
We use cookies to ensure our website works properly and to personalise your experience. Cookies policy
Department of Neurological Physiotherapy R.V.S College of Physiotherapy, Coimbatore, The Tamil Nadu Dr. M.G.R. Medical University, Chennai, Tamil Nadu, India.
Effectiveness of Sensory Integration Therapy on Gross Motor Function among Spastic Diplegic Cerebral Palsy. Objectives:Research to ascertain the effectiveness of sensory integration therapy and conventional physical therapy on gross motor function among spastic diplegic cerebral palsy. Design :Pre and Post test of experimental study design is adopted. Setting :The site of the study was R.V.S College of Physiotherapy Out-Patient department, Sulur,Coimbatore. 20 Spastic Diplegic Cerebral Palsy children aged 6-12 were selected conventional physical therapy and sensory integration was given 5 days in a week for 4 months. Result :On comparing the mean post-treatment GMFM-88 scores of both groups, Group A (sensory integration therapy) exhibited greater improvement than Group B (conventional physical therapy). Conclusion :The sensory integration therapy is found to be more effective in improving gross motor function in spastic diplegic cerebral palsy children.
Cerebral Palsy (CP) is a long-term motor disorder caused by irreversible but non-progressive injury to the developing brain, usually before birth or in early infancy. Spastic CP is the most common type, marked by increased muscle tone and exaggerated reflexes due to upper motor neuron damage (WHO 2007; Bax 2005). CP affects nearly 1 million individuals in the U.S., with about 1 in 345 children diagnosed annually. Around 90% of cases occur prenatally or during birth, with risks increased by prematurity, low birth weight, multiple births, or kernicterus. Diagnosis is often delayed until age two, and nearly half of affected children show cognitive delays (Schmitt 2025).
Spastic diplegic CP typically begins with low tone that progresses to spasticity, causing delayed milestones such as sitting, crawling, and walking. Children often display tight legs, toe-walking, scissoring gait, and balance difficulties, with some developing skeletal issues like coxa valga. Cognitive delay occurs in about 30% of cases, though many maintain normal intelligence (Abdel 2024). While diplegia primarily affects the lower limbs, weakness in core muscles and reduced proprioception are common, and upper limb and hand function—crucial for daily tasks—may also be mildly affected (Elbasan 2017).
Upper limb motor control involves the motor cortex, internal capsule, corticospinal tracts, basal ganglia, and cerebellum. In spastic diplegia, periventricular white matter damage mainly affects lower-limb fibers, though some upper-limb pathways may be involved, leading to difficulties with shoulder movement, elbow extension, and hand coordination (Levitt 2018). Disruption of motor signals causes increased tone, poor voluntary control, and altered sensation, sometimes resulting in bent elbows or forearm rotation during movement, reducing efficiency (Rosenbaum 2007).
Clinical management relies on tools like the GMFM-88, which measures gross motor skills and is especially useful for evaluating standing, walking, and jumping in diplegia (Russell 2013). Sensory Integration Therapy uses play-based tasks to enhance sensory processing through neuroplasticity, with children classified as mild, moderate, or severe based on motor and cognitive status (Ayres 1972). Conventional physiotherapy remains essential, focusing on stretching, strengthening, posture correction, and functional training to improve mobility, balance, and independence (Damiano 2006).
II. METHODOLOGY
The study was conducted in the Physiotherapy outpatient department of R.V.S College of Physiotherapy Out-Patient department, Sulur , Coimbatore.
The study design was a Pre and Post test experimental study conducted over a period of 4 months.
•Clinically Diagnosed Patients with spastic diplegic
• GMFCS level II-III
• Age group between 6-12years
• Both Male and Female
•Able to understand command ; pediatric mini-mental status examination (MMSE score >23).
• Patient with cognitive impairments
• uncontrolled seizures for past six months
• Severe Deformities
• Visual impairments
• Mentally unstable patients
• Uncooperative patients
Institutional review board approved this two group experimental study. A total of 20 patients were selected on the basis of inclusion criteria and exclusion criteria and were divided equally into two groups, group A and group B using randomized method. Each group consisted of 10 patients, the study procedures were explained to the patients and informed consent was obtained prior to the study .The group A performed sensory integration therapy while group B perform conventional physical therapy .Both group receive treatment for four week .The outcome measure for gross motor function was measured by gross motor function scale88.
The Gross Motor Function Measure 88(GMFM88)
This is a standardized tool used to observe and track changes in motor skills in children with cerebral palsy. In this assessment, the GMFM-88 version is commonly used. The evaluation takes place in a calm, safe environment ;where the child feels comfortable and free to move. To allow for unrestricted movement, the child is dressed in loose, comfortable clothing. A trained physiotherapist gently guides the child through the assessment, observing how they perform a series of everyday movements and activities.
In every session, activities and the following exercises were done by the groups.
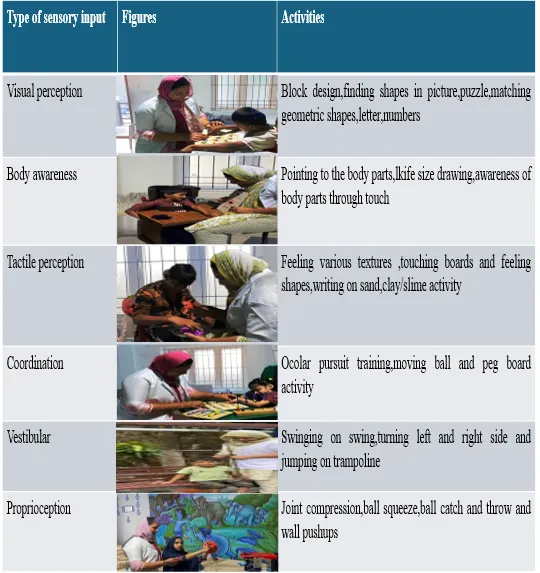
Group A :
The experimental group was given SIT for hour, which included the following. Vision perception activity, Body awareness ,Tactile perception, Visual-motor coordination training.
The exercises were introduced gradually, with each level of difficulty added only when the child was able to perform the task comfortably and without strain. Therapy sessions were conducted for one hour a day, five days a week, over a period of four week with appropriate rest breaks to prevent fatigue. The children’s progress were assessed using the Gross Motor Function Measure 88 before starting the intervention and after completing the therapy program.5 sessions of one hour duration in a week with 10-15 rep is given.
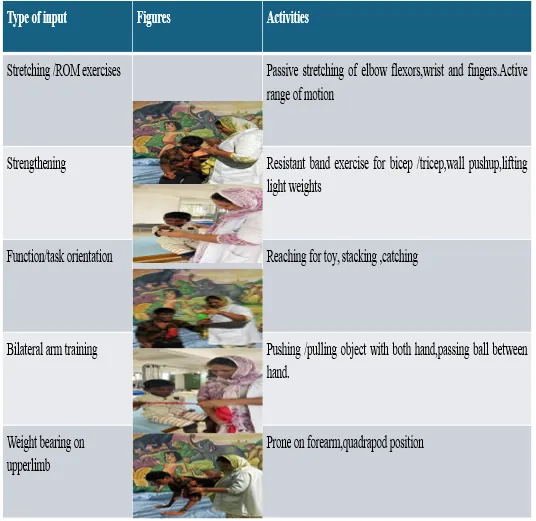
Group B
This received conventional physical therapy focused on power. This included standard exercises such as passive range of motion, stretching, and strengthening exercises.
In addition, children were guided through various transitional movements—such as rolling, sitting, crawling, kneeling, lying down, standing, and walking. All exercises were performed by a trained physiotherapist and tailored to support each child’s motor development and mobility. 5 sessions of one hour duration in a week with 10-15 rep is given.
|
Measurement |
Mean |
Mean difference |
Standard deviation |
Paired ‘t’ value |
|
Pre test Post test |
64.7 73.6 |
8.9 |
0.994 |
28.3 |
Table 1 Data analysis and Results
*0.005 Level of Significance
Table 1: Mean value, mean difference, standard deviation and paired ‘t’ value between pre-test and post-test scores of GMFM88 among Group A (sensory integration therapy).
In Group A for gross motor function the calculated paired t value is 28.3 and ‘t table value is 3.250 at 0.005 level of significance. Since the calculated ‘t’ value is more than ‘t’ table value there is significant difference in gross motor function following sensory integration therapy among spastic diplegic cerebral palsy children.
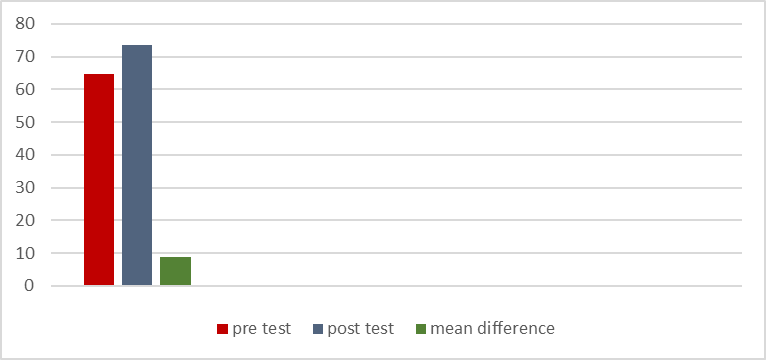
Figure 6: Graphical representation of pre test mean, post test mean and mean difference of gross motor function among Group A.
|
Measurement |
Mean |
Mean Difference |
Standard deviation |
Paired ‘t’ value |
|
Pre test Post test |
64.5 67.9 |
3.4 |
2.75 |
3.9 |
*0.005 Level of significance
Table 2: shows Mean value, mean difference, standard deviation and paired ‘t’ value between pre-test and post-test scores of GMFM88 among Group B (Conventional physical therapy).
In Group B for gross motor function the calculated paired t value is 3.9 and ‘t’ table value is 3.250 at 0.005 level of significance. Since the calculated ‘t’ value is more than ‘t’ table value there is significant difference in gross motor function following Conventional physical therapy among spastic diplegic cerebral palsy children.
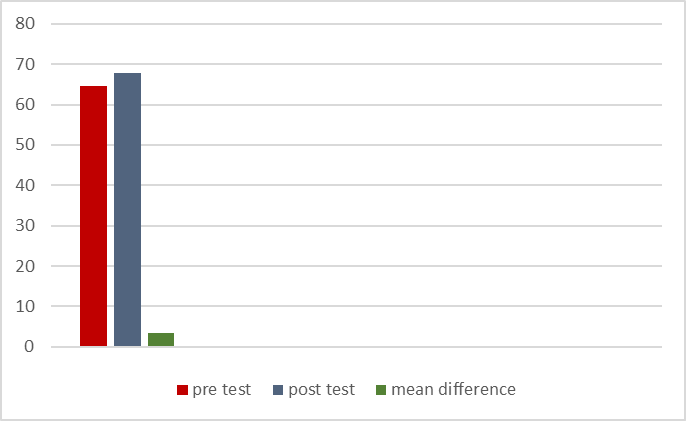
Figure 7: Graphical representation of pre test mean, post test mean and mean difference gross motor function among Group
|
Groups |
Improvement |
Standard deviation |
Unpaired ‘t’ value |
|
|
Group A |
Mean |
Mean difference |
1.96 |
5.93 |
|
8.9 |
5.5
|
|||
|
Group B |
3.4 |
|||
*0.005 level of significance
Table 3: Mean value, mean difference, standard deviation and unpaired ‘t’ value of GMFM88 between Group A and Group B
In Group A and Group B for gross motor function the calculated unpaired ‘t’ value is 5.93 and ‘t’ table value is 2.101 at 0.005 level of significance since the calculated ‘t’ value is more than ‘t’ table value there is significant difference between sensory integration therapy and conventional physical therapy in management of gross motor function among spastic diplegic cerebral palsy.
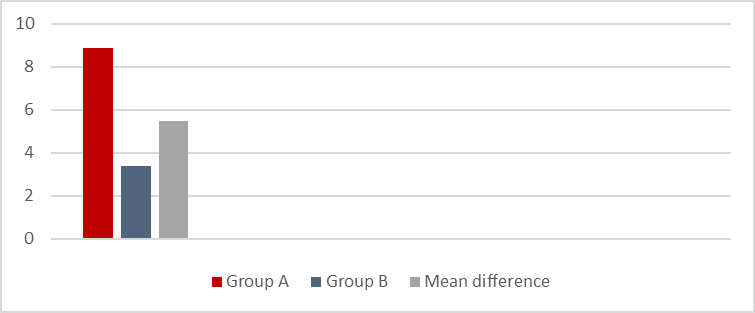
Figure 8: Graphical representation of unpaired ‘t’ value for gross motor function between group A and group B
A total of twenty children diagnosed with spastic diplegic cerebral palsy participated in the study. They were randomly divided into two equal group. Children in group A received sensory integration therapy, while those in Group B received conventional physical therapy.
Prior to the commencement of the interventions, all participants were evaluated using the Gross Motor Function Measure-88 (GMFM-88) to assess their baseline gross motor function. After completing the 4 weeks of intervention the GMFM-88 was repeated to determine the extent of improvement in each group.
The statistical analysis of pre- and post-intervention scores using a paired t-test revealed a calculated t-value of 28.3, which is significantly higher than the critical table value of 3.2 at a 0.005 level of significance.This clearly indicates a highly significant improvement in gross motor function following sensory integration therapy in spastic diplegic cerebral palsy children.
The paired t-test for Group B showed a calculated t-value of 3.9, which exceeds the critical table value of 3.250 at the 0.005 level of significance.These results suggest that conventional physical therapy also produced a statistically significant improvement in gross motor function among spastic diplegic cerebral palsy children, though the magnitude of change was comparatively less than that observed in sensory integration therapy.
To compare the overall effectiveness of both therapeutic approaches, an unpaired t-test was used to analyze the post-intervention GMFM-88 scores between group A and group B. The test revealed a calculated t-value of 5.93, which is well above the critical table value of 2.101 at a 0.005 significance level.This statistically significant result confirms that there is a considerable difference in gross motor function improvement between the two groups.
On comparing the mean post-treatment GMFM-88 scores of both groups, Group A exhibited greater improvement than group B. Hence it is concluded that sensory integration therapy is more effective than conventional physical therapy in the management of gross motor function among spastic diplegic cerebral palsy children.
III. DISCUSSION
The purpose of this study was to compare the effectiveness of sensory integration therapy (SIT) and conventional physiotherapy on gross motor function in children with spastic diplegic cerebral palsy. Twenty children were randomly divided into two groups. Group A received sensory integration therapy, and Group B received conventional physiotherapy. Improvement was measured using the GMFM-88 scale.
The results of the study showed that both therapies improved gross motor function, but sensory integration therapy produced greater improvement compared to conventional physiotherapy.
Improving gross motor function is an important goal in the management of children with cerebral palsy. Children in Group A demonstrated significantly better gains in GMFM-88 scores, indicating improved abilities in activities such as sitting, standing, and walking.
Previous studies also support these findings. Carlsen reported that children who received sensory integration therapy for two hours per week over six weeks showed better motor outcomes. Similarly, Sham Soddini et al. (2009) found significant improvements in motor function after twelve weeks of sensory integration therapy in children with spastic diplegic cerebral palsy. A follow-up study in 2010 confirmed continued progress.
Sensory integration therapy helps children process sensory information more effectively. According to Ayres (1972), sensory integration is the brain’s ability to organize sensory input for purposeful movement. Poor sensory processing can lead to difficulties in movement, participation, and emotional regulation, as explained by Bundy and Murray (2002).
In spastic diplegic cerebral palsy, early brain injury disrupts sensorimotor integration, leading to poor balance, coordination, and increased spasticity. Sensory integration therapy uses structured sensory activities that stimulate the vestibular, proprioceptive, and tactile systems, promoting neuroplasticity. This improves communication between sensory and motor areas of the brain, resulting in better posture, balance, motor planning, and gross motor skills (Warakthur, 2022).
Conventional physiotherapy also improves gross motor function by addressing neuromuscular problems such as muscle weakness, spasticity, and poor motor control. Through stretching, strengthening, balance training, and task-specific exercises, conventional therapy promotes neuroplastic changes and improves voluntary movement and postural stability (Eun Young, 2017).
CONCLUSION
This study was undertaken to compare the relative effectiveness of sensory integration therapy and conventional physical therapy in enhancing gross motor function among children diagnosed with spastic diplegic cerebral palsy. A total of twenty children with spastic diplegia were selected and randomly assigned into two equal groups. Group A received intervention through sensory integration therapy, while Group B was managed using conventional physiotherapeutic techniques.
Based on the results obtained, it can be concluded that both therapeutic approaches yielded statistically significant improvements in gross motor function. However, the outcomes were more favorable in the group that underwent sensory integration therapy, indicating a higher degree of effectiveness in enhancing motor performance when compared to conventional physiotherapy .
The study only assessed short term progress of the patient. Long term follow up is needed to evaluate the difference in the condition of the patient from current status.
RECOMMENDATION
Further study is needed to systematically determine the most efficacious protocol for each.
REFERENCES
Integration Therapy on Functional Mobility in Children With Spastic Diplegic Cerebral Palsy. Cureus, 15(9),
Integration Therapy on Functional Mobility in Children With Spastic Diplegic Cerebral Palsy. Cureus, 15(9),



Najeena P.*, Cathrine S., Franklin Shaju M. K., Effectiveness Of Sensory Integration Therapy On Gross Motor Function Among Spastic Diplegic Cerebral Palsy, Int. J. Sci. R. Tech., 2026, 3 (5), 996-1004. https://doi.org/10.5281/zenodo.20415077
 10.5281/zenodo.20415077
10.5281/zenodo.20415077