Japan maintains highly standardised Kampo regulation based on approved formulae and pharmacopoeial control.
Despite these differences, all systems face common challenges involving raw material variability, adulteration, herb-drug interactions, and weak pharmacovigilance infrastructure. Future progress will require harmonised quality standards, improved analytical methods, stronger safety monitoring, and evidence models appropriate for complex botanical products.
A balanced regulatory approach should neither reject traditional knowledge nor accept it uncritically. Instead, phytopharmaceutical regulation should integrate modern scientific evaluation with the historical experience of traditional medicine systems. Greater international cooperation and scientific innovation will be essential for achieving safe, effective, and globally accepted phytopharmaceutical regulation.
REFERENCES


Poonam Borse*, Lalan Wagh, Avinash Darekar, Regulatory Requirements For Phytopharmaceuticals: A Comparative Analysis Of India, The United States, Europe, China, And Japan, Int. J. Sci. R. Tech., 2026, 3 (6), 104-120. https://doi.org/10.5281/zenodo.20503146
 10.5281/zenodo.20503146
10.5281/zenodo.20503146