
We use cookies to ensure our website works properly and to personalise your experience. Cookies policy
1MOT-Neurology, PG Final Year, Chettinad School of Occupational Therapy, Chettinad Academy of Research and Education, Kelambakkam, Chennai, TN-603103India
2Chettinad School of Occupational Therapy, Chettinad Hospital and Research Institute, Chettinad Academy of Research and Education, Kelambakkam, Chennai, TN-603103 India, ORCID-ID: 0009-0007-6400-2733
The study intends to find the effectiveness of mirror therapy combined with theraputty hand activities on hand functions in stroke survivors. Materials and Methods: A RCT was conducted at Chettinad Hospital and Research Institute, Chennai. Sixty stroke survivors were selected and randomly allocated into 2 groups: experimental group (n = 30) and control group (n = 30). The CG was given conventional therapy, while the EG received mirror therapy combined with theraputty hand activities. The intervention was administered for 4 weeks. Hand function was assessed prior and following the intervention using the Fugl-Meyer Assessment (FMA) for Hand Function. Statistical analysis included paired and independent sample t-tests, and effect size was found by Cohen’s d. Results: The 2 groups were comparable at baseline, with no noteworthy difference in pre-test FMA scores. The CG showed minimal improvement, with mean FMA scores increasing from 16.43 ± 3.45 to 16.57 ± 3.87 (t is equal to -0.47, p is equal to 0.63), pointing no notable change. EG demonstrated substantial improvement, with mean FMA scores increasing from 15.67 ± 3.65 to 27.97 ± 2.11 (t = -23.21, p < 0.001). Post-test comparison revealed significantly higher FMA value in the EG than in the CG. Intervention produced an exceptionally large positive effect (Cohen’s d = 4.13) compared with the negligible effect observed in the CG (Cohen’s d = 0.036). Conclusion: Mirror Therapy coupled with theraputty hand activities was highly effective in improving hand function in stroke survivors. The combined intervention resulted in significant gains in motor performance, hand strength, coordination and functional hand use compared with conventional therapy alone. This approach is a safe, practical, cost-effective, and evidence-based rehabilitation strategy for enhancing hand function and promoting functional independence after stroke.
Stroke is a leading cause of mortality and long-term disability worldwide, resulting from an interruption of cerebral blood flow that causes neurological impairments affecting motor, sensory, cognitive, and functional abilities.¹,² Upper extremity (UE) dysfunction is among the most common consequences of stroke, affecting approximately 70–80% of survivors and significantly limiting independence in activities of daily living (ADLs).³,â´ Common impairments include muscle weakness, spasticity, reduced coordination, impaired dexterity, and decreased voluntary motor control, all of which adversely affect hand function.âµ Recovery of hand function is therefore a primary goal of stroke rehabilitation.¹
Motor recovery after stroke is largely dependent on neuroplasticity, the brain’s ability to reorganize neural pathways following injury.ⶠRehabilitation approaches that provide repetitive, task-specific practice and sensory feedback can facilitate cortical reorganization and functional recovery.âµ Mirror Therapy (MT) is a simple and cost-effective intervention that utilizes visual feedback by creating the illusion of movement in the affected limb through reflection of the unaffected limb. This visual illusion activates motor cortical regions and the mirror neuron system, thereby promoting motor recovery.â· Studies have demonstrated that MT improves upper limb motor function and hand coordination, particularly when combined with other rehabilitation interventions.â¸,â¹
Hand strengthening and dexterity training are also essential components of post-stroke rehabilitation. Therapeutic putty (Theraputty) is widely used in occupational therapy to improve grip strength, pinch strength, dexterity, and fine motor control through graded resistance exercises.¹â°,¹¹ Evidence suggests that resistance-based hand exercises enhance muscle activation and functional hand performance.¹² Recent rehabilitation research emphasizes that combining neural stimulation approaches with active motor training may produce superior outcomes compared to single-modality interventions.¹³ While MT facilitates neural activation and motor planning, Theraputty exercises improve hand strength and dexterity. However, limited evidence exists regarding the combined effect of MT and Theraputty activities specifically on hand function in individuals with stroke. Therefore, the present study aims to evaluate the effectiveness of Mirror Therapy combined with Theraputty activities on hand function among stroke survivors.
RELATED LITERATURE
Recent literature strongly supports the use of mirror therapy, hand exercise programs, theraputty-based rehabilitation, and combined therapeutic approaches for improving upper extremity recovery following stroke. Studies by Heike Thieme demonstrated that mirror therapy is a cost-effective and non-invasive intervention that enhances motor and functional outcomes, particularly when combined with task-oriented training, strengthening exercises, and conventional rehabilitation. Similarly, Nurulhuda Jaafar and Ita Daryanti Saragih reported improvements in hand function, dexterity, and coordination, especially during the subacute phase of stroke recovery, while Moo-Hyun Lee highlighted its role in improving grip strength, motor activation, and voluntary movement control through repetitive functional activities.
Research on hand exercise programs has also shown significant benefits for post-stroke upper extremity rehabilitation. Jeffrey A. Kleim and Theresa A. Jones emphasized that repetitive motor practice promotes neuroplasticity and motor relearning by strengthening neural pathways. Lijuan Xu et al. found that wearable hand orthosis training combined with conventional therapy improved upper extremity motor function and hand use in daily activities. Furthermore, Carolee J. Winstein reported that increased intensity of self-directed arm and hand exercises was associated with better Fugl-Meyer Assessment outcomes, while Janet H. Carr and Roberta B. Shepherd highlighted the importance of functional hand activities in facilitating the transfer of motor skills to everyday tasks.
Evidence also supports the use of theraputty as an effective rehabilitation tool for improving hand strength, dexterity, coordination, and functional performance after stroke. Virgil Mathiowetz emphasized the importance of resistive hand exercises in restoring upper extremity strength and manual function. Janet H. Carr and Roberta B. Shepherd noted that repetitive and task-specific hand activities promote motor relearning and functional recovery, whereas Stephen J. Page reported that repetitive strengthening exercises combined with active functional use significantly enhance motor performance and occupational functioning. Additionally, Jeffrey A. Kleim and Theresa A. Jones suggested that theraputty exercises provide valuable tactile and proprioceptive sensory input, which may improve sensory awareness and motor control.
Recent studies further indicate that combined rehabilitation approaches yield superior outcomes compared to isolated interventions. Jeffrey A. Kleim and Theresa A. Jones emphasized the effectiveness of multimodal rehabilitation strategies, while Alberto Saavedra-García reported improved functional arm performance when mirror therapy was combined with electrical stimulation. Likewise, Ita Daryanti Saragih demonstrated greater improvements in upper limb recovery, coordination, and daily functional performance when mirror therapy was integrated with conventional physiotherapy, strengthening exercises, and task-oriented activities. Lijuan Xu highlighted the benefits of wearable orthotic-assisted rehabilitation in enhancing repetitive movement training and motor recovery, and Peter Langhorne concluded that multimodal rehabilitation programs are particularly effective because they simultaneously address strength, coordination, sensory feedback, and functional task performance.
The Fugl-Meyer Assessment (FMA) remains one of the most widely used outcome measures in stroke rehabilitation research due to its reliability, objectivity, and sensitivity in detecting changes in motor recovery. David J. Gladstone emphasized its usefulness in tracking both minor and major improvements in upper extremity function over time. The assessment comprehensively evaluates reflex activity, movement synergies, voluntary control, wrist stability, grasp function, coordination, and movement speed. According to Janet Sanford, the FMA has been extensively used as a primary outcome measure in studies investigating mirror therapy, robotic-assisted rehabilitation, strengthening exercises, wearable orthoses, and task-oriented training. Furthermore, Carolee J. Winstein reported consistent improvements in FMA scores following interventions such as mirror therapy, repetitive hand exercises, and robotic rehabilitation, supporting its value in measuring treatment effectiveness.
AIM OF THE STUDY:
The aim of the study is to investigate the effectiveness of mirror therapy combined with theraputty hand activities on hand functions in stroke survivors.
OBJECTIVES OF THE STUDY:
MATERIALS AND METHODS
STUDY DESIGN
A randomized controlled trial (RCT) study design was adopted.
STUDY DURATION
4 week period of 6 sessions/week, 30 minutes per session
SAMPLE SIZE
The sample size for the research consisted of 60 participants diagnosed with Stroke.
SAMPLE TECHNIQUES
A convenient sampling technique was used for recruiting participants meeting the inclusion criteria for the study.
STUDY PLACE
The study was conducted at Chettinad Hospital and Research Institute, Chennai.
INCLUSION CRITERIA
EXCLUSION CRITERIA
TOOL USED
Fugl-Meyer Assesment
MATERIALS USED
INTERVENTION
In this study, a clinic-based MT protocol was used where participants were instructed to complete a 30-minute session using mirror (38 × 28 cm) placed in front of them at an angle of 70° to 80° at the trunk level. During the treatment, the injured UE was completely hidden behind the mirror, while the reflection of the good hand created the visual impression of normal movement in the injured hand. Participants were asked to observe the mirror reflection carefully while doing all movements simultaneously with both UE.
Then exercises and functional hand activities were performed simultaneously with both hands. Exercises included practicing ROM and strengthening fingers, wrist and forearm movements. Participants performed bilateral hand movements with theraputty. Functional hand activities included rolling putty from fingertips to wrist, squeezing putty into a fist, pressing thumb against each finger using putty, squeezing fingers together with putty between them, pulling fingers toward the center and squeezing cone-shaped putty, stretching putty around the fingers outward, pressing thumb down into cylindrical putty and curling each finger individually into the putty.

Figure 1: Rolling theraputty from fingertips to wrist

Figure 2: Squeezing putty into a fist
STUDY PROCEDURE
Ethical and institutional approvals were obtained prior to the study. Sixty stroke patients aged 45–65 years who met the inclusion criteria were recruited from the outpatient and inpatient departments of the selected hospital using convenience sampling. Written informed consent was obtained from all participants following an explanation of the study objectives and procedures. Baseline assessment was conducted using the Fugl-Meyer Assessment (FMA) to evaluate upper extremity motor function, hand function, coordination, and sensorimotor performance.
Participants were randomly allocated into Experimental Group (EG) and Control Group (CG) using opaque sealed envelopes, ensuring a single-blind study design. The EG received Mirror Therapy combined with theraputty hand activities for 30 minutes per session, six days per week, for four weeks (24 sessions). The intervention included warm-up exercises followed by mirror therapy and theraputty-based hand activities under researcher supervision. The CG received routine conventional therapy. Post-intervention assessment was conducted after four weeks using the FMA. Pre- and post-intervention data were statistically analyzed to determine the effectiveness of Mirror Therapy combined with theraputty activities on hand function in individuals with stroke.
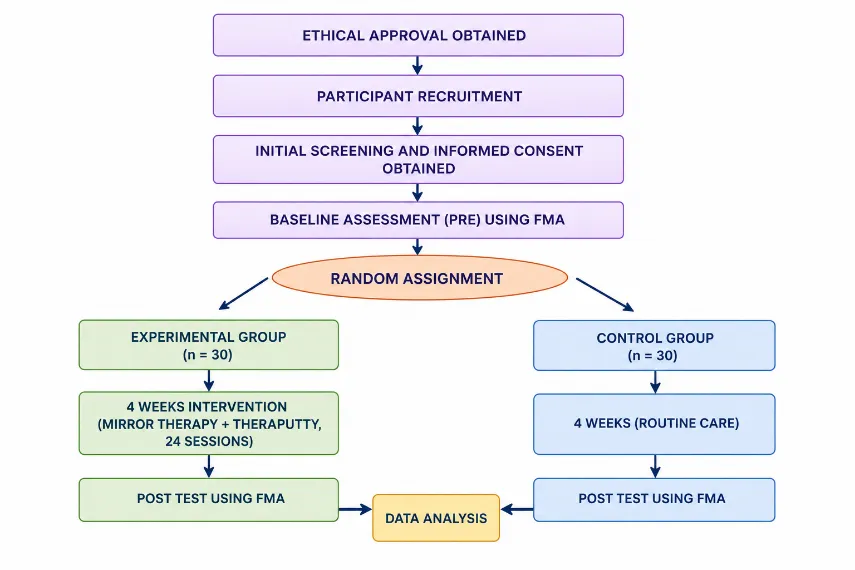
STUDY PROCEDURE FLOWCHART
DATA NALYSIS AND RESULTS
Data were analyzed using paired sample t-tests for within-group comparisons and independent sample t-tests for between-group comparisons. Cohen's d was calculated to determine intervention effect size.
|
Age(yrs) Variables |
Mean ± SD |
|
Total Population (n=60) |
54.68 ± 3.84 |
|
Experimental Group (n=30) |
54.96 ± 3.68 |
|
Control Group (n=30) |
54.40 ± 4.03 |
Table 1: Distribution of Demographical Age Variables among EG and CG
|
Age(yrs) Variables |
Mean ± SD |
|
Total Population (n=60) |
54.68 ± 3.84 |
|
Experimental Group (n=30) |
54.96 ± 3.68 |
|
Control Group (n=30) |
54.40 ± 4.03 |
Table 2: Distribution of Demographical Gender Variables among Experimental Group and Control Group
The Table 1 and Table 2 present the demographic characteristics of the study participants.A total of 60 stroke survivors were included in the study, with 30 participants each in the Experimental Group (EG) and Control Group (CG). The overall mean age was 54.68 ± 3.84 years, with comparable mean ages in the EG (54.96 ± 3.68 years) and CG (54.40 ± 4.03 years), indicating age homogeneity between the groups. Regarding gender distribution, the EG comprised 22 males (73.3%) and 8 females (26.7%), while the CG included 18 males (60.0%) and 12 females (40.0%). Although males predominated in both groups, the gender distribution was reasonably balanced, suggesting demographic comparability and minimizing the potential influence of age and gender on the study outcomes.
|
|
Mean ± SD |
t |
p |
|
|
Control Group |
Pre-test |
16.43 ± 3.45 |
- .47 |
0.63 |
|
Post-test |
16.57 ± 3.87 |
|||
Table 3: Paired t-test statistic for pre-test and post-test for CG using FMA
|
|
Mean ± SD |
t |
p |
|
|
Experimental Group |
Pre-test |
15.67 ± 3.65 |
-23.21 |
p < 0.01 |
|
Post-test |
27.96 ± 2.11 |
|||
Table 4: Paired t-test statistic for pre-test and post-test for EG using FMA
The Table 3 and Table 4 compare the pre-test and post-test FMA scores within the Control Group (CG) and Experimental Group (EG), respectively. As shown in Table 3, the CG demonstrated a negligible increase in mean FMA score from 16.43 ± 3.45 to 16.57 ± 3.87, with a paired t-value of -0.47 and a non-significant p-value of 0.63 (p > 0.05), indicating that conventional therapy alone did not result in significant improvement in hand function. In contrast, Table 4 shows that the EG exhibited a substantial increase in mean FMA score from 15.67 ± 3.65 to 27.97 ± 2.11 following the intervention. The paired t-test revealed a highly significant difference (t = -23.21, p < 0.01), demonstrating that mirror therapy combined with theraputty hand activities was highly effective in improving hand function among stroke survivors.
|
Group |
Mean ± SD |
t |
p |
|
Control Group |
16.43 ± 3.45 |
.83 |
.40 |
|
Experimental Group |
15.67 ± 3.65 |
|
|
Table 5: Analysis of Pre-test data between Control group and Experimental Group using FMA
The Table 5 compares pre-test FMA scores of EG & CG by independent sample t-test. Mean pre-test FMA score for CG was 16.43 ± 3.45 and EG was 15.67 ± 3.65. There was not much change in the two groups at the start, as pointed by the acquired t-value of 0.83 with a p-value of 0.40, which is statistically not noteworthy (p > 0.05). This suggests that the two groups were comparable at the beginning of the intervention.
|
Group |
Mean ± SD |
t |
p |
|
Control Group |
16.57 ± 3.87 |
-14.155 |
p < 0.01 |
|
Experimental Group |
27.96 ± 2.11 |
|
|
Table 6: Analysis of Post-test FMA scores between CG and EG
The Table 6 compares post-test FMA scores of CG and EG. The CG had a mean post-test score of 16.57 ± 3.87, whereas the EG showed a significantly greater score of 27.97 ± 2.11. The independent t-test value found was -14.155 showing a clear statistical proof of p-value of < 0.01. These findings suggest that EG achieved greater improvement in hand function compared to CG following intervention.
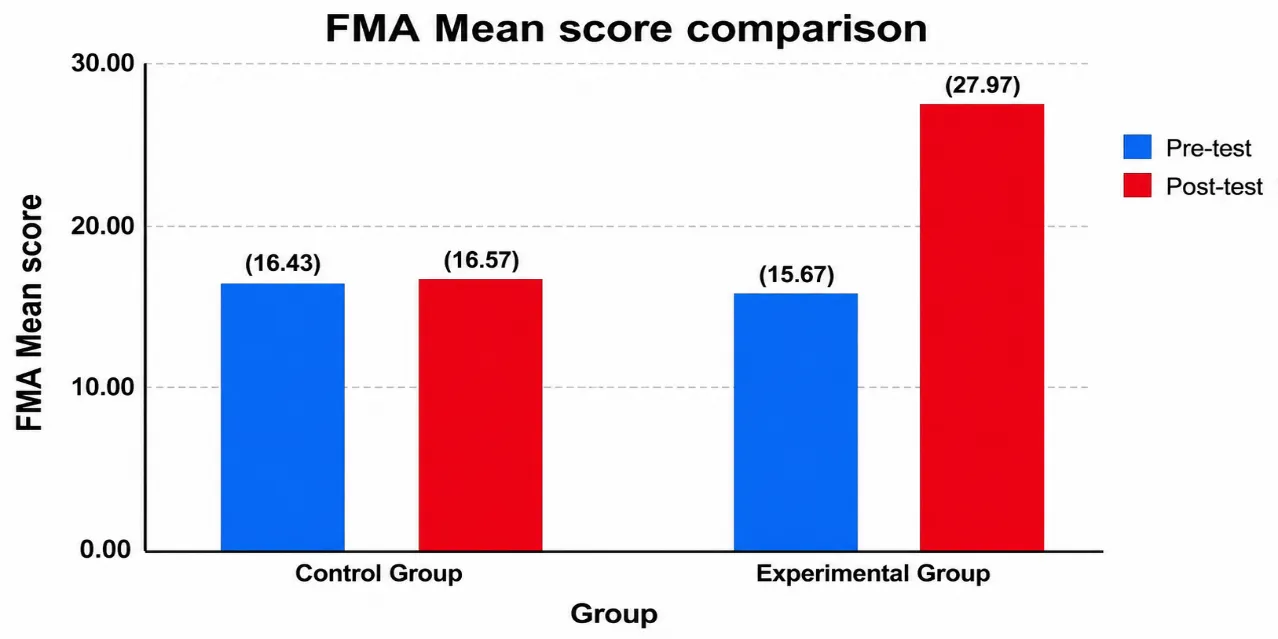
Figure 3: Pre-test and Post-test score comparison between CG and EG
Figure 3 presents the mean pre-test and post-test FMA scores of the Control Group (CG) and Experimental Group (EG). Both groups demonstrated comparable baseline hand function, with mean pre-test FMA scores of 16.43 ± 3.45 in the CG and 15.67 ± 3.65 in the EG. After four weeks, the CG showed only a minimal improvement (16.57 ± 3.87), whereas the EG exhibited a substantial increase in FMA scores (27.96 ± 2.11), reflecting an improvement of approximately 12.30 points. The figure clearly demonstrates that mirror therapy combined with theraputty hand activities resulted in significantly greater improvement in hand function compared to conventional therapy alone.
|
Time |
Group |
Cohen’s d |
Interpretation |
|
Pre-test to Post-test |
Control Group |
0.036 |
extremely small/negligible effect size. |
|
Pre-test to Post-test |
Experimental Group |
4.13 |
extremely large effect size. |
Table 7: Effect Size Analysis
Table 7 presents the effect size analysis using Cohen’s d to determine the magnitude of change in FMA scores within each group. The Control Group (CG) showed a negligible effect size (Cohen’s d = 0.036), reflecting minimal improvement in hand function following conventional therapy. In contrast, the Experimental Group (EG) demonstrated an extremely large effect size (Cohen’s d = 4.13), indicating a substantial and clinically meaningful improvement after the intervention. The marked difference in effect sizes between the groups highlights the strong therapeutic impact of mirror therapy combined with theraputty hand activities. These findings confirm the effectiveness of the intervention in significantly enhancing hand function among stroke survivors.
DISCUSSION
The present study evaluated the effectiveness of Mirror Therapy (MT) combined with Theraputty Hand Activities on hand function among stroke survivors. Both the Experimental Group (EG) and Control Group (CG) were comparable at baseline in terms of age, gender, and pre-test FMA scores, ensuring group homogeneity. The Control Group showed only minimal, non-significant improvement in hand function following conventional therapy, whereas the Experimental Group demonstrated a significant increase in FMA scores from 15.67 ± 3.65 to 27.97 ± 2.11 after four weeks of intervention (p < 0.01), with an extremely large effect size (Cohen’s d = 4.13). These findings indicate that MT combined with Theraputty activities was highly effective in enhancing hand function among stroke survivors.
The observed improvements are consistent with previous studies reporting the benefits of mirror therapy in promoting upper extremity motor recovery and functional performance after stroke.¹â´â»¹â· Mirror therapy facilitates motor relearning through visual feedback, activation of the mirror neuron system, and cortical reorganization, thereby enhancing neuroplasticity.¹â¶ In addition, Theraputty activities provide repetitive, task-specific practice and graded resistance training, which improve hand strength, dexterity, and motor control.¹â¸ The combination of neural stimulation through MT and active hand exercise through Theraputty likely produced synergistic effects, resulting in superior functional outcomes compared with conventional therapy alone. Overall, the findings support the use of MT combined with Theraputty Hand Activities as an effective rehabilitation strategy for improving hand function in individuals with stroke.¹â´â»¹â¹
CONCLUSION
Mirror therapy combined with theraputty hand activities is highly effective in improving hand function among stroke survivors. The intervention produced significant improvements in motor performance, dexterity, grip function, coordination, and overall functional use of the affected hand compared with conventional therapy alone. These findings support the integration of mirror therapy and theraputty-based exercises into occupational therapy and stroke rehabilitation programs.
LIMITATIONS
FUTURE RECOMMENDATIONS
ACKNOWLEDGEMENTS
The authors thank the participants, Chettinad School of Occupational Therapy, Chettinad Hospital and Research Institute, Chettinad Academy of Research and Education and the faculty of Chettinad School of Occupational Therapy for their support throughout the study.
REFERENCES


Kshitilipsha¹, Pankaj Kumar2*, Effectiveness Of Mirror Therapy Combined With Theraputty Hand Activities On Hand Functions In Stroke Survivors, Int. J. Sci. R. Tech., 2026, 3 (6), 1675-1683. https://doi.org/10.5281/zenodo.21033400
 10.5281/zenodo.21033400
10.5281/zenodo.21033400