
We use cookies to ensure our website works properly and to personalise your experience. Cookies policy
Haldia Institute of Health Sciences
Packed red blood cells (PRBCs) are the blood component most commonly used and have a critical role in the treatment of anemia, trauma, large-scale surgery and other haematological diseases. PRBCs are stored under refrigerated conditions to maintain adequate blood supply but as the storage time increases, a sequence of biochemical, metabolic and structural changes that are collectively referred to as storage lesions occurs. These changes can affect the viability, function and survival of erythrocytes following transfusion. The purpose of this review is to outline the state of the art knowledge regarding storage lesions and their effects on biochemical and haematological parameters of PRBCs. These biochemical changes include loss of adenosine triphosphate (ATP), 2,3-diphosphoglycerate (2,3-DPG), glucose utilization, lactate production, pH changes, potassium loss, sodium imbalance, oxidative stress and increased free hemoglobin release. Furthermore, significant haematological changes (morphology changes to red blood cells, fragility of the cell membrane, decrease in cell deformability, hemolysis, changes in red blood cell indices and formation of microparticles) gradually affect erythrocyte quality. Such changes to the stored blood can lead to decreased oxygen carrying capacity, trigger inflammatory response, contribute to hyperkalemia, and negatively impact transfusion effects, especially in the critically ill patient and those requiring massive transfusion. Current strategies include using better additive solutions, leukoreduction, optimizing storage conditions, using antioxidant based preservation, and promising new technologies to reduce the occurrence of storage lesions and improve blood quality. Further studies on new markers and improved preservation methods are key to further optimizing PRBC storage, ensuring transfusion safety and clinical outcomes.
In modern medicine, blood transfusions are an essential part of treating a wide range of medical and surgical issues. It is used to treat severe anemia, postpartum hemorrhage, postoperative blood loss, and acute trauma-related hemorrhage [1]. Moreover, patients suffering from hematological disorders, malignancies and chronic diseases are often in need of blood transfusions over and over again to achieve optimal oxygen carrying capacity and clinical outcomes. The safety, availability, and efficacy of blood products have significantly advanced due to the evolution of blood banking and transfusion medicine, which is why transfusion treatment is an essential part of patient care. The most common type of blood product is packed red blood cells, or PRBCs. PRBCs are produced by extracting plasma from whole blood, yielding a concentrated source of erythrocytes with reduced plasma content [2]. By increasing the blood's oxygen carrying capacity, they hope to re-open or restore oxygen transport to tissues. In humans, PRBC transfusion is routinely indicated in patients with symptomatic anemia, acute blood loss, perioperative blood loss, intensive care requirements, and in certain chronic hematological diseases. It is important to keep the structural integrity and functional quality of the PRBCs during the storage period, as the use of these products in clinical practice is widespread [3]. “The blood storage is one of the basic knowledge of transfusion medicine and is the activity carried out in blood banks to ensure that blood components are available whenever needed in emergency or routine clinical practice. Blood donation and transfusion are normally separated by a long period of time, and stored blood should maintain the viability and function of the red blood cells until their use in transfusion. Preservative and additive solutions like citrate phosphate dextrose adenine (CPDA-1) or saline adenine glucose mannitol (SAGM) are typically used to store packed red blood cells at 2-6°C [4]. PRBCs can be stored for up to 35-42 days depending on the type of preservative solution used”. Maintaining the quality of RBC during this period of storage is of paramount importance as the efficacy of transfusion of blood relies on the survival of, deformability and the oxygen delivery capacity of erythrocytes. Appropriate storage conditions will help to minimise cellular deterioration, prevent haemolysis and keep stored blood safe and effective for transfusion. Red blood cells, even under the best storage conditions, still make biochemical, metabolic, structural and functional changes, which are grouped under the terms storage lesions [5]. These changes start soon after the blood has been taken and during storage. The most common causes of storage lesions are decreased cellular metabolism, loss of energy reserves, oxidative stress, membrane damage, and changes in ion transport mechanisms. Storage lesions cause a decrease in adenosine triphosphate , 2,3 diphosphoglycerate, build up of lactate, lowering of pH, leakage of potassium into the storage medium, increase in oxidative damage, membrane vesiculation and morphological transformation of erythrocytes. These changes can affect the deformability of red blood cells, shorten the post-transfusion life, and decrease the amount of oxygen delivered to tissues [6]. It is important to have a thorough knowledge of storage lesions to evaluate and enhance the blood preservation strategy and improve transfusion outcomes. Many studies have shown that there are significant biochemical and hematological changes as a result of the length of storage, which can have an impact on the quality and performance of PRBCs for transfusion. Many of these changes are deemed tolerable for existing storage protocols, but the clinical implications of these changes are still under investigation, especially with regards to critically ill patients, neonates, trauma patients, and patients receiving massive transfusion [7]. A summary of current knowledge about storage induced changes may help researchers, clinicians and transfusion specialists to understand the factors that impact blood quality, relate laboratory data to the changes in the blood, and discover better methods of blood storage. This information is also helpful in the continual improvement of transfusion safety and care of patients. The current scientific literature on packed red blood cell (pRBC) storage lesions, including biochemical and haematological changes, will be summarized in this review. It also describes the processes that lead to these changes, the importance of these changes from a therapeutic perspective, and current initiatives to mitigate storage-induced alterations that impact the efficacy and quality of PRBCs.
2. BIOLOGY OF RED BLOOD CELLS
2.1 Structure and Function of Red Blood Cells
In order for the body to exhale carbon dioxide, it relies on specialized cells called erythrocytes, also known as red blood cells (RBCs), are responsible for carrying oxygen throughout the body after it leaves the lungs. Human RBCs are biconcave, disc-shaped cells that have a lifespan of around 120 days in the bloodstream, and an average diameter of around 7–8 μm. The mature erythrocytes do not contain any nucleus, mitochondria, endoplasmic reticulum or ribosomes. The structure has been uniquely designed to provide space maximisation for hemoglobin, an iron containing protein, for binding and transport of oxygen. Because of their biconcave form, The ability of red blood cells (RBCs) to squirm into tiny capillaries and their large surface area to volume ratio makes them ideal for gas exchange. Red blood cells (erythrocytes) help carry oxygen throughout the body; they also participate in the transport of carbon dioxide, blood buffering and maintain normal blood rheology. These structural and functional features are critical to provide sufficient tissue oxygenation and keep the physiological homeostasis [8].
2.2 RBC Metabolism
Red blood cells are metabolically active during their entire life even though they have no mitochondria. They can only produce ATP by anaerobic glycolysis and therefore glucose is the main substrate they use for ATP production. The Embden–Meyerhof glycolytic pathway is responsible for metabolizing about 90–95% of the glucose in the cell, generating ATP which is used to run ion pumps in the membranes, maintain cell shape, and maintain the integrity of the membranes. Low ATP concentration leads to decreased membrane function, decreased cellular deformability and increased hemolysis [9]. The production of nicotinamide adenine dinucleotide phosphate through the pentose phosphate pathway requires less glucose. The importance of NADPH in protecting erythrocytes from oxidative stress is evident, because it keeps glutathione in its reduced state and thus helps to prevent oxidative damage to the lipids and proteins of the cell membranes. The glycolytic intermediate 2,3 diphosphoglycerate, or 2,3-DPG, influences hemoglobin's oxygen affinity. Hemoglobin is able to deliver oxygen to the periphery when levels of 2,3-DPG in the cell are high. The concentration of 2,3-DPG decreases gradually during blood storage and causes hemoglobin to bind oxygen more tightly, causing a brief decrease in the delivery of oxygen after blood transfusion [10] .
2.3 Characteristics Important for Blood Storage
The safety and efficacy of preserved packed red blood cells depend on a number of critical cell characteristics. The deformability of the membrane is crucial to erythrocytes passing through the microcirculation without mechanical damage. Reduced post-transfusion cell survival and increased rigidity during storage are associated with loss of deformability. The other important property is the efficient delivery of oxygen carried by erythrocytes which requires proper functioning of hemoglobin and sufficient levels of intracellular ATP and 2,3-DPG. Depleted by the storage process, these metabolites have a negative effect on the delivery of oxygen to tissues soon after transfusion. Lastly, the survival of the cells depends on the loss of damage to the membrane and the maintenance of ionic balance and metabolic activity during the storage period. A biochemical and structural progressive deterioration may lead to hemolysis, membrane vesiculation, and impaired in vivo survival of transfused RBCs. Hence, maintaining these qualities is essential for the safety, effectiveness and clinical success of packed red blood cell transfusion [11].
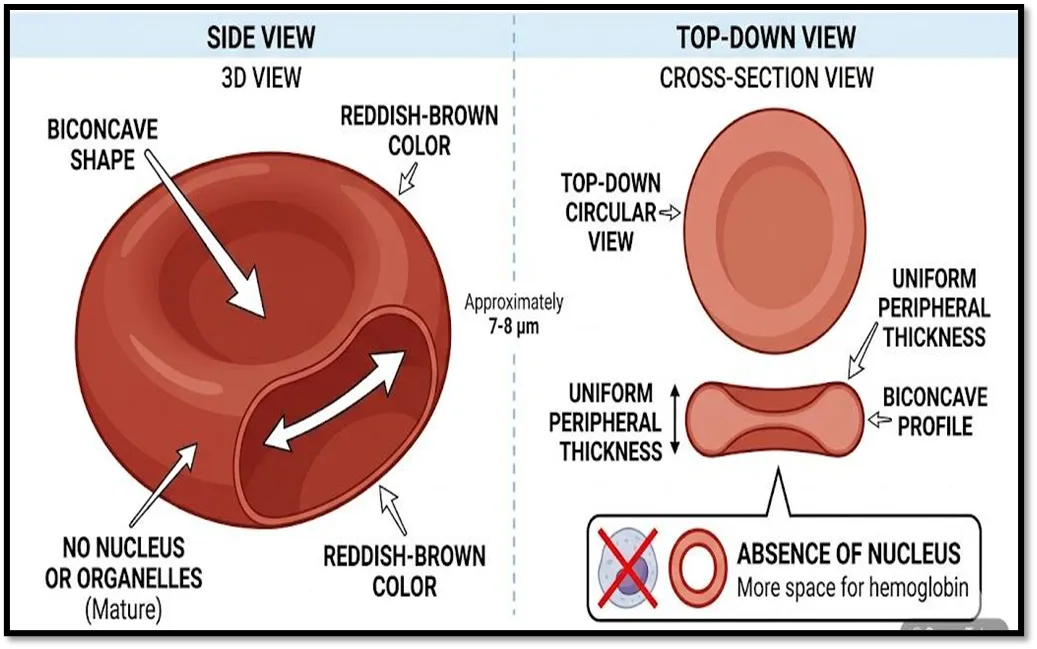
Figure 1. Structure of a normal red blood cell showing its biconcave shape, hemoglobin-rich cytoplasm, and major physiological functions.
|
Characteristic |
Physiological Role in Normal RBCs |
Importance During Blood Storage |
Changes During Prolonged Storage |
References |
|
Biconcave shape |
Provides a excellent gas exchange efficiency due to large surface area relative to volume and allows passage through narrow capillaries. |
Maintains deformability and facilitates post-transfusion microcirculation. |
Progressive transformation into echinocytes and spherocytes, reducing flexibility. |
[12] |
|
Hemoglobin (Hb) |
Glues oxygen from the blood to the body's tissues and returns carbon dioxide to the lungs. |
Determines the oxygen-carrying capacity of stored PRBCs. |
Oxygen-release efficiency decreases due to depletion of intracellular 2,3-DPG. |
[13] |
|
Cell membrane |
Preserves cell shape, regulates ion exchange, and protects intracellular contents. |
Essential for maintaining membrane integrity and minimizing hemolysis during storage. |
Membrane lipid and protein oxidation increase fragility, vesiculation, and hemolysis. |
[14] |
|
ATP |
Supplies energy for membrane ion pumps, maintains membrane integrity, and preserves cellular deformability. |
Supports RBC viability and prolongs post-transfusion survival. |
ATP levels progressively decline, leading to impaired membrane function and increased cell rigidity. |
[15] |
|
2,3-Diphosphoglycerate (2,3-DPG) |
Regulates hemoglobin–oxygen affinity and promotes oxygen release to peripheral tissues. |
Ensures efficient oxygen delivery after transfusion. |
Concentration decreases rapidly during storage, temporarily impairing oxygen unloading. |
[16] |
|
Ion homeostasis |
Maintains intracellular potassium and sodium balance through ATP-dependent ion pumps. |
Prevents osmotic imbalance and cellular swelling. |
Potassium leaks into the storage medium, while sodium accumulates within the cells. |
[17] |
|
Antioxidant defense system |
Protects RBCs from oxidative damage through glutathione, catalase, and superoxide dismutase. |
Preserves membrane proteins, lipids, and hemoglobin stability. |
Antioxidant capacity decreases, resulting in oxidative stress and membrane damage. |
[18] |
|
Cell survival |
Ensures an average lifespan of approximately 120 days in circulation. |
Maximizes recovery and survival of transfused erythrocytes. |
Progressive biochemical and structural deterioration shortens post-transfusion survival. |
[19] |
Table 1. Structural and Functional Characteristics of Red Blood Cells and Their Importance During Blood Storage
3. Packed Red Blood Cells and Storage Conditions
3.1 Preparation of Packed Red Blood Cells (PRBCs)
Among the several blood components that are manufactured from healthy donors, packed red blood cells are among the most frequently transfused. Following donation, centrifugation separates the blood into its component parts: red blood cells, plasma, and buffy coat. The majority of the plasma is removed and a concentrated suspension of erythrocytes is formed, called PRBCs. Some blood banks leukoreduce prior to storage while others do it after storage, either way it is done in the blood bank, it helps to reduce the white blood cell count, hence the chances of febrile non-hemolytic transfusion reaction, alloimmunization and the accumulation of inflammatory mediators in storage. The prepared PRBC then are combined with preservative or additive solutions and preserved under controlled conditions until they are given as transfusion [20].
3.2 Storage Solutions
The viability, metabolism and functional integrity the effectiveness of the preservation solution used to keep red blood cells is crucial. These solutions give nutrients, help sustain osmotic equilibrium and limit metabolic degradation during storage. Citrate phosphate dextrose adenine is a popular anticoagulant-preservative solutio. Citrate binds up calcium ions to prevent coagulation, phosphate buffers, dextrose provides an energy source for glycolysis and adenine helps to produce ATP. The recommended storage temperature for PRBCs preserved in CPDA-1 is 20°C, and the storage period is usually up to 35 days. After the plasma has been removed, Saline Adenine Glucose Mannitol (SAGM) is often used to further improve red blood cell preservation. Glucose and adenine keep the erythrocyte membrane stabilized and help to minimize hemolysis during storage, so that PRBCs can be stored for up to 42 days. Other additive solutions such as AS-1, AS-3 and AS-5 have also been created to support the survival of red blood cells by supplying them with further nutrients and reducing biochemical deterioration during extended storage [21].
3.3 Storage Conditions
The maintenance of the quality and safety of PRBCs depends on proper storage conditions. The international guidelines for blood banking suggest to store PRBC at temperature of 2–6°C in a blood bank refrigerator with temperature control. This temperature range is effective in reducing cellular metabolism, bacterial growth, and maintaining red blood cell viability. Depending on the preservative solution, the maximum storage time is one month. The storage period for PRBCs in CPDA-1 is usually 35 days and for PRBCs preserved with additive solutions like SAGM is 42 days. Blood banks are keeping a constant watch on the refrigerator temperature, inventory control and quality control parameters during storage, to ensure that blood products comply with the transfusion standards and to keep the products safe [22].
3.4 Factors Affecting Storage Quality
PRBCs have several factors that affect their quality in storage. The most important factor is storage duration and over time biochemical, metabolic and structural changes can occur, which are grouped together as storage lesions. While temperatures are lower, cellular metabolism is affected, but inappropriate temperature fluctuations can cause hemolysis and affect red blood cell integrity. Leukoreduction can reduce the levels of leukocytes derived cytokines, enzymes and reactive oxygen species which can cause inflammatory responses and oxidative damage, thereby improving the storage quality. On the other hand, certain patients may receive irradiation so that graft-versus-host disease, which can occur after blood transfusions, might be lessened, which can result in higher fragility, potassium loss, and hemolysis, especially in long storage. Thus, it is important to follow standard processing and storage procedures to maintain the quality of PRBCs and maximize the benefits of blood transfusion [23].
|
Storage Solution |
Major Components |
Primary Function |
Maximum Storage Period |
|
CPDA-1 (Citrate Phosphate Dextrose Adenine) |
Citrate, phosphate, dextrose, adenine |
Prevents coagulation, maintains pH, supplies glucose, supports ATP synthesis |
35 days |
|
SAGM (Saline Adenine Glucose Mannitol) |
Saline, adenine, glucose, mannitol |
Preserves membrane integrity, reduces hemolysis, prolongs RBC survival |
42 days |
|
AS-1 (Adsol) |
Saline, adenine, glucose, mannitol |
Improves RBC viability and minimizes storage lesions |
42 days |
|
AS-3 (Nutricel) |
Saline, adenine, glucose, citrate, phosphate |
Maintains ATP levels and supports RBC metabolism |
42 days |
|
AS-5 (Optisol) |
Saline, adenine, glucose, mannitol |
Enhances membrane stability and reduces hemolysis |
42 days |
Table 2. Common preservative and additive solutions used for the storage of packed red blood cells (PRBCs), their principal components, primary functions, and recommended maximum storage duration [24].

Fig 2: Flow diagram of PRBC preparation and storage process.
4. Mechanisms of Storage Lesions
4.1 Definition of Storage Lesions
Prolonged storage causes a group of alterations in packed red blood cells called "storage lesions." Any number of biochemical, metabolic, structural, or functional changes could be at work here. The erythrocytes' shelf life is prolonged by the low temperature, but their gradual degeneration is still there. These changes start soon after the blood is drawn and during the entire storage period will impact on red blood cell viability, integrity of the cell membrane, deformability and oxygen delivery capacity. Storage lesions are typically more severe with longer storage time and could affect the quality or clinical utility individuals receiving blood transfusions, particularly those in critical care and those undergoing extensive transfusions [25].
4.2 Cellular Mechanisms
Progressive metabolic abnormalities of erythrocytes is the main cause of development of storage lesions. There are no mitochondria or nuclei in mature red blood cells, which means that they produce all of their energy via anaerobic glycolysis. As the available amount of glucose diminishes and enzyme activity decreases during refrigerated storage, the glycolytic activity progressively decreases. As a result, the metabolic rate of stored erythrocytes becomes progressively diminished. Loss of metabolism is one of the most important effects resulting in a loss of adenosine triphosphate . ATP is crucial for maintaining the asymmetry of membrane phospholipids, for regulating the sodium–potassium ATPase pumps, for maintaining membrane flexibility, and for preventing premature destruction of cells. When ATP is reduced, the integrity of the cell membrane is compromised, the ion balance in the cell is disrupted, and erythrocytes gradually become non-biconcave. ATP depletion is also responsible for increased rigidity of the membrane, increased hemolysis, and decreased post-transfusion survival. Another major contributor to storage lesions is oxidative stress. Reactive oxygen species (ROS) are always formed during storage through auto-oxidation of hemoglobin, and other oxidative reactions. The antioxidant defence system of erythrocytes decreases during storage, leading to the progressive accumulation of ROS in erythrocytes. This oxidative imbalance leads to the damage of membrane lipids, cytoskeletal proteins and hemoglobin, which leads to impaired cellular function and increased sensitivity to hemolysis. Both ATP depletion and oxidative stress contribute to the advancement of storage deterioration [26].
4.3 Membrane Alterations
The membrane of the erythrocytes is very sensitive to oxidative damage especially in the prolonged storage. Lipid peroxidation is one of the earliest changes in membrane that is caused by the attack of membrane phospholipids by being around when ROS are present leads to reduced stability and increased permeability of the membrane. Lipid peroxidation causes loss of structural integrity and leakage of intracellular potassium and other intracellular constituents into the storage medium. Protein oxidation also causes damage to membrane and cytoskeletal proteins. Oxidative modifications of structural proteins, such as spectrin, ankyrin, band 3 protein, and actin are responsible for changes in membrane architecture. These modifications affect interactions between the membrane and the cytoskeleton, thus decreasing the mechanical stability and fragility of the membrane. As the damage to the membrane increases, the erythrocytes get progressively less biconcave and become less flexible. The decrease in cell deformability decreases their ability to pass through the narrow capillaries and splenic sinusoids, thus reducing their viability after transfusion. Morphological changes of discocytes to echinocytes and finally to spherocytes is a characteristic feature of the advanced storage lesion [27].
4.4 Microvesicle Formation
A key aspect of storage lesions is the generation of microvesicles from the red blood cell (RBC) population. When erythrocytes sustain oxidative damage to their membranes, it triggers the release of these extracellular vesicles, destruction of the cytoskeletal elements and loss of membrane phospholipids. The vesiculation of microvesicles is a process of protection which eliminates damaged membrane components; however, when there is too much vesiculation, it will progressively decrease the areas of the membranes and add to the fragility of the erythrocytes. Microvesicles can be stored and contain phospholipids, membrane proteins, hemoglobin and bioactive molecules that could induce inflammatory responses, endothelial activation and coagulation after transfusion. There is growing evidence to indicate that there is a relationship between higher concentrations of micro vesicles with prolonged storage and other adverse transfusion-related outcomes [28].
4.5 Progressive Changes During Storage
Lesions that form over time while stored in a refrigerator are known as storage lesions. Decreases in metabolic activity and 2,3-Diphosphoglycerate (2,3-DPG) levels are observed during the initial days of storage. Continued storage results in further deterioration of erythrocyte metabolism due to glucose consumption, lactate production and progressive acidification of the storage medium. At the same time, there is a potassium leakage from the cells, oxidative stress is enhanced, structural modifications of membrane proteins, and an acceleration of the production of micro vesicles. At the end of storage, red blood cells are extremely rigid, fragile, morphologically altered and hemolyse quickly. These biochemical and structural changes decrease functional properties of stored PRBCs and could affect the efficacy of PRBC transfusion. Therefore, knowledge of the mechanisms of storage lesion is important to improve storage protocols and to optimize transfusion outcomes [29].
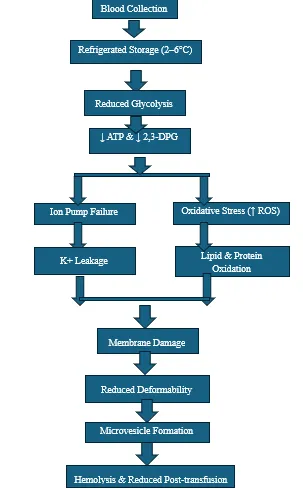
Fig 3: Mechanisms Involved in the Development of Storage Lesions in Packed Red Blood Cells During Refrigerated Storage.
|
Mechanism |
Underlying Process |
Effect on PRBCs |
Clinical Significance |
References |
|
Reduced metabolism |
Decline in glycolytic activity during refrigerated storage |
Reduced energy production |
Initiates storage lesion development |
[30] |
|
ATP depletion |
Continuous ATP consumption with limited regeneration |
Membrane instability, impaired ion transport, reduced deformability |
Decreased RBC survival after transfusion |
[31] |
|
Oxidative stress |
Excess production of reactive oxygen species (ROS) |
Oxidative damage to lipids, proteins, and hemoglobin |
Increased hemolysis and cellular dysfunction |
[32] |
|
Lipid peroxidation |
Oxidation of membrane phospholipids |
Increased membrane permeability and fragility |
Promotes potassium leakage and hemolysis |
[33] |
|
Protein oxidation |
Oxidative modification of membrane and cytoskeletal proteins |
Loss of membrane integrity and altered cell shape |
Reduced mechanical stability |
[34] |
|
Reduced deformability |
Membrane and cytoskeletal damage |
Impaired passage through microvasculature |
Reduced post-transfusion recovery |
[35] |
|
Microvesicle formation |
Shedding of damaged membrane fragments |
Loss of membrane surface area and bioactive vesicle release |
May contribute to inflammation and thrombosis |
[36] |
Table 3. Principal cellular and membrane mechanisms involved in the development of storage lesions in packed red blood cells (PRBCs) and their effects on erythrocyte quality and transfusion outcomes.
5. Biochemical Changes During Storage
Packed red blood cells experience a series of progressive biochemical changes during the refrigerated storage that are collectively called storage lesions. Mature erythrocytes do not have mitochondria or a nucleus, and thus rely solely on anaerobic glycolysis to produce energy and maintain cellular homeostasis. Over time, metabolic activity slows with a depletion of important metabolites, build-up of metabolic waste, imbalance of ions and more oxidative damage. These biochemical changes have a negative impact on the viability of the erythrocytes, integrity of the erythrocyte membrane, capacity to deliver O2 and post-transfusion recovery.
5.1 ATP Depletion
The main energy source needed for the structural and functional integrity of RBCs is adenosine triphosphate (ATP). It regulates the activity of membrane ion pumps, helps to keep membranes phospholipid asymmetric, maintains intracellular ion balance, and keeps membranes flexible. In refrigerated storage the glycolytic enzyme activity gradually decreases, which results in a gradual decrease in ATP production, but cellular ATP levels remain utilized for key metabolic processes. The amount of ATP in the cell decreases significantly as the storage period is prolonged. Normally the reduction in ATP will reduce the activity of the sodium–potassium ATPase, causing ionic imbalance, membrane rigidity, and decreased erythrocyte deformability. Moreover, when ATP levels are low, the rapidity of membrane vesiculation, osmotic fragility, and hemolysis are increased. As such, ATP-depleted erythrocytes used for transfusion have a shorter survival time in the blood of the recipient and lower therapeutic effectiveness [37].
5.2 Decrease in 2,3-Diphosphoglycerate (2,3-DPG)
2,3-Diphosphoglycerate (2,3-DPG) is a crucial glycolytic intermediate that controls the oxygen-binding ability of hemoglobin. At normal 2,3-DPG levels, the oxygen dissociation curve of haemoglobin moves to the right, releasing oxygen to the tissues surrounding the heart. After 14 days of refrigeration, the levels of 2,3-DPG in blood are usually extremely low, to the point where they are almost impossible to detect. Low temperatures primarily cause a drop because they suppress metabolism and reduce glycolytic activity. When 2,3-DPG levels fall, hemoglobin's oxygen affinity rises, limiting the quantity of oxygen that may be delivered to tissues immediately following a transfusion. Anyone requiring a large blood transfusion or severely ill patients during periods of low 2,3-DPG should be aware of the potential drawbacks of the short-term fall in 2,3-DPG [38].
5.3 Glucose Consumption
Mature erythrocytes use glucose as their sole energy substrate, and continually metabolize it via anaerobic glycolysis. Glucose slowly breaks down during storage to produce ATP for cell maintenance and normal function of the cell membrane. Preservative solutions have extra glucose but as the glucose is used up by the metabolic activity, it continues to be depleted over time. Depleted glucose supplies result in decreased ATP production and exacerbate further metabolic decline. As glycolysis slows down, the integrity of the erythrocyte membrane and the ability to sustain its ionic regulation is gradually impaired, exacerbating the storage lesion.
5.4 Lactate Accumulation
In red blood cells, the major product of anaerobic glycolysis is lactate. During refrigerated storage, glucose continues to be metabolised, causing the concentration of lactate in the storage solution to increase over time. There is a continuous rise in lactate concentration, which is related to the continued anaerobic metabolism in spite of diminished enzyme activity. High levels of lactate can directly lead to acidification of the storage medium, and also interfere with glycolytic enzymes further decreasing ATP production. High lactate concentrations are thus a useful biochemical parameter to assess storage-induced metabolic deterioration [39].
5.5 pH Reduction
Lactate builds up during storage, causing a progressive decrease in the pH of the storage solution. Preservative solutions buffer for a while, but over time these buffers are overwhelmed. A decrease in pH will have a negative impact on several intracellular enzymes essential for glycolysis and energy production. Acidification further increases oxidative injury, decreases the function of membrane proteins and increases ATP depletion. Low pH thus leads to a marked decrease in the viability of the erythrocytes, and hemolysis is enhanced during long storage.
5.6 Potassium Leakage
The intracellular potassium concentration is maintained by the ATP-dependent sodium–potassium pumps present in the erythrocyte membrane. During storage, the activity of these ion pumps gradually decreases as the ATP content decreases. Loss of membrane integrity and defects in ion transport leads to leakage of potassium out of the erythrocytes into the surrounding storage solution. The potassium concentration in the outside of the cell therefore rises gradually during the storage time. If you are transfusing older PRBC units, such as in a massive transfusion or a transfusion to a baby, an elevation of potassium can lead to hyperkalemia and cardiac problems. Thus, one of the clinically significant biochemical changes that occurs with the prolonged storage of blood is the build-up of potassium [40].
5.7 Sodium Alterations
Unlike potassium leakage, sodium slowly flows into erythrocytes due to a decrease in sodium–potassium ATPase activity. This ionic homeostasis disrupts leads to osmotic imbalance and changes in the intracellular water content. Sodium changes are usually not as clinically relevant as potassium changes, but indicate progressive membrane dysfunction and decreased cell metabolism. Changes in both sodium and potassium levels are indications of decreasing membrane transport potential during storage, when combined.
5.8 Oxidative Stress and Reactive Oxygen Species
A storage lesion develops due in large part to oxidative stress. The auto-oxidation of hemoglobin and other oxidative reactions cause reactive oxygen species (ROS) to be constantly created during cold storage. Glutathione, catalase, superoxide dismutase, and glutathione peroxidase are antioxidant defense systems found in normal red blood cells that help to neutralize excess reactive oxygen species (ROS). But with prolonged storage these anti-oxidant mechanisms start to reduce, leading to oxidative imbalances. This led to damage to the ROS of phospholipids, cytoskeletal proteins, membrane transport proteins, and hemoglobin molecules. Oxidative injury leads to increased lipid peroxidation, protein oxidation, vesiculation of the membranes and decreased erythrocyte deformability. Oxidative stress also is a primary cause of hemolysis during storage and will play a significant role in the progressive decline in PRBC quality during storage [41].
5.9 Free Hemoglobin Release
Free hemoglobin will be released from the erythrocytes during prolonged storage, when some erythrocytes gain integrity in the storage material. The level of extracellular free hemoglobin rises with the duration of storage and is considered to be a reliable marker of the impairment of erythrocytes. This free Hb has biological implications as it freely binds nitric oxide (NO) leading to decreased NO availability and endothelial dysfunction and vasoconstriction. Overwhelming free hemoglobin can also be responsible for excess oxidative injury and inflammatory responses after transfusion. The regulatory agencies set allowable limits for hemolysis of blood stored in units, but it is also important to minimize the release of free hemoglobin in stored units to ensure the safe and effective use of PRBC transfusion. As a whole, these metabolic changes are quite interdependent. Red blood cells in storage suffer from deterioration in quality and functional performance due to oxidative stress, glucose consumption, “loss of 2,3-DPG, pH drop, accumulation of lactate, and depletion of ATP and 2,3-DPG”. Better storage solutions and preservation procedures can be developed to lower the occurrence of storage lesions and improve transfusion results, therefore understanding these biochemical changes is helpful [42].
|
Biochemical Parameter |
Direction of Change During Storage |
Underlying Cause |
Clinical Significance |
|
ATP |
↓ |
Reduced glycolytic activity and continuous ATP consumption |
Decreased membrane integrity, reduced deformability, shortened RBC survival |
|
2,3-DPG |
↓ |
Suppressed glycolysis during refrigerated storage |
Lower oxygen transport to tissues and an increase in the hemoglobin-oxygen affinity |
|
Glucose |
↓ |
Continuous utilization as the primary energy substrate |
Reduced ATP synthesis and impaired cellular metabolism |
|
Lactate |
↑ |
Ongoing anaerobic glycolysis |
Increased anaerobic metabolism and acidification of the storage medium |
|
pH |
↓ |
Accumulation of lactate and metabolic by-products |
Enzyme inhibition, ATP depletion, and cellular dysfunction |
|
Potassium (Kâº) |
↑ |
Failure of Naâº/Kâº-ATPase and membrane leakage |
Increased risk of hyperkalemia, particularly during massive or neonatal transfusion |
|
Sodium (Naâº) |
Altered (intracellular ↑) |
Impaired membrane ion transport |
Disturbed ionic balance and membrane dysfunction |
|
Reactive Oxygen Species (ROS) |
↑ |
Hemoglobin auto-oxidation and declining antioxidant defenses |
Oxidative damage to membrane lipids, proteins, and hemoglobin |
|
Free Hemoglobin |
↑ |
Progressive hemolysis and membrane disruption |
Indicator of hemolysis; contributes to endothelial dysfunction and reduced nitric oxide availability |
Table 4. Major Biochemical Changes in Packed Red Blood Cells During Storage [43]
6. Hematological Changes During Storage
Packed red blood cells undergo several biochemical and hematological changes during storage that impact the structural integrity, morphology and functional characteristics of the erythrocytes. These changes occur gradually in course of refrigerated storage and are closely related with storage lesions. Changes in blood cell morphology, stability, deformability, hematological parameters and EVs production can have a profound impact on the survival of donor RBCs and their function. It is important to recognize these hematological changes to assess the quality and clinical effectiveness of stored PRBCs.
6.1 Morphological Changes
The progressive change on the morphology of RBCs is one of the earliest and most prominent signs of storage lesion. Normally, fresh erythrocytes are disc-shaped (discocytes), able to traverse small capillaries and possess a wide surface area that promotes gas transfer. Over the course of refrigerated storage these changes gradually occur, as ATP is depleted, oxidative injuries take place, and the composition of lipids in the membrane changes. Consequently, discocytes start to change into echinocytes, which have several small membrane projections evenly spaced. The formation of the echinocytes may be reversible to a certain extent, but if stored for a long period of time, irreversible damage is done to the membrane. The erythrocytes continue to change, some of them becoming even more spheroidal, smaller, with less surface area and greater rigidity, as they continue to be stored. Spherocytes have reduced deformability and are more maybe taken up by the spleen and undergo splenolysis following transfusion. The progressive morphological changes will be important indicators of the reduction of erythrocyte quality during storage [44].
6.2 Membrane Fragility
Erythrocyte membrane slowly deteriorates during the refrigerated storage period. Oxidative stress causes membrane phospholipid and cytoskeletal protein damage, which in turn causes loss of membrane integrity, and loss of ATP leads to the loss of phospholipid asymmetry and ion homeostasis. The more unstable the membrane the more delicate the erythrocyte and the more susceptible to mechanical and osmotic stress it is. The fragility of the membrane makes stored RBCs more susceptible to early rupture during processing, transport and transfusion. The fragility of the membrane tends to correlate with the length of time stored and is a measure of the build up of metabolic and oxidative damage to the erythrocyte membranes.
6.3 Hemolysis
Hemolysis is a crucial hematological alteration that happens when blood is stored. This happens when the membrane deteriorates with time, causing the erythrocytes to burst and releasing intracellular chemicals into the storage solution. Hemolysis levels rise steadily with storage time due to a number of factors, including oxidative stress, lipid peroxidation, protein oxidation in membranes, and diminished membrane flexibility. There are generally limits set by regulatory authorities for the amount of hemolysis that can be found in stored PRBC units, but the more the unit is hemolyzed, the fewer viable erythrocytes will be available for the transfusion and the higher the extracellular levels of free hemoglobin, potassium and other intracellular constituents. Hemolysis is therefore a significant quality-control parameter in blood banking, and excessive hemolysis could affect the therapeutic efficacy of blood transfusion and transfusion safety [45].
6.4 Reduced Deformability
Red blood cell deformability refers to the fact that RBCs can alter their shape in order to fit through capillaries that are narrower than their resting diameter. The maintenance of the normal biconcave shape depends mainly on the elasticity of the membrane, the integrity of the cytoskeleton, the viscosity of the intracellular fluids, and the maintenance of the normal biconcave shape. As the ATP contents deplete due to storage conditions, and as the storage time increases, membrane flexibility is also lost, and the organization of the cytoskeletal components is also affected. Thus erythrocytes stored in blood banks are increasingly rigid and less deformable to mechanical stresses. The decreased deformability reduces the ability of microvascular passage, shortens post transfusion survival, and decreases efficiency of oxygen delivery to peripheral tissues. Loss of deformability is one of the most significant functional changes of storage lesions, directly affecting the clinical function of transfused PRBCs.
6.5 Changes in Red Blood Cell Indices
Hematological indices which change measurably during prolonged storage can give helpful clues to erythrocyte quality. A slight rise in Mean Corpuscular Volume (MCV) may occur during storage since this may lead to sodium accumulation in cells and hence to water influx.A slight rise in Mean Corpuscular Volume (MCV) may happen in the course of storage as disturbances in ion transport promote the accumulation of sodium in cells, which in turn leads to water influx and a mild swelling of the cells. The Mean Corpuscular Hemoglobin is fairly stable as the hemoglobin content of individual erythrocytes does not vary greatly during storage. But there is a small variation that may occur due to hemolysis. Marginal decrease in Mean Corpuscular Hemoglobin Concentration (MCHC) may result due to alterations in cell volume and membrane integrity. This is a progressive structural change in stored erythrocytes, although such changes are typically small. During storage, RDW rises, as the cells lose membrane, swell and shrink, and morphologically change to various extents, making the cell population more heterogeneous. A rise in RDW thus indicates greater variation in erythocyte size and morphology which is correlated with storage lesions [46].
6.6 Microparticle Formation
One of the hallmarks of long-term storage of PRBCs is the liberation of red blood cell-derived microparticles (also known as extracellular vesicles). The membrane-bound vesicles are produced on membrane budding and vesiculation due to oxidative stress, ATP depletion, calcium influx, and cytoskeletal disruption. Vesiculation is one way of eliminating damaged parts of the membrane, but excessive vesiculation causes progressive loss of membrane surface area, increased formation of spherocytes and increased susceptibility (fragility) of erythrocytes. Moreover, these microparticles are enriched with biologically active molecules, membrane proteins, hemoglobin, and phospholipids which can trigger inflammation, endothelial activation, coagulation and immune modulation after transfusion.The number of microparticles rises steadily during refrigerated storage and it is now being used as a useful marker of the severity of the storage lesion. Therefore, tracking the generation of microparticles during storage of PRBCs could be useful for understanding the quality and integrity of the stored PRBCs and contribute to the development of better blood processing methods.
|
Hematological Parameter |
Storage-Related Change |
Underlying Mechanism |
Clinical Significance |
|
RBC Morphology |
Discocyte → Echinocyte → Spherocyte |
ATP depletion, membrane lipid loss, oxidative damage |
Reduced cell survival and impaired microcirculation |
|
Membrane Fragility |
Increased |
Lipid peroxidation and cytoskeletal protein damage |
Greater susceptibility to hemolysis |
|
Hemolysis |
Increased |
Progressive membrane rupture |
Release of free hemoglobin and potassium |
|
Deformability |
Decreased |
Membrane rigidity and cytoskeletal alterations |
Reduced capillary passage and post-transfusion recovery |
|
MCV |
Slight increase |
Intracellular sodium and water accumulation |
Indicates altered cell volume regulation |
|
MCH |
Minimal change |
Stable intracellular hemoglobin content |
Limited diagnostic significance during storage |
|
MCHC |
Slight decrease |
Membrane alterations and increased cell volume |
Reflects changes in hemoglobin concentration |
|
RDW |
Increased |
Greater variation in cell size and morphology |
Marker of storage-induced erythrocyte heterogeneity |
|
Microparticles |
Increased |
Membrane vesiculation due to oxidative and mechanical stress |
Associated with inflammation, thrombosis, and endothelial dysfunction |
Table 5. Major Hematological Changes in Packed Red Blood Cells During Storage [47]
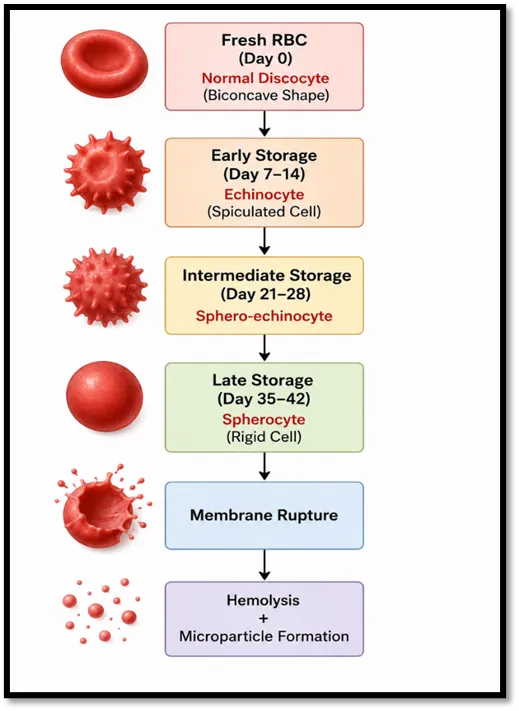
Fig 4. Schematic representation of the progressive morphological transformation of red blood cells during refrigerated storage, illustrating the transition from normal discocytes to echinocytes, sphero-echinocytes, and spherocytes, ultimately leading to hemolysis and microparticle formation.
7. Clinical Implications of Storage Lesions
Significant therapeutic implications may arise from the possibility that the storage damage of packed red blood cells (PRBCs) in these cells affects the safety and effectiveness of blood transfusions. Erythrocyte function and post-transfusion effectiveness can be impacted by changes in biochemical and haematological parameters, such as ATP depletion, reduction in 2,3-DPG, oxidative stress, membrane damage and hemolysis, leakage of potassium ions, and the creation of microparticles. The oxygen transport to peripheral tissues is temporarily reduced due to a drop in 2,3-DPG and the decreased mobility of red blood cells and the increase of hemolysis leads to a release of free hemoglobin that could participate in the creation of oxidative stress, endothelial dysfunction and impaired tissue perfusion. In stored PRBCs, progressive accumulation of potassium can lead to hyperkalemia, especially in neonates, renal impaired patients or rapid and massive transfusion. Furthermore, inflammatory mediators and microparticles derived from transfusion-related storage may cause immune activation and vascular inflammation after transfusion [48]. These effects are thought to be more important in critically ill patients, trauma and those who receive multiple or high-volume transfusion, which can lead to worse clinical results due to storage lesions. While the present blood banking procedures ensure satisfactory quality of stored PRBCs, further measures are still needed to reduce the storage lesions to make blood transfusion a safer and more effective treatment [49].
8. Strategies to Minimize Storage Lesions
Reduce storage lesions and avoid deterioration to many methods have been devised to ensure that packed red blood cells (PRBCs) maintain their quality while stored in the refrigerator. In order to improve erythrocyte longevity, restrict hemolysis, and facilitate ATP synthesis, new additions such Saline Adenine Glucose Mannitol , AS-1, AS-3, and AS-5 contain nutrients and membrane stabilizers. Removing WBCs prior to storage helps to reduce the buildup of inflammatory cytokines, ROS, and other bioactive substances, which helps to minimize oxidative damage and transfusion reactions. Use of proper storage conditions, preferably 2-6°C, a good quality control system, and proper storage times are critical to uphold the PRBCs' structural and functional integrity. Vitamins C and E, glutathione, and N-acetylcysteine are antioxidants that have been tested in clinical trials for their ability to reduce oxidative stress, to protect components of membranes, and to limit hemolysis, but there is a need for additional clinical validation before these interventions are routinely used. Furthermore, new preservation technologies like hypoxic storage systems, better additive solutions, rejuvenation solutions, and metabolomics, proteomics and artificial intelligence-based new methods of quality assessment present excellent potential to further decrease the storage-related lesions while also enhancing blood transfusion safety and effectiveness [50].
9. Future Perspectives
Progress has been made in understanding further study is needed to maximize storage quality and transfusion outcomes, as there are biochemical and hematological changes that occur during the preservation of packed red blood cell products. The creation of more effective additives to reduce oxidative stress, keep membrane integrity intact during storage, preserve 2,3-DPG levels, and increase ATP needs more investigation. Elucidation of other biomarkers such as extracellular vesicles, oxidative stress markers, metabolic signatures etc. could be used to determine the quality of PRBCs more accurately than the based on the storage period only, which would help in improving the quality control in blood banking. Individualized blood storage strategies according to donors' characteristics, such as sex, age, and metabolic profile, could further optimize the effectiveness of blood preservation and transfusion. Furthermore, potential breakthroughs in omics sciences as metabolomics, proteomics, lipidomics and genomics are helping to better elucidate the molecular mechanisms of storage lesions, which could aid in the development of future generations of preservation methods. Future clinical studies with well-designed research incorporating these new technologies will be crucial in order to reduce storage lesions, optimize the quality of stored PRBCs and better ensure the safety and efficacy of blood transfusion.
CONCLUSION
Packed red blood cells are a vital component of transfusion medicine and are a vital part of treating clinical conditions in which blood is lost, such as anemia, trauma, major surgery. Storage lesions develop, however, during long storage in the refrigerator, causing the progressive biochemical and hematological changes which impact the erythrocytes quality and functional integrity. These changes involve ATP depletion, 2,3 diphosphoglycerate depletion, oxidative stress, electrolyte imbalance, membrane damage, decreased deformability, hemolysis and microparticle formation, which can negatively affect oxygen delivery and post transfusion survival of red blood cells. Storage lesions cannot be avoided, but appropriate blood banking procedures and preservation methods do help to ensure acceptable storage quality. The continuous improvement of additive solutions, leukoreduction, antioxidant based preservation and development of new technologies has demonstrated promising potential to reduce storage related deterioration. Blood storage research aimed at finding reliable biomarkers, novel preservation techniques, and the clinical effects of storage lesions is crucial to optimize blood storage and improve transfusion outcomes. Improved knowledge of these changes will aid in creating safer and more effective transfusion practices that will improve patient care and the quality of blood banking practice.
REFERENCES

Priyanka Ghosh*, Suman Chakraborty, Sambit Roy, Impact Of Storage Lesions On Biochemical And Hematological Parameters Of Packed Red Blood Cells, Int. J. Sci. R. Tech., 2026, 3 (7), 534-552. https://doi.org/10.5281/zenodo.21412874
 10.5281/zenodo.21412874
10.5281/zenodo.21412874