
We use cookies to ensure our website works properly and to personalise your experience. Cookies policy
1Department of Pharmacy Practice, St. Johns college of Pharmaceutical Sciences, Yerrakota, Yemmiganur, Kurnool, Andhra Pradesh, India.
2Orthopedic, Sunrise Hospital, Kurnnool, Andhra Pradesh, India.
Background: Pharmacoeconomics refers to the scientific discipline that compares the value of one pharmaceutical drug or drug therapy to another. The fixed dose combinations (FDCs) of muscle relaxants, non-steroidal anti-inflammatory drugs and paracetamol are commonly prescribed in the treatment of acute lower backache associated with muscle spasm. Objectives: The present was undertaken with aim to identify best drug combination treatment approach that reduce lower back ache associated with muscle spasm and to reduce the financial burden to the patients. Methodology: A Prospective observational study was conducted over a period of 2 weeks in Sunrise hospital, Kurnool. A total of 100 patients between ages range from 18 and 60 years having low back pain were randomly divided into two groups. Group A was prescribed thiocolchicoside (4 mg) + aceclofenac (100 mg) + paracetamol (325 mg) while Group B was prescribed chlorzoxazone (500 mg) + aceclofenac (100 mg) + paracetamol (325 mg) orally twice daily for 14 days. Severity of pain at rest and on movement was recorded using visual analogue scale. Muscle spasm was evaluated by hand-to-floor distance. Result:There was statistically significant reduction in severity of pain and muscle spasm on 7th day and day 14 in both groups.Among two groups patients receiving Thiocolchicoside, aceclofenac, and paracetamol have shown better improvement in terms of cost effectiveness when compared to chlorzoxazone, aceclofenac, and paracetamol. Conclusion: This pharmacoeconomic analysis shows that Thiocolchicoside, aceclofenac, paracetamol is more cost-effective as compared to chlorzoxazone, aceclofenac and paracetamol.
Introduction to Pharmacoeconomics
Pharmacoeconomics (PE), a subfield of health economics, evaluates the behavior of individuals, firms, and markets regarding pharmaceutical products, services, and programs. Operationally, it compares the clinical, economic, or humanistic outcomes and costs (resource consumption) of pharmaceutical alternatives from selected perspectives. The objective is to identify, measure, value, and link resource consumption to outcomes to establish relative medical worth. Drawing from economics, epidemiology, medicine, pharmacy, and social sciences , PE evaluations are categorized into economic evaluations—such as cost-minimization (CMA), cost-benefit (CBA), cost-effectiveness (CEA), cost-utility (CUA), and cost-consequences (CCA) analyses —and humanistic evaluations, which focus on quality of life, patient preferences, and satisfaction
Foundations of Pharmacoeconomics (PE)
Pharmacoeconomics (PE), a specialized subfield of health economics, evaluates the behavior of individuals, firms, and markets regarding pharmaceutical products, services, and programs. Operationally, PE identifies, measures, values, and links the resource consumption (costs) of alternative pharmaceutical interventions to their clinical, economic, or humanistic consequences. This dual analysis allows stakeholders to establish the relative medical worth of competing strategies. PE methodologies integrat e principles from economics, epidemiology, medicine, pharmacy, and the social sciences.
Classification of Evaluative Frameworks
Pharmacoeconomic evaluation techniques are systematically grouped based on how outcomes are framed:
Cost-Effectiveness Analysis (CEA) Methodology
CEA represents the most widely implemented economic evaluation technique. It is designed to compare interventions that yield an identical natural clinical outcome (e.g., years of life saved, ulcers healed, millimeters of mercury reduction in blood pressure). Because it relies on these specific natural units, CEA cannot compare treatments across distinct, unrelated medical domains.
The economic efficiency of independent and mutually exclusive health strategies is quantified using two primary analytical metrics:
1. Average Cost-Effectiveness Ratio (ACER)
Calculated for standalone or independent programs to define the isolated cost required to achieve a single unit of clinical outcome:
ACER = Net Cost/ Net Health Benefit
2. Incremental Cost-Effectiveness Ratio (ICER)
The essential diagnostic tool for choosing between competing, mutually exclusive therapeutic strategies. It measures the additional financial expenditure required to achieve one additional unit of clinical benefit over the standard comparator:
ICER = Cost of New Program - Cost of Current Program \ Effectiveness of New Program - Effectiveness of Current Program
Sequential Procedural Steps in CEA
Conducting a comprehensive CEA requires a rigorous, multi-stage framework:
Pharmacological Profiles of Select Analgesic and Myorelaxant Agents
Evaluating the economic and clinical value of pharmaceutical alternatives requires a baseline understanding of their individual pharmacokinetic (PK) and pharmacodynamic (PD) profiles.
Aceclofenac
Paracetamol (Acetaminophen)
Chlorzoxazone
Thiocolchicoside
Materials and Methods
AIM: The main aim of our study was to find out the cost effevtiveness ratio for Aceclofenac, paracetemol and thiocolchocoside vs Aceclofenac,paracetemol and chlorzoxazone
OBJECTIVES:
STUDYSITE: Sunrise hospital, Kurnool
STUDY DURATION: The study was conducted over a period of 6 months
SAMPLE SIZE: 92 subjects (each group 46 subjects) contains two groups
Group-A: 46 ( Thiocolchicoside (4 mg) + aceclofenac (100 mg) + paracetamol (325mg)
Group–B:46 (chlorzoxazone (500mg) +aceclofenac (100mg) +paracetamol (325 mg)
STUDYDESIGN: Prospective observational study
STATISTICAL MEASURES: The collected data will analysed by using MS-EXCELsoftware, statistics to produce results from the data
SOURCE OF DATA COLLECTION
STUDY CRITERIA INCLUSION CRITERIA
EXCLUSION CRITERIA:
RESULTS AND DISCUSSION:
A total of 97 patients who met the selection criteria were enrolled in the study. Among them, 3 from Group A and 2 from group B were dropped out because of loss of follow-up. Therefore, a total of 92 patients, 46 from group A and 46 patients from group B completed the study as shown in Table 1.
|
|
Aceclofenac, Paracetamol And Thiocolchocoside (Zeroket-TH) Group A |
Aceclofenac,Paracetamol And Chlorzoxazone (Group Acebolic-MR) Group B |
|
Patients enrolled in study |
49 |
48 |
|
Patients dropped out |
3 |
2 |
|
Patients completed in study |
46 |
46 |
Table 1: Enrolment of patients in both treatment group
Figure 1: Gender-wise distribution in our study includes both group A and group B. Among 92 patients 42 (46%) patients are males and 50 (54%) patients are females as shown in fig 6.1and also shown in table representation in table.6.2
Figure 1: Gender wise categorization
|
|
Male |
Female |
|
No. of patients |
42 |
50 |
Table 2: Gender distribution
Figure 2: Represents that gender in different age groups is as follows years, 18-28 years age groups male are 5 and female are 6, 28-38 years age groups males are 6and females are 5, 38-48 year age groups male are 5 and females are 7,48-60 years age groups male are 5 and females are 7
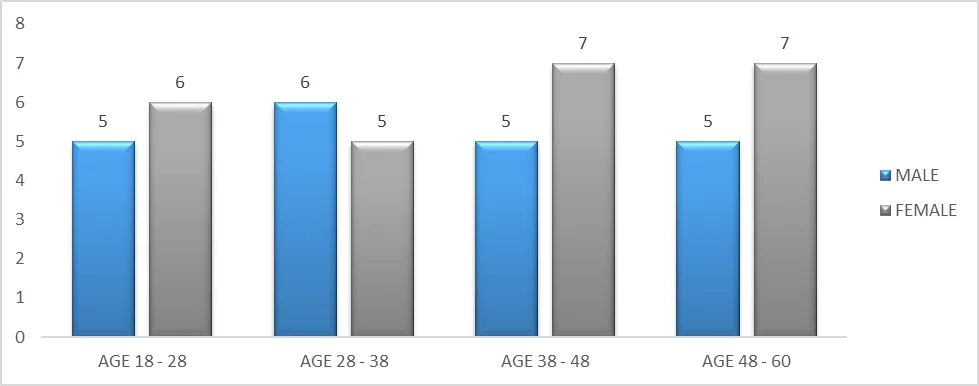
Figure 2: Gender and age wise distribution in aceclofenac(100mg) + paracetamol(325mg) + thiocolchocoside(4mg)
Figure 3: Represents that gender in different age groups is as follows years, 18-28 years age groups male are 4 and female are 6, 28-38 years age groups males are 6and females are 7, 38-48 years age groups male are 3 and females are 6, 48-60 yearsage groups male are 6 and females are 8.
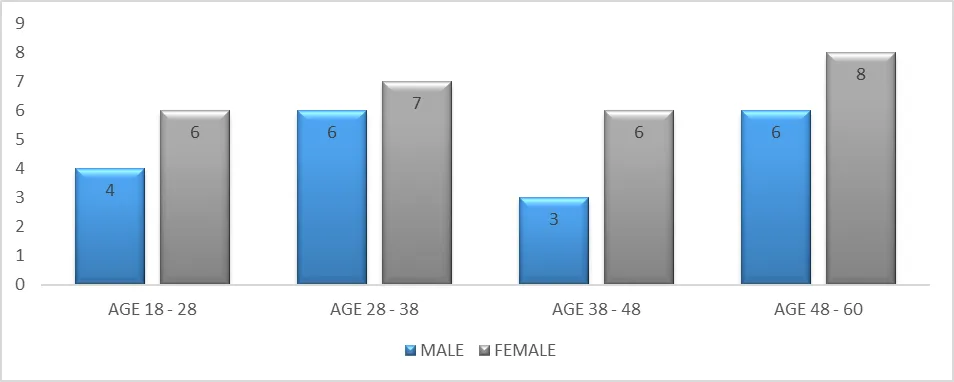
Figure 3: Gender and age wise distribution in Aceclofenac (100mg) +Paracetamol(325mg) + Chlorzoxazone(500mg)
Table 3 Represents the age-wise distribution in both groups, ZEROKET-TH 18-28 yearsage patients are 11, 28-38 years age patients are 11, 38-48 years age patients are 12, 48-60 years age group patients are 12, and ACEBOLIC MR18-28 year age patients are 10, 28-38 years age patients are 12, 38-48 years age patientsare 9, 48-60 years age group patients are 14.
|
|
Age 18-28 |
Age 28-38 |
Age 38-48 |
Age 48-60 |
|
ZEROKET-TH |
11 Patients |
11 Patients |
12 Patients |
12 Patients |
|
ACEBOLIC MR |
10 Patients |
12 Patients |
09 Patients |
14 Patients |
Table 3: Age wise distribution in both groups
|
S.no |
Score |
1st Visit |
1st follow up |
||||||
|
|
A |
% |
B |
% |
A |
% |
B |
% |
|
|
1 |
No pain |
0 |
0 |
0 |
0 |
0 |
0 |
0 |
0 |
|
2 |
Mild |
0 |
0 |
0 |
0 |
22 |
48% |
15 |
33 % |
|
3 |
Moderate |
0 |
0 |
0 |
0 |
21 |
46% |
17 |
37% |
|
4 |
Severe |
30 |
65% |
31 |
67% |
3 |
6% |
14 |
30% |
|
5 |
Worst |
16 |
35% |
15 |
33% |
0 |
0 |
0 |
0 |
Table 4: Effectiveness of pain intensity in Group-A and Group-B
|
S.no |
Score |
2nd follow up |
|||
|
|
A |
% |
B |
% |
|
|
1 |
No pain |
18 |
39% |
11 |
24% |
|
2 |
Mild |
19 |
41% |
23 |
50% |
|
3 |
Moderate |
9 |
20% |
12 |
26% |
|
4 |
Severe |
0 |
0 |
0 |
0 |
|
5 |
Worst |
0 |
0 |
0 |
0 |
Figure 4a Prevalence of pain intensity in Group-A and Group-B in 1st first visit:
In the group -A,44% of patients having worst pain and 56% of patients having severe pain.In the group-B,49% of patients having worst pain and 51% of patients having severe pain.
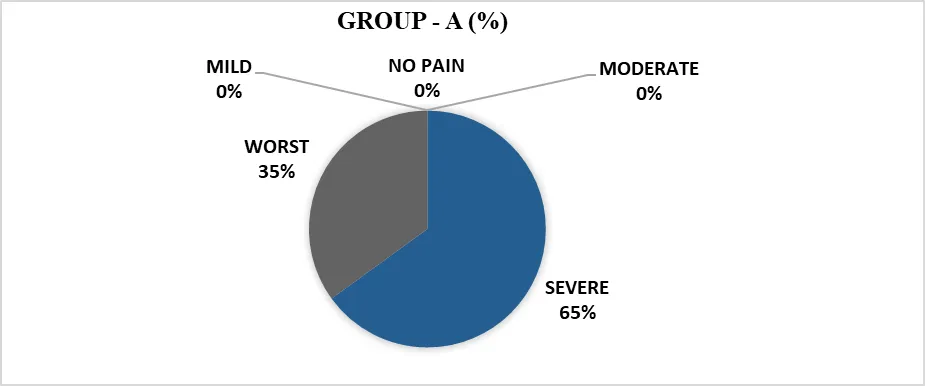
6.4a. Prevalence of pain intensity in Group - A and Group -B in 1st Visit.
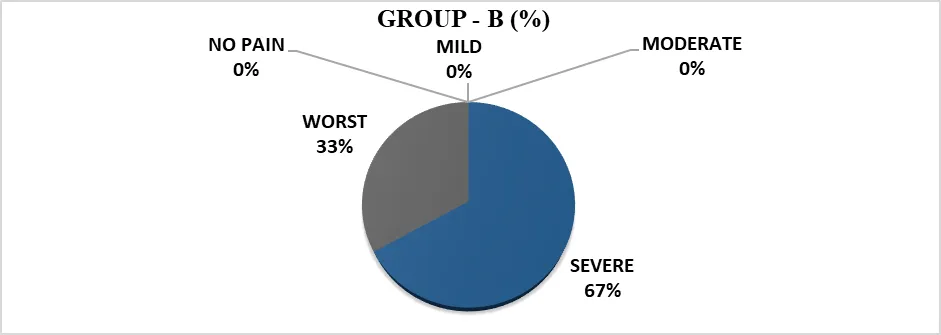
Figure 4b Prevalence of pain intensity in Group-A and Group-B in 1stfollow up:
In 1st follow up, we are observing that in group-A patients has 48% mild pain, 46% moderate pain and 6% severe pain. In Group- B patients has33% mild pain, 37% moderate pain and30% severe pain.
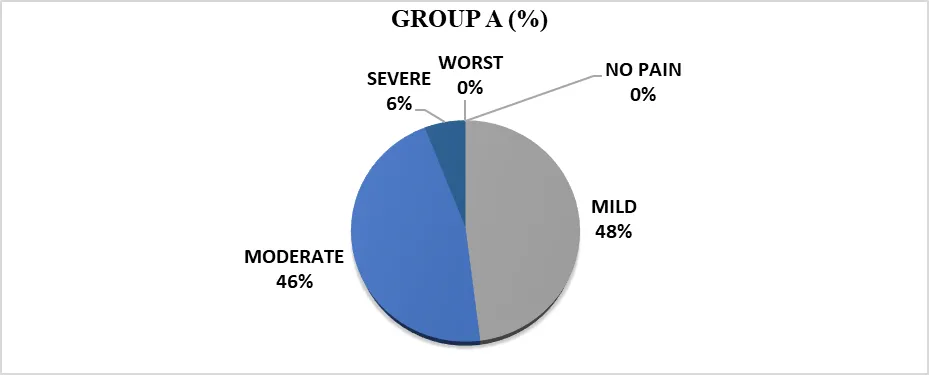
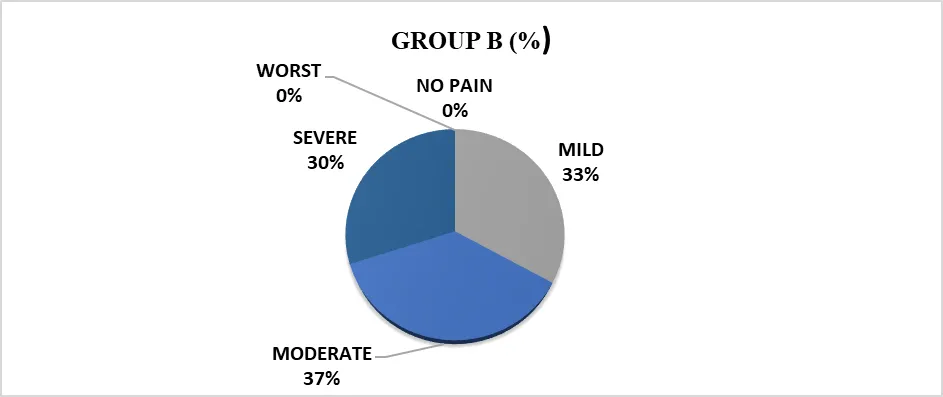
4b. Prevalence of pain intensity in Group - A and Group -B in 1st follow up.
Figure 4c: Prevalence of pain intensity in Group-A and Group-B in 2nd follow up:
In 2nd follow up, we are observing that in group-A patients has 39% no pain, 41% mild pain and 20% moderate pain. In Group- B patients having 24% has no pain,50% mild pain and 26% moderate pain.
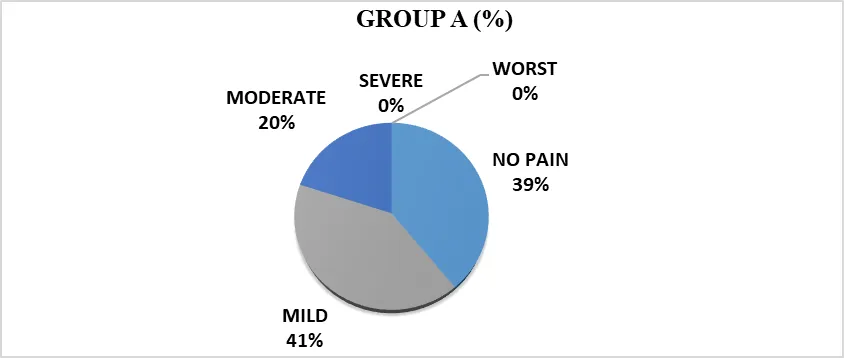
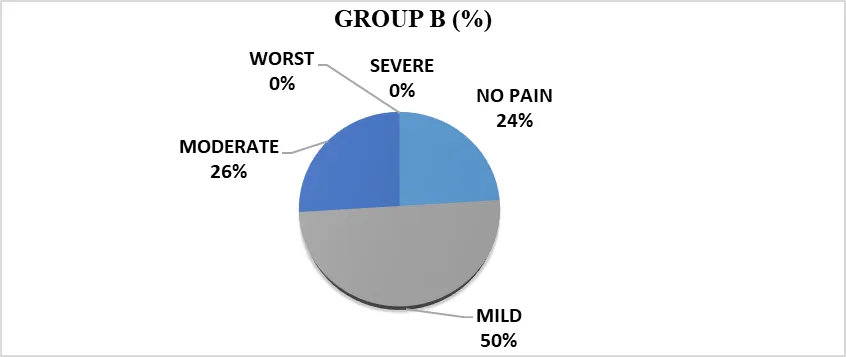
4c. Prevalence of pain intensity in Group - A and Group -B in 2nd follow up
Figure 5 and Table 5 Represent changes in Pain intensity (VAS) from baseline to 2 weeks on treatment with both combination drugs (Group A: Aceclofenac, Paracetamol&Thiocolchicosideand Group B:Aceclofenac, Paracetamol& Chlorzoxazone) and there was a great proportion of reductions in Pain score (VAS) from week to week in our study, we observed that there was a significant reduction in Pain score.
In Group A Pain score (VAS) From the first visit to 1st follow up period there was a reduction in average of 4.21 of pain score and from 0 to 2 weeks (1st visit to second follow up) accumulatively there was a reduction in pain intensity on average of 7.02of pain score respectively.
In Group B Pain score (VAS) From the first visit to 1st follow up period there was a reduction in average of 3.47 of pain score and from 0 to 2 weeks (1st visit to second follow up) accumulatively there was a reduction in pain intensity on average of 6.01 of pain score respectively.
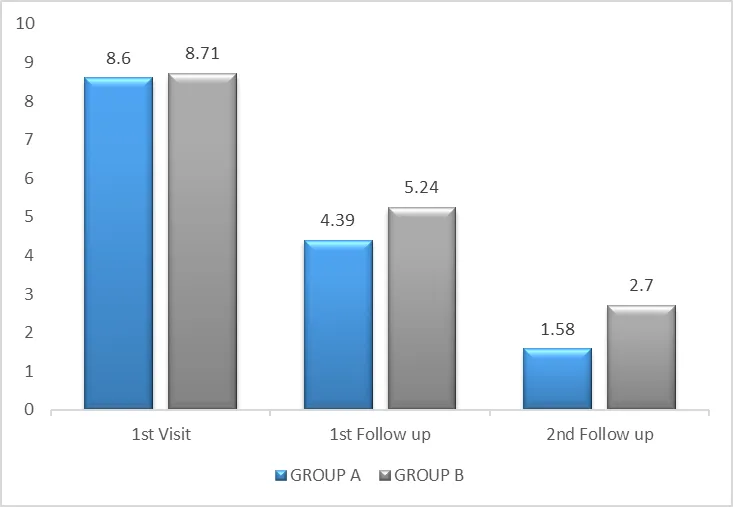
Figure 5: Changes in pain score (VAS) from the first visit to second follow up withboth combination drugs Aceclofenac (100mg) + paracetamol (325mg) + Thiocolchocoside (4mg) and Aceclofenac (100mg) + Paracetamol (325mg) + Chlorzoxazone (500mg)
|
Visits |
GROUP A (Pain score) (MEAN ±SD) |
GROUP B (Pain score) (MEAN ±SD) |
P VALUE |
|
First visit |
8.6±1.64 |
8.71±1.09 |
0.711724 |
|
First follow up |
4.39±1.68 |
5.24±2.00 |
0.029593 |
|
Second follow up |
1.58±1.72 |
2.7±2.11 |
0.008251 |
Table 5: Changes in pain score (VAS) from the first visit to second follow up with both combination drugs Aceclofenac (100mg) + paracetamol (325mg) + Thiocolchocoside (4mg) and Aceclofenac (100mg) + Paracetamol (325mg) + Chlorzoxazone (500mg)
Figure 6 and Table 6 Represent changes in FTF distance from baseline to 2 weeks on treatment with both combination drugs (Group A: Aceclofenac, Paracetamol & Thiocolchicoside and Group B:Aceclofenac, Paracetamol & Chlorzoxazone) and there was a great proportion of reductions in FTF distance from week to week in our study, we observed that there was a significant reduction in FTF distance.
In Group A FTF distance from the first visit to 1st follow up period there was a reduction in average of 19.84cm and from 0 to 2 weeks (1st visit to second follow up) accumulatively there wasaverage reduction of 30.71cm respectively.
In Group B FTF distance from the first visit to 1st follow up period there was a reduction in average of 16.04cm and from 0 to 2 weeks (1st visit to second follow up) accumulatively there was average reduction of 27.46cm respectively.
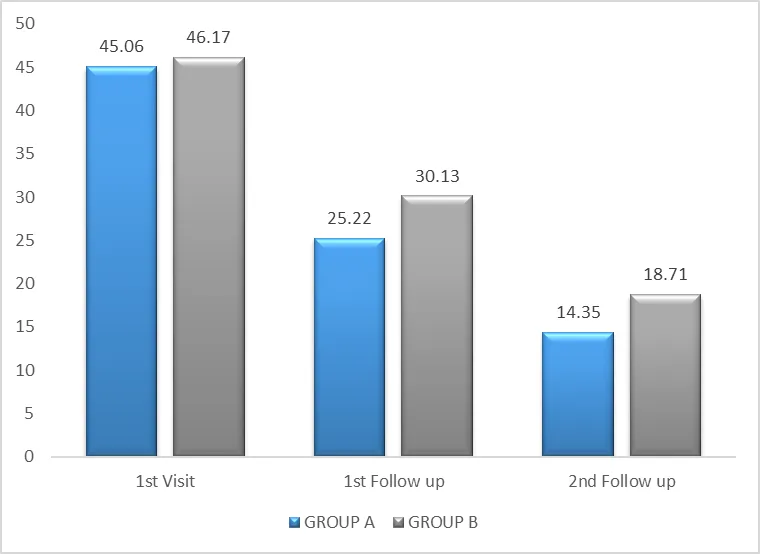
Figure 6: Changes in FTF distancefrom the first visit to second follow up withboth combination drugs Aceclofenac (100mg) + paracetamol (325mg) + Thiocolchocoside (4mg) and Aceclofenac (100mg) + Paracetamol (325mg) + Chlorzoxazone (500mg)
|
Visits |
GROUP A (FTFD) (MEAN ±SD) |
GROUP B (FTFD) (MEAN ±SD) |
P VALUE |
|
First visit |
45.06±7.40 |
46.17±6.45 |
0.446043 |
|
First follow up |
25.22±4.96 |
30.13±6.51 |
0.000134 |
|
Second follow up |
14.35±4.43 |
18.71±6.08 |
0.000161 |
Table 6: Changes in FTF distance from the first visit to second follow up withboth combination drugs Aceclofenac (100mg) + paracetamol (325mg) + Thiocolchocoside (4mg) and Aceclofenac (100mg) + Paracetamol (325mg) + Chlorzoxazone (500mg)
Table 7 Represents the costs of both drugs, The cost of the Aceclofenac (100mg) + Paracetamol (325mg) + Thiocolchocoside (4mg) (ZEROKET TH) is 140/- Rs and The cost of Aceclofenac (100mg) + Paracetamol (325mg) + Chlorzoxazone (500mg) (ACEBOLIC MR) is 175/- Rs.
|
|
ZEROKET TH |
ACEBOLIC MR |
|
Cost per 10 tablets |
140/- Rs |
175/- Rs |
Table 7: Cost of the both drugs
Table 8. Represents the cost evaluation of both drugs in low back ache associated with muscle spasm patients. The drug Aceclofenac (100mg) + Paracetamol (325mg) + Thiocolchocoside (4mg)cost for reducing 1 point of pain score in VAS (INR)is 56 and the cost for reducing 1cm of FTF distance (INR) is 12.76.
Aceclofenac (100mg) + Paracetamol (325mg) + Chlorzoxazone (500mg)cost for reducing 1 point of pain score in VAS (INR)is 81.53and the cost for reducing 1cm of FTF distance (INR) is 17.84.
|
TREATMENT |
PAIN SCORE (VAS) |
FTF distance |
|
Aceclofenac, Paracetamol& Thiocolchicoside |
56 |
12.76 |
|
Aceclofenac, Paracetamol&Chlorzoxazone |
81.53 |
17.84 |
Table 8: Cost evaluation of both drugs in low back ache with muscle spasm patients (for reducing one point of pain intensity in VAS and 1 cm of FTF distance)
Cost evaluation of both drugs for reducing 1 point of pain intensity in VAS and 1cm of FTF distance per day
Aceclofenac, Paracetamol& Thiocolchicoside (ZEROKET-TH) costs for reducing 1 point of pain intensity in VAS is 4 INR and 1cm of FTF distance is 0.91 INR per day.
Aceclofenac, Paracetamol& Chlorzoxazone (ACEBOLIC MR) costs for reducing 1 point of pain intensity in VAS is 5.82 INR and 1cm of FTF distance is 1.27 INR per day.
DISCUSSION:
Low back pain (LBP) describes pain between the lower edge of the ribs and the buttock. It can last for a short time (acute), a little longer (sub-acute) or a long time (chronic). It can affect anyone. LBP makes it hard to move and can affect quality of life and mental well-being.
Muscle spasms (also called muscle cramps) occur when your muscle involuntarily and forcibly contracts uncontrollably and can't relax.
Lower back spasms can result from poor posture, muscle overuse, and sprains and strains. The incidence of acute backache increasing in the present scenario due to modernization, lack of exercise and postural problems.
The treatment and prevention of LBP associated with muscle spasm significant costs, and rising demand for clinical intervention is set to further increase the burden on healthcare resources. Therefore, it is essential to identify the most cost effective therapeutic options in order to make optimal use of available resources. Thus, in low back spasm, muscle relaxants with analgesics are considered important.
The study reported here is a pharmacoeconomic approach in comparison of aceclofenac (100mg) + paracetamol (325mg) + thiocolchocoside (4mg);Aceclofenac (100mg) + Paracetamol (325mg) + Chlorzoxazone (500mg)in the treatment of low back spasmpatients were used in this study by application of cost-effective analysis. One of the main objective was to identify the best drug combination treatment approach that reduces pain intensity for two weeks in terms of cost. It was reported that combination therapy of Aceclofenac, Paracetamol & Thiocolchicoside is more cost-effective as compared to Aceclofenac, Paracetamol & Chlorzoxazonewhen the cost per reduction in pain intensity is considered.
Thiocolchicoside has a selective and potent affinity for g-aminobutyric acid A (GABA-A) receptors and acts on muscular contractures by activating the GABA inhibitory pathways thereby behaving as a potent muscle relaxant.Aceclofenac is a NSAID that potently inhibits the cyclo-oxygenase enzyme (COX) that is involved in the synthesis of prostaglandins, which are inflammatory mediators that cause pain, swelling, inflammation. Paracetamol is antipyretic that relates to the inhibition of CNS cyclooxygenase (COX) enzyme activities. Together helps in relieving muscular pain. It works by blocking the release of certain chemical messengers that cause pain, inflammation, and fever. Chlorzoxazone is muscle relaxant that acts to relax certain muscles in your body and relieve the discomfort caused by acute (short-term), painful muscle or bone conditions. Together with paracetamol and aceclofenac combination works to relieve pain, inflammation, and swelling in conditions that affect muscles. Also, it effectively relieves muscle stiffness or spasm, thereby improving muscle movement.
Sanjeev Kumar, et al., have performed study on “To compare the efficacy and safety of FDC of thiocolchicoside and aceclofenac vs chlorzoxazone, aceclofenac and paracetamol in patients with acute lower backache associated with muscle spasm” The study concluded that the findings confirm that FDC of thiocolchicoside and aceclofenac is a preferred option for patients with lower backache pain associated with muscle spasm. This may affect the efficacy and safety of both drugs in treatment of LBP associated with muscle spasm.
This pharmacoeconomics study was carried out for a comparative evaluation of the cost-effectiveness of Aceclofenac, Paracetamol & Thiocolchicoside and Aceclofenac, Paracetamol & Chlorzoxazone in low back spasm patients. There was a clinically significant difference in the efficacy of both drug molecules. As per this comparative analysis, it was found thatAceclofenac, Paracetamol & Thiocolchicoside is more cost-effective as compared to Aceclofenac, Paracetamol & Chlorzoxazone in terms of reducing both pain intensity on VAS as well as FTF distance.
The study results showed a significant difference in the cost of both drug molecules. The cost per reduction of 1 point of pain score on VAS was found to be 56 INR by Aceclofenac, Paracetamol & Thiocolchicoside, whereas 81.6 INR by Aceclofenac, Paracetamol & Chlorzoxazone. The cost per reduction of 1cm of FTF distance was found to be 13.57 INR by Aceclofenac, Paracetamol & Thiocolchicoside, whereas 19.50 INR by Aceclofenac, Paracetamol & Chlorzoxazone.
REFERENCES

Maka Venkateswarlu1, K. Jagadeesh1*, D. Rajaiah2, A Pharmacoeconomic Approach In Comparision Of Aceclofenac, Paracetamol And Thiocolchocoside Vs Aceclofenac, Paracetamol And Chlorzoxazone In Treatment Of Lower Backache Associated With Muscle Spasm By Application Of Cost- Effective Analysis, Int. J. Sci. R. Tech., 2026, 3 (5), 884-896. https://doi.org/10.5281/zenodo.20395182
 10.5281/zenodo.20395182
10.5281/zenodo.20395182