
We use cookies to ensure our website works properly and to personalise your experience. Cookies policy
Department of Pharmaceutics, Gokhale Education Society's Sir M.S. Gosavi, college of Pharmaceutical Education and Research, Nashik, Maharashtra, India.
The past decade has witnessed an accelerating convergence of digital technology and clinical medicine, producing a new generation of therapeutic tools that operate not through molecules but through software, sensors, and algorithms. Digital therapeutics (DTx) represent one of the most consequential developments in this space: software-based interventions that deliver evidence-based therapeutic actions to prevent, manage, or treat medical disorders. Alongside these are broader digitalization efforts in pharmacy practice, spanning automated dispensing systems, telepharmacy, AI-assisted clinical decision support, and real-time remote patient monitoring. This review examines the landscape of digital therapy and pharmaceutical digitalization, tracing the conceptual distinctions between digital health, digital medicine, and digital therapeutics, and analyzing how each domain intersects with pharmacy practice. We discuss the evolution of smart medical devices including digital blood pressure monitors, smart glucometers, pulse oximeters, smart inhalers, wearable ECG monitors, and AI-based diagnostic systems. We also address persistent challenges including data privacy vulnerabilities, device cost barriers, regulatory fragmentation, and ethical questions surrounding AI-driven clinical decisions. The review concludes with a forward-looking analysis of the Internet of Medical Things (IoMT), digital pharmacists, predictive health analytics, and the role of smart hospitals in reshaping pharmaceutical care. The evidence gathered suggests that while digitalization in pharmacy holds genuine promise, its benefits are unevenly distributed and its risks are not yet fully managed.
1.1 Defining the Digital Health Ecosystem
Few areas of healthcare terminology are as tangled as the cluster of terms surrounding "digital health." The World Health Organization defines digital health broadly as "the field of knowledge and practice associated with the development and use of digital technologies to improve health," encompassing electronic health records, telemedicine, mobile health apps, and wearable sensors [1]. Within this broad umbrella, the term digital medicine refers more specifically to the use of software and hardware tools in clinical measurement, monitoring, and intervention, grounded in rigorous clinical evidence [2]. Digital therapeutics occupy a more specific niche still: they are software-based interventions, typically delivered via mobile applications or connected platforms, that produce a clinical or therapeutic outcome that has been validated in randomized controlled trials and is often subject to regulatory approval [3].
The distinction matters practically. A wellness app that encourages users to exercise is a digital health tool. A software program that uses cognitive behavioural therapy to treat insomnia and has received FDA de novo authorization is a digital therapeutic. The difference lies not in the medium but in the evidence standard, the regulatory pathway, and the nature of the therapeutic claim being made. Pharmacy practice is affected by all three tiers of this hierarchy, but the clinical and regulatory implications are quite different across them.
|
Parameter |
Digital Health |
Digital Medicine |
Digital Therapeutics (DTx) |
|
Definition |
Broad application of digital technologies in healthcare |
Evidence-based digital tools supporting clinical measurement and intervention |
Software-driven therapeutic interventions for disease prevention, management, or treatment |
|
Primary Objective |
Health promotion and wellness |
Clinical monitoring and decision support |
Direct therapeutic effect |
|
Clinical Validation |
Often limited |
Moderate to strong |
Strong clinical evidence required |
|
Regulatory Oversight |
Minimal or variable |
Moderate |
Strict regulatory review (FDA/CE) |
|
Examples |
Fitness apps, wellness trackers |
Smart ECG systems, CGM devices |
reSET®, Somryst®, EndeavorRx® |
|
End Users |
General public |
Clinicians and patients |
Prescribers and patients |
|
Therapeutic Claim |
Usually absent |
Supportive clinical claims |
Explicit therapeutic claims |
Table 1. Distinction Between Digital Health, Digital Medicine, and Digital Therapeutics
1.2 Why Pharmacy Needs to Pay Attention
Pharmacists have historically been the last clinical checkpoint before a drug reaches a patient. That role is being redefined. Digital therapeutics are, in a meaningful sense, non-drug treatments that pharmacists now encounter in clinical practice. Smart glucometers generate data that informs insulin dosing. Adherence reminder apps reduce missed doses in chronic disease management. Automated dispensing systems operate in pharmacies with minimal human oversight. Remote monitoring platforms alert pharmacists to deteriorating patient metrics. Each of these technologies intersects with core pharmacist competencies: medication therapy management, patient counselling, adverse event monitoring, and dose optimization.
The COVID-19 pandemic accelerated all of this considerably. Between March and April 2020, telehealth utilization in the United States increased by over 150-fold relative to pre-pandemic levels, and many regulatory flexibilities granted during the pandemic have since been retained or formalized [4]. Telepharmacy expanded access to medication counselling in underserved rural communities. AI-based diagnostic tools were deployed at scale with little time for careful validation. The pandemic forced rapid adoption, which also exposed gaps in readiness that this review addresses.
1.3 Scope of This Review
This review synthesizes evidence across the full spectrum of digital therapy and pharmaceutical digitalization, covering the development of smart medical devices, the regulatory landscape for FDA-cleared digital therapeutics, AI-assisted clinical systems, remote patient monitoring, and the ethical and logistical challenges that constrain real-world implementation. Both landmark foundational studies and recent literature from 2018 to 2024 are included. The intended audience is broad: pharmacy researchers, clinical pharmacists, medical informaticians, healthcare policy analysts, and students encountering this field for the first time.
2. Evolution of Digital Healthcare
2.1 From Paper to Pixels: A Brief Historical Trajectory
Traditional healthcare was organized around physical access. Patients came to clinics; clinicians examined them; prescriptions were written on paper and dispensed by hand. Information was local, often siloed within a single institution or a single physician's memory. The introduction of electronic health records in the 1990s began to shift this paradigm, but the shift was slow, expensive, and often implemented in ways that increased clinician burden rather than reducing it [5].
What changed the trajectory more fundamentally was not EHRs but smartphones. By 2015, there were more than 100,000 health-related applications available in major app stores, and adoption was growing rapidly across age groups and geographies [6]. The smartphone gave patients continuous access to health tools without requiring clinic visits. It also gave developers an inexpensive distribution platform that bypassed many traditional regulatory checkpoints, which created both the opportunity for innovation and the problem of unvalidated claims proliferating unchecked in consumer markets.
2.2 The Role of AI and Machine Learning
Artificial intelligence entered clinical medicine through several routes simultaneously. In diagnostic imaging, convolutional neural networks trained on large labelled datasets began matching or exceeding dermatologist performance in classifying skin lesions in controlled conditions by 2017 [7]. In clinical text analysis, natural language processing systems began extracting structured information from unstructured clinical notes at speeds and volumes no human team could match. In genomics, machine learning models identified prognostically meaningful patterns in multi-omic data that traditional statistical methods had failed to detect.
Topol's influential 2019 analysis in Nature Medicine argued that the most valuable application of AI in medicine is not replacing clinicians but freeing them from tasks that machines can perform routinely, creating time for the human dimensions of care that cannot be automated [8]. That argument remains contested. Critics note that AI performance benchmarks are typically measured in controlled retrospective datasets, and performance in real clinical deployments is frequently lower, sometimes dramatically so [9]. The gap between published benchmark accuracy and real-world clinical utility is one of the field's most under-discussed problems.
Machine learning in pharmacy has produced several practically useful applications. Algorithms trained on prescription databases can identify patients at high risk of non-adherence or adverse drug interactions before these events occur. Predictive models applied to pharmacy dispensing data have been used to flag opioid prescription patterns consistent with diversion. AI-assisted pharmacovigilance systems process post-marketing adverse event reports faster than manual review, though false negative rates remain a concern [10].
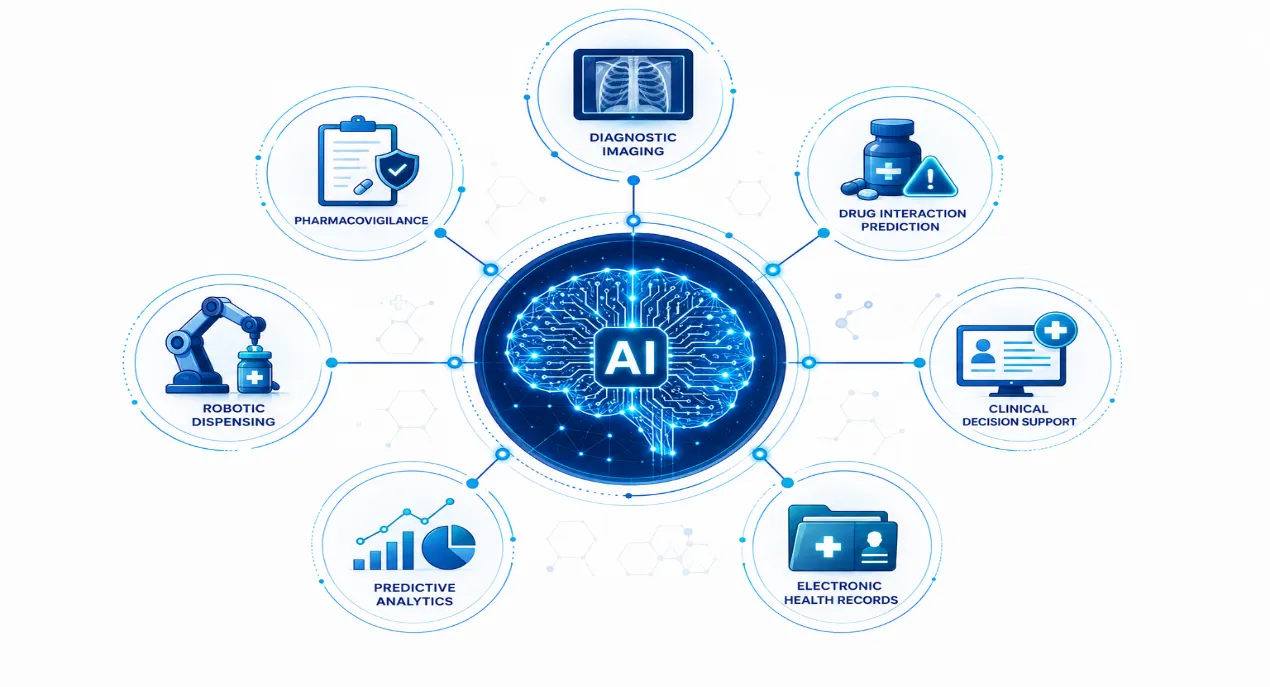
Figure 1. AI and Machine Learning Applications in Healthcare and Pharmacy
2.3 IoT and the Connected Patient
The Internet of Things connects physical devices to digital networks, enabling continuous data collection from sensors embedded in everyday objects. In healthcare, this translates into a patient who can be monitored around the clock without being physically present in a clinical setting. A patient with heart failure wears a patch that transmits continuous ECG data to a cloud platform where an algorithm flags rhythm abnormalities. A patient with poorly controlled diabetes checks blood glucose with a device that automatically logs the reading, syncs it with a nutrition app, and alerts the care team if glucose exceeds a defined threshold. These scenarios are not futuristic; they describe systems available and in use today [11].
The phrase Internet of Medical Things (IoMT) has emerged to describe this connected healthcare ecosystem, distinguishing medically relevant IoT applications from the broader consumer market. IoMT device adoption was estimated at over 300,000 devices globally by 2022, generating healthcare data volumes that present both analytical opportunity and infrastructure challenge [12].
2.4 COVID-19 as a Catalyst
The pandemic's impact on digital health adoption deserves separate attention because it was genuinely discontinuous rather than merely accelerating an existing trend. Dorsey and Topol, writing in The Lancet in 2020, argued that the pandemic "may have done more for telemedicine in one month than the prior ten years of gradual change" [4]. This is supported by utilization data: Medicare telehealth claims in the US increased from approximately 840,000 in the first quarter of 2019 to over 52 million in the second quarter of 2020 [13].
For pharmacy specifically, the pandemic years saw telepharmacy services expand into states and countries where they had previously faced regulatory barriers. Medication delivery services scaled rapidly. Remote medication reconciliation replaced in-person consultations for patients in lockdown. Automated dispensing systems became more attractive as infection control concerns limited face-to-face staff interactions. Not all of this innovation was well-planned, and not all of it persisted post-pandemic, but it created institutional familiarity with digital tools that has been difficult to reverse.
3. Digitalization in Therapeutics: Smart Devices and AI-Integrated Systems
3.1 Smart Medical Monitoring Devices
The term "smart" applied to medical devices is sometimes marketing language and sometimes a meaningful technical descriptor. A genuinely smart medical device does more than measure; it processes measurements, identifies patterns, communicates results, and ideally supports a clinical decision. The following devices represent the practical front line of digital therapy as it exists today.
Digital Blood Pressure Monitors. Modern connected sphygmomanometers go considerably beyond their oscillometric predecessors. Devices validated against the AAMI/ESH/ISO universal standard can now transmit readings automatically to smartphone apps, detect irregular heartbeats, and flag readings to care teams when values exceed predefined thresholds. A 2018 meta-analysis by Tucker et al. found that home blood pressure monitoring combined with clinical support produced significantly better blood pressure control compared with clinic-based monitoring alone, though the "clinical support" component was essential and the device alone was insufficient [14]. The lesson here is important: a connected device is not a treatment; it is a data source. What happens with that data determines the clinical value.
Smart Glucometers. Blood glucose monitoring has been a staple of diabetes management for decades, but the integration of continuous glucose monitoring (CGM) with algorithmic analysis has changed what is clinically possible. Abbott's FreeStyle Libre system and Dexterity's G6 (now G7) generate continuous interstitial glucose readings without fingerstick sampling, paired with trend data that allows patients and clinicians to anticipate glycaemic excursions rather than merely responding to them. A randomized trial published in The Lancet (Beck et al., 2017) found that CGM use in adults with type 1 diabetes on multiple daily injections reduced time in hypoglycaemia and improved glycaemic control compared with standard monitoring [15]. The clinical benefit, however, depends heavily on how patients and clinicians interpret and act on the trend data.
Pulse Oximeters. The pandemic brought consumer pulse oximeters into millions of homes. It also exposed a significant limitation: studies published in NEJM and JAMA Internal Medicine in 2021 and 2022 demonstrated that pulse oximetry systematically overestimates oxygen saturation in patients with darker skin tones, creating a documented disparity in COVID-19 clinical management [16]. This is a case where rapid digital adoption preceded adequate validation across diverse populations, with real clinical consequences. The lesson is not that pulse oximetry is useless; it is that device validation in demographically representative populations is not optional.
Smart Inhalers. Approximately 50% of patients with asthma or COPD use their inhalers incorrectly, and medication adherence in these conditions is chronically poor. Smart inhalers address this with sensors attached to or built into inhaler devices that detect each actuation, record the time and date, and transmit this data to smartphone apps. The Propeller Health platform, studied in a randomized trial by Merchant et al. (2018), demonstrated significant improvements in rescue inhaler-free days and adherence to controller medication in adults with asthma when the system included personalized feedback and environmental triggers data [17]. The key mechanism is feedback; the sensor alone without the behaviour-change component did not produce meaningful adherence improvement.
Wearable ECG Monitors. Single-lead ECG capture via wearable devices has been validated for atrial fibrillation detection in multiple populations. The Apple Heart Study (Perez et al., 2019) enrolled over 419,000 participants and found that irregular pulse notification followed by ECG patch confirmation had a positive predictive value of 0.84 for concurrent AF [18]. The study attracted both enthusiasm and criticism: it demonstrated that population-scale cardiac screening via consumer devices is technically feasible, but it also raised questions about what to do with a positive finding in an otherwise healthy, asymptomatic individual. Downstream cascade testing, anxiety, and over-medicalization are real risks of broad screening programs, even effective ones.
Wearable Fitness Trackers. Devices like the Fitbit family and Garmin health trackers collect step counts, sleep data, heart rate variability, skin temperature, and in some models, blood oxygen saturation. Their clinical utility is more contested than their commercial success suggests. A 2016 JAMA paper by Jakicic et al. found that adding a wearable fitness tracker to a behavioural weight loss intervention produced less weight loss than the intervention without the tracker, which was counterintuitive and highlighted the complexity of behaviour change [19]. More recent evidence suggests that wearables are most useful when embedded within structured clinical programs rather than used as standalone consumer tools.
|
Device Category |
Clinical Application |
Key Digital Features |
Representative Example |
Clinical Benefit |
|
Digital Blood Pressure Monitor |
Hypertension management |
Wireless BP transmission, trend analysis |
Omron Connect |
Improved BP monitoring |
|
Continuous Glucose Monitor (CGM) |
Diabetes management |
Real-time glucose tracking |
FreeStyle Libre |
Reduced hypoglycaemia |
|
Pulse Oximeter |
Oxygen saturation monitoring |
Smartphone connectivity |
NoninConnect |
Remote respiratory monitoring |
|
Smart Inhaler |
Asthma/COPD management |
Adherence tracking, reminders |
Propeller Health |
Improved inhaler adherence |
|
Wearable ECG Monitor |
Arrhythmia detection |
Continuous ECG monitoring |
Apple Watch ECG |
Early AF detection |
|
Fitness Tracker |
Lifestyle monitoring |
Activity and sleep tracking |
Fitbit Charge |
Increased physical activity |
Table 2. Smart Medical Devices and Their Clinical Applications
3.2 AI-Integrated Healthcare Systems
AI-Based Blood Group Detection. Manual ABO and Rh blood typing in resource-limited settings carries the risk of human error with potentially fatal consequences. Several research groups have developed image-based AI classifiers that analyse photographs of standard agglutination tests to determine blood group with high accuracy. A study by Bhattacharya et al. (2019) demonstrated that a convolutional neural network achieved 99.4% accuracy in blood group determination from smartphone-captured images, with potential applications in emergency settings and low-resource environments [20]. This application is promising precisely because it addresses a well-defined, high-stakes task where human error rates are documented and the AI operates on standardized visual inputs.
AI-Assisted Disease Diagnosis. Liang et al. (2019) published a study in Nature Medicine showing that an AI system trained on electronic health records of paediatric patients achieved diagnostic accuracy comparable to experienced clinicians across a range of conditions including respiratory diseases and gastrointestinal disorders [21]. Esteva et al.'s 2017 Nature paper on dermatologist-level skin cancer classification was the study that most prominently entered public consciousness [7], though subsequent real-world deployments have produced more mixed results. The pattern is consistent: AI diagnostic tools perform well in the datasets they are trained on and less predictably when moved to different hospital systems, demographic groups, or imaging equipment.
Robotic Drug Dispensing Systems. Automated dispensing robots in hospital and retail pharmacies reduce medication errors attributable to manual dispensing by eliminating transcription, picking, and labelling errors. The Omnicell and BD Pyxis systems are the most widely deployed examples in institutional settings. A systematic review by Chapuis et al. (2010) reported error rate reductions of 80-85% with unit-dose automated dispensing compared with traditional cart-fill systems [22]. More recent installations integrate barcode verification, weight checks, and camera-based visual confirmation. The remaining error modes are predominantly system configuration errors, where incorrect drugs are loaded into correct locations, rather than mechanical failures.
4. Types of Digital Therapeutics
4.1 Mobile Health Applications
The mHealth ecosystem is enormous and only partially mapped. As of 2023, the Google Play Store and Apple App Store together list over 350,000 health-related applications [23]. The clinical quality of this ecosystem is highly variable. Torous and colleagues have repeatedly documented that the gap between what patients need clinically and what app stores offer is substantial, and that evidence-based apps are consistently in the minority compared with commercially motivated wellness products [24].
The most clinically validated mobile applications address conditions where behavioural intervention is known to be effective and where patient engagement can be monitored and supported. Apps for diabetes self-management, smoking cessation, alcohol use disorder, and anxiety and depression have the strongest evidence bases. Less validated are applications for cancer symptom monitoring, pain management, and general wellness, where outcome measurement is harder and the risk of harm from replacing effective treatment with an ineffective app is real.
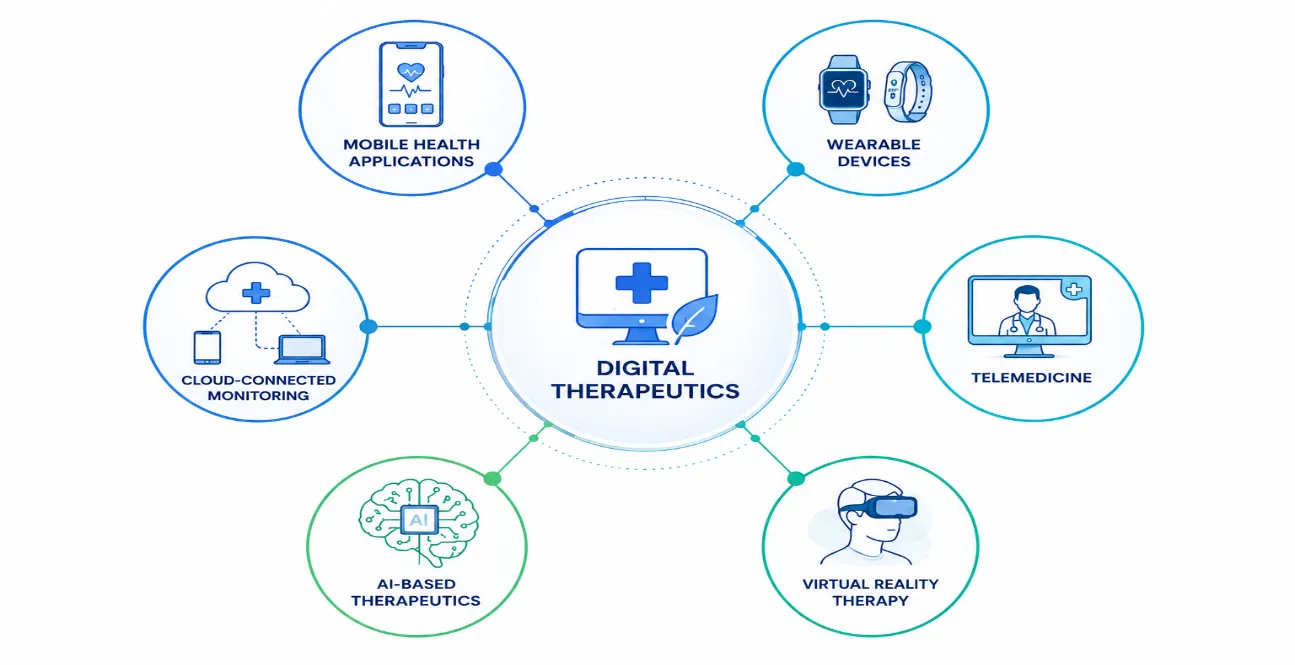
Figure 2. Classification of Digital Therapeutics
4.2 Wearable Devices
Wearable devices span a wide range of clinical sophistication. At one end are consumer fitness trackers with wellness features and limited clinical validation. At the other are prescription wearables like the EMBRACE watch (now Embrace2) for seizure detection, which received FDA approval in 2018 and generates quantified seizure data that previously required supervised video EEG in a clinical setting [25]. The clinical value of a wearable is proportional to the quality of the sensor, the validity of the algorithm interpreting sensor data, and the clinical use case to which the output is applied.
Patch-based biosensors represent an important subcategory. The BioSticker (BioIntelliSense), iRhythm Zio Patch, and Holter monitor successors like the CardioNet MCOT system generate continuous physiological data over days to weeks in ambulatory patients. These are not consumer devices; they require prescriptions, clinical ordering systems, and downstream clinical review workflows to translate data into decisions.
4.3 Telemedicine and Telepharmacy
Telemedicine encompasses synchronous video consultations, asynchronous image sharing, remote monitoring programs, and hybrid models that combine elements of each. Its application to pharmacy practice, telepharmacy, is particularly relevant in rural settings where access to clinical pharmacists is limited. A systematic review by Hayden et al. (2020) found that telepharmacy services maintained comparable rates of pharmacist intervention for potential drug-related problems relative to in-person services, while substantially expanding geographic access [26].
The limitations of telepharmacy are practical rather than conceptual. Physical examination of the patient is not possible; counselling on inhaler technique or injection administration requires video quality and patient dexterity that may not be present in all settings; and medication verification for complex regimens is more difficult at a distance. These constraints are real but not insurmountable, and the evidence suggests that telepharmacy's benefits in access expansion outweigh its limitations in most patient populations when implemented with appropriate clinical governance.
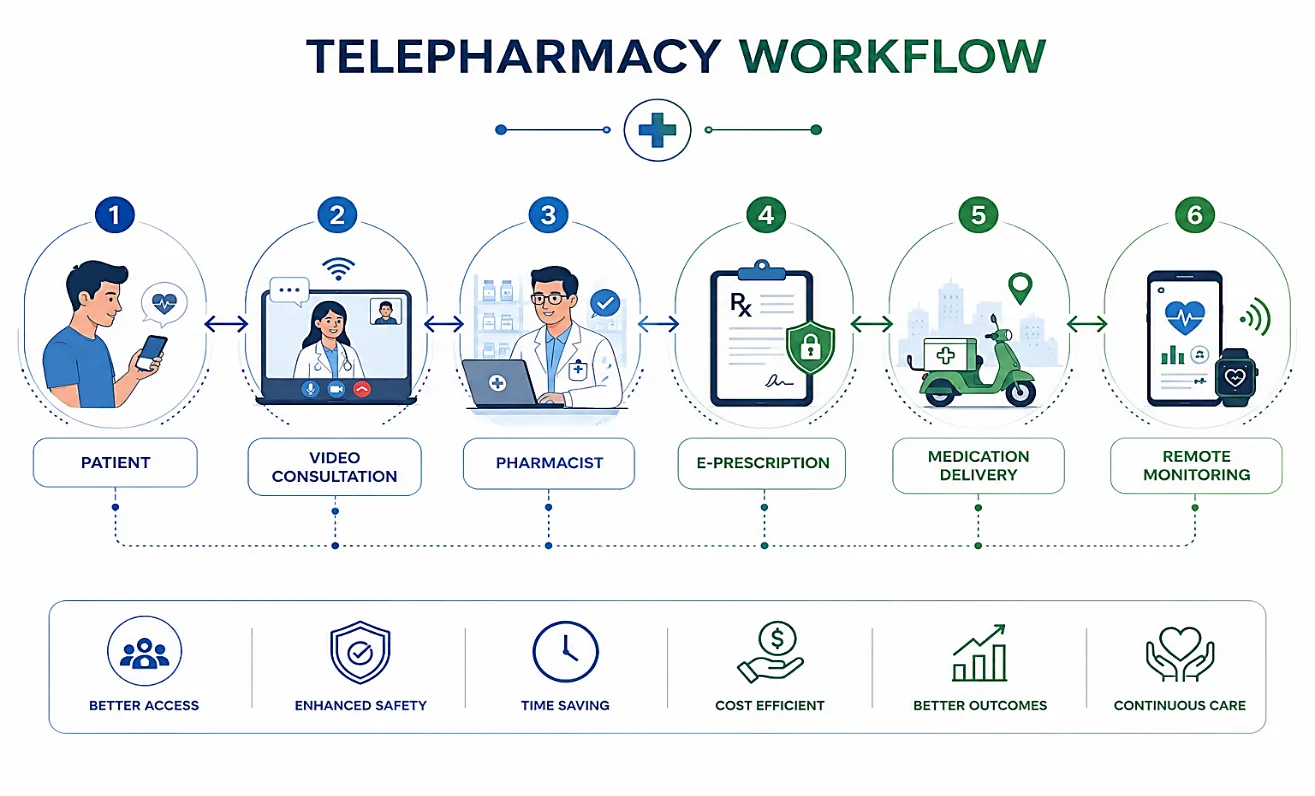
Figure 3. Telepharmacy Workflow Model
4.4 Virtual Reality Therapy
Virtual reality therapy uses immersive 3D environments to deliver therapeutic interventions for pain management, anxiety disorders, phobias, PTSD, and physical rehabilitation. The biological rationale for VR analgesia is reasonably well understood: cognitive distraction through immersive environments competes with pain signal processing in the anterior cingulate cortex and prefrontal regions, reducing perceived pain intensity without pharmacological intervention [27]. Hoffman et al.'s work on VR-based pain management in burn wound care demonstrated reductions in procedural pain that translated into reduced opioid consumption, a finding with obvious clinical relevance in the context of the opioid crisis [28].
VR for mental health is less mature but promising. Exposure therapy delivered through VR for specific phobias has demonstrated efficacy comparable to in vivo exposure in multiple controlled trials, with the practical advantages of controlled, repeatable exposure scenarios that are difficult or impossible to create in real-world settings [29]. The main barriers remain device cost, motion sickness in susceptible patients, and the need for clinical supervision, though lower-cost headsets like the Meta Quest series have reduced hardware barriers considerably.
4.5 AI-Based Therapeutic Systems
AI-based clinical decision support systems (CDSS) embedded in electronic health record platforms now alert prescribers to drug interactions, contraindications, and abnormal dosing ranges at the point of prescribing. These systems can prevent a subset of adverse drug events, though alert fatigue, the phenomenon by which clinicians override or ignore the majority of alerts because too many are clinically irrelevant, is a well-documented implementation problem [30]. Studies suggest that override rates for pharmacy CDSS alerts range from 49% to over 95% depending on the institution and alert type, which raises serious questions about whether the alerts are calibrated appropriately or whether they are generating noise rather than clinical signal.
More sophisticated AI-based therapeutic systems are being developed that use longitudinal patient data to adjust medication recommendations dynamically. Insulin dosing algorithms that incorporate CGM data, meal logs, exercise tracking, and historical glycaemic patterns are among the best-developed examples. Early versions of these algorithms require human pharmacist or physician oversight of recommendations before they are implemented; fully closed-loop insulin delivery systems (artificial pancreas systems) now exist in research and increasingly in commercial form, with several FDA-cleared systems available as of 2023 [31].
4.6 Cloud-Connected Monitoring Devices
Cloud connectivity enables something that was genuinely not possible before: longitudinal clinical monitoring at scale without institutional infrastructure. A patient discharged after a myocardial infarction can wear a patch that uploads continuous ECG data to a cloud platform where an algorithm identifies ventricular arrhythmias and notifies the care team within minutes. A patient with COPD can use a spirometer that uploads effort data after each test, allowing the care team to track lung function trends between clinic visits. The clinical logic is compelling. The implementation challenges are substantial: data security, alert fatigue in receiving care teams, liability for missed alerts, and the difficulty of incorporating continuous data streams into clinical workflows designed around episodic visits.
5. Applications in Pharmacy and Healthcare
5.1 Medication Management
Medication non-adherence is one of the most expensive problems in modern healthcare. The WHO estimates that in developed countries, only 50% of patients with chronic illnesses adhere to their prescribed treatment regimens, and the costs attributable to non-adherence in the US alone exceed $100 billion annually [32]. Digital adherence tools address this from several angles.
Adherence reminder apps use push notifications, scheduled alarms, and refill reminders to reduce missed doses. A systematic review by Anglada-Martinez et al. (2015) found that SMS-based and app-based adherence interventions produced modest but statistically significant improvements in adherence across HIV, hypertension, and diabetes populations, with effect sizes that were larger when the intervention included two-way communication rather than one-way reminders [33]. The two-way component matters because it allows the system to identify and respond to the reasons for non-adherence, which are heterogeneous and require individualized responses.
Smart pill dispensers, including devices like the Hero and MedMinder platforms, combine automated dispensing with electronic dose logging and family or caregiver alerts. These devices are most useful in elderly patients with polypharmacy and cognitive impairment, where the combination of complex regimens and reduced memory reliability creates a high-risk environment. The evidence base for smart dispensers in reducing clinical adverse events (hospitalizations, emergency visits) rather than surrogate adherence measures is thinner, and cost-effectiveness has not been convincingly demonstrated in controlled trials.
5.2 Chronic Disease Management
Diabetes. The integration of CGM data with insulin management has produced measurable clinical improvements across multiple studies. The DIAMOND trial (Beck et al., 2017) and the GOLD trial (Lind et al., 2017) both demonstrated HbA1c reductions and reduced hypoglycaemia with CGM use in type 1 diabetes on multiple daily injections [15, 34]. For type 2 diabetes on insulin, a Cochrane review (Poolsup et al., 2013, updated analyses since) found more modest benefits, likely because the behavioural component of responding to CGM data is harder to implement in less intensively managed patients. The digital tool is only as effective as the clinical system supporting its use.
Hypertension. Connected blood pressure devices linked to pharmacist or physician review programs have produced clinically meaningful reductions in systolic blood pressure in randomized trials. The TASMINH4 trial (McManus et al., 2018) demonstrated that self-monitoring with telemonitoring added to usual care produced a 7.7 mmHg greater reduction in systolic BP at 12 months compared with usual care alone [35]. This magnitude of reduction, if sustained, translates into meaningful cardiovascular event reduction at population scale. The pharmacist role in reviewing and responding to transmitted BP data was central to this benefit.
|
Disease Condition |
Digital Tool Used |
Clinical Purpose |
Reported Clinical Outcome |
|
Diabetes mellitus |
CGM systems |
Continuous glucose monitoring |
Improved HbA1c control |
|
Hypertension |
Telemonitoring systems |
Remote BP management |
Reduced systolic BP |
|
Asthma |
Smart inhalers |
Adherence improvement |
Reduced rescue inhaler use |
|
COPD |
Remote spirometry |
Lung function monitoring |
Early exacerbation detection |
|
Depression |
CBT mobile apps |
Mental health support |
Reduced depressive symptoms |
|
Insomnia |
Digital CBT platforms |
Sleep therapy |
Improved sleep quality |
Table 3. Applications of Digital Therapeutics in Chronic Diseases
5.3 Mental Health Applications
Digital mental health is one of the most active areas of DTx development and one of the most ethically complicated. Apps for anxiety, depression, insomnia, and substance use disorders are among the most downloaded health applications globally, but their clinical validation varies enormously. A systematic review by Linardon et al. (2020) found that cognitive behavioural therapy delivered through apps produced significant reductions in depression and anxiety symptoms in randomized controlled trials, with effect sizes in the moderate range (d = 0.3-0.5), which are meaningful but smaller than those produced by face-to-face CBT [36].
The concern is not only about efficacy but about appropriate use. Apps like Woebot and Wysa offer AI-driven conversational CBT at scale, and are used by millions of people who might otherwise have no access to psychological support. Whether they are reaching people who genuinely lack alternatives or replacing higher-quality face-to-face treatment for people who could access it is an empirical question that current data cannot fully answer. There is also a documented and disturbing phenomenon of "adverse effects" from mental health apps: a study by Lagan et al. (2021) found that several commercially available mental health apps contained content that was clinically inaccurate or potentially harmful, and that app store ratings were poorly correlated with clinical quality [37].
5.4 Remote Patient Monitoring in Clinical Pharmacy
Clinical pharmacists operating remote monitoring programs have demonstrated reductions in hospital readmissions for high-risk patients with heart failure, COPD, and post-surgical populations. The mechanism is intuitive: continuous physiological data allows earlier identification of decompensation, which enables earlier clinical intervention, which prevents hospitalizations. A retrospective analysis by Bhatt et al. (2021) found that patients enrolled in a pharmacist-managed remote monitoring program post-discharge had a 30-day readmission rate of 8.4% compared with 16.2% in a matched control group [38]. These numbers are striking and worth taking seriously, though the non-randomized design limits causal inference.
5.5 AI-Based Diagnostics in Pharmaceutical Care
Point-of-care AI diagnostic tools are beginning to enter pharmacy settings. AI-enabled smartphone devices that assess skin conditions, detect pill identification, analyse urine dipstick results, and process lateral flow test images for conditions including COVID-19, influenza, and strep throat are available and increasingly used. The pharmacy as a first point of contact for minor illness management is well-established in many healthcare systems, and AI-assisted triage tools could extend the diagnostic and therapeutic scope of pharmacy practice meaningfully. The regulatory framework for these tools is still catching up with their deployment.
6. Challenges and Limitations
6.1 Data Privacy and Cybersecurity
Health data is among the most sensitive personal information that exists, and health apps and devices generate it continuously. Grundy et al.'s 2019 BMJ analysis of 24 popular health apps found that 19 of them transmitted user data to 55 unique third parties, often without adequate disclosure [39]. Advertising technology companies, data brokers, and analytics firms receive health app data through software development kits embedded in the apps; most users have no meaningful awareness of this. The consequences can be severe: insurance discrimination based on inferred health status, employment discrimination based on mental health app use, and domestic abuse risks when tracking data is accessed by abusive partners.
Healthcare-specific cybersecurity vulnerabilities are also a serious concern. Ransomware attacks on hospital systems in 2020-2023 disrupted clinical operations, including pharmacy dispensing systems, at dozens of institutions, with documented harm to patients including delayed medication administration and cancelled procedures. The FDA has issued cybersecurity guidance for medical devices, and the 2023 Omnibus Spending Bill included requirements for FDA to establish cybersecurity standards for medical devices, but implementation and enforcement remain works in progress [40].
6.2 Cost and Access Equity
Smart medical devices are expensive. A current-generation CGM system costs $200-$400 per month in the US without insurance, which is prohibitive for the substantial portion of the diabetes population living in poverty. The patients most likely to benefit from digital monitoring are often those with the most poorly controlled disease, who are also the patients least able to afford the devices. Insurance coverage for DTx products is patchy and inconsistent: some commercial plans cover specific approved products; Medicare and Medicaid coverage remains limited and highly variable by state. This creates a situation where the benefits of digitalization accrue preferentially to more affluent, insured, and digitally literate populations, which risks exacerbating existing health disparities rather than reducing them.
6.3 Regulatory Fragmentation
The regulatory landscape for digital health products is genuinely complicated, and not consistently so across jurisdictions. The FDA's Digital Health Centre of Excellence has worked to create clearer pathways, including the Breakthrough Device Program for digital health tools and the Software as a Medical Device (SaMD) regulatory framework. But a product that achieves FDA De Novo authorization faces a separate regulatory process in the European Union through the EU Medical Device Regulation (EU MDR), which has different evidentiary and post-market surveillance requirements. The regulatory burden of achieving market authorization in multiple major markets is substantial enough to discourage smaller developers and create consolidation pressure in the industry [41].
Within the US, the regulatory distinctions between FDA-regulated prescription DTx products, FDA-exempted general wellness products, and the large gray zone in between (products making clinical claims without regulatory clearance) are not well understood by most prescribers, payers, or patients. The result is a market where validated products compete alongside unvalidated products in ways that are confusing for everyone involved.
6.4 Ethical Concerns in AI-Driven Care
AI systems in healthcare raise ethical questions that are not fully resolved. Algorithmic bias is the most documented: AI diagnostic systems trained predominantly on data from majority-group populations have demonstrated lower performance in minority populations for dermatological diagnosis, sepsis prediction, and pain assessment, to cite three well-documented examples [42]. The bias is not a product of malice but of the statistical learning process and the composition of training datasets, but its effects are clinical and real.
Questions of accountability are also unresolved. When an AI-assisted prescribing recommendation leads to a medication error, who is liable? The prescribing clinician who followed the recommendation? The system developer? The hospital that implemented it? Current legal frameworks were not designed for AI-mediated clinical decisions, and the literature on AI ethics in healthcare, while growing rapidly, has not converged on practical solutions to these questions [43].
7. Recent Advances
The period 2020-2024 has seen several developments worth specific mention. The emergence of large language model (LLM) applications in clinical decision support represents a qualitative change in what AI can do in text-heavy clinical tasks. GPT-4 passed the United States Medical Licensing Examination at or above the passing threshold in studies published in 2023, and early applications in patient triage, clinical documentation, and patient education are being evaluated [44]. The clinical deployment of LLMs raises new validation challenges because their outputs are generative rather than discriminative, making systematic accuracy evaluation harder than for classification-based systems.
Closed-loop insulin delivery systems achieved regulatory approval at a level of sophistication that approaches the autonomous. The Medtronic MiniMed 780G system and the Tandem Control-IQ system both automatically adjust basal insulin delivery in response to CGM readings and projected glucose trends, with options for auto-correction bolusing, bringing them close to the "artificial pancreas" concept that has been a research goal for decades [31]. Real-world data from registries and patient populations are beginning to validate the clinical outcomes promised in pivotal trials.
Wearable biosensors capable of continuous blood pressure monitoring without a cuff represent a potential inflection point in hypertension management. Several companies including Samsung, Valencell, and Aktiia have published validation studies, though as of 2023, no cuffless continuous BP device has achieved consistent accuracy across the physiological range needed for clinical management [45]. This is an area to watch; if a validated device reaches market at consumer price points, the management of hypertension in ambulatory populations could be substantially improved.
In pharmacy automation, robotic systems have extended beyond the traditional pill-counting applications to compound formulation verification, IV admixture preparation, and clinical trial medication management. BD's Rowa automation systems and Omnicell's newer installations incorporate machine learning-based image verification that can detect subtle product substitutions that barcode scanning alone would miss [46].
8. Future Perspectives
8.1 The Digital Pharmacist
The concept of the digital pharmacist, a clinically trained professional whose practice is mediated primarily through digital tools rather than physical dispensing, is already a reality in telepharmacy settings. The logical extension of this role involves pharmacists managing patient populations through continuous remote monitoring data, with AI systems handling routine medication adjustment recommendations within protocol-defined parameters, while the pharmacist focuses on patients whose data patterns fall outside protocol boundaries. This is a plausible and clinically well-grounded vision of pharmacy practice evolution, and it requires rethinking pharmacy education, licensure, and reimbursement structures simultaneously [47].
8.2 Predictive Healthcare Analytics
Machine learning models trained on longitudinal pharmacy data can predict which patients will have acute exacerbations before they occur, which patients are likely to discontinue their medications within 90 days, and which drug combinations carry interaction risks that standard rule-based CDSS systems miss. These predictive capabilities are most valuable when connected to proactive outreach workflows: the model identifies the at-risk patient; the system initiates a pharmacist call or automated message; the pharmacist intervenes; the exacerbation is prevented. Demonstrating these causal chains in prospective controlled studies is the methodological frontier, and several trials are ongoing [48].
8.3 Smart Hospitals and IoMT Integration
Smart hospital architectures integrate IoMT data from multiple device categories, patient location tracking, pharmacy automation systems, clinical decision support, and electronic health records into unified clinical intelligence platforms. The promise is a hospital that knows in real time which beds contain patients with deteriorating vital signs, which patients have missed medication doses, which operating rooms are at capacity, and which patients are ready for discharge. Realizing this promise requires both technical infrastructure and clinical workflow redesign, neither of which is trivial, and both of which need to happen simultaneously. Several hospital systems in Singapore, Israel, and Scandinavia have published early-implementation data suggesting that smart hospital investments reduce medication errors and early warning failure-to-rescue events, though long-term outcome data at scale are still accumulating [49].
8.4 Robotic Pharmacy Systems
The next generation of pharmacy robotics will likely move beyond dispensing into compounding, preparation verification, and bedside medication delivery using autonomous mobile robots. Intravenous admixture preparation, which currently involves manual compounding under sterile conditions, carries contamination risk that robotic preparation has been shown to reduce in multiple controlled studies [50]. Integrating pharmacy robotics with smart logistics, electronic medication administration records, and real-time patient demand prediction represents a convergence of technologies that could substantially reduce preventable medication errors in inpatient settings.
CONCLUSION
Digital therapy and the broader digitalization of pharmacy practice represent a genuine transformation in clinical medicine, not a hype cycle that will eventually deflate. The evidence supporting specific digital therapeutics, connected monitoring devices, AI-assisted clinical systems, and telepharmacy services is real and, in many cases, strong. FDA authorization pathways for prescription DTx products have created a regulatory framework, however imperfect, that distinguishes validated interventions from unvalidated wellness products.
At the same time, it is worth being clear-eyed about where the field is. Most digital health applications are deployed without rigorous clinical evaluation. Most patients using health apps are not using evidence-based products. Most health systems have not built the clinical workflows, data governance structures, or workforce training programs needed to make smart device data clinically useful rather than clinically burdensome. The gap between what is technically possible and what is routinely implemented is large.
The pharmacist's role in digital health is likely to expand substantially in the coming decade. Managing medication therapy through continuous monitoring data, using predictive analytics to identify at-risk patients before crises occur, supervising AI-assisted adherence programs, and practicing telepharmacy across geographic boundaries are all trajectories that current evidence supports and current clinical need motivates. Whether that expansion happens equitably, whether the patients most in need of digital health tools gain access to them, and whether the privacy and security concerns that currently shadow the field are addressed by regulation and industry practice will determine whether digital pharmacy fulfils its clinical potential or becomes another technology that benefits the already advantaged.
REFERENCES

Punam Shivaji Wavhule*, Emerging Digital Therapy And Digitalization In Pharmacy: A Comprehensive Review, Int. J. Sci. R. Tech., 2026, 3 (7), 608-623. https://doi.org/10.5281/zenodo.21427141
 10.5281/zenodo.21427141
10.5281/zenodo.21427141