
We use cookies to ensure our website works properly and to personalise your experience. Cookies policy
Department of Pediatric and Preventive Dentistry, Guru Nanak Dev dental College and Research Institute, Sunam, India
Dental caries remains one of the most prevalent chronic diseases worldwide, particularly affecting children and high risk populations. Although fluoride has been the cornerstone of caries prevention for decades, concerns regarding fluorosis, systemic overexposure, and patient acceptance have driven increasing interest in non fluoridated alternatives. Contemporary caries management emphasizes early detection, risk based prevention, and minimally invasive interventions that preserve natural tooth structure. This review comprehensively evaluates non fluoridated caries preventive strategies, categorizing them into physical barriers, mineral enhancers, biofilm modifiers, and antimicrobial agents. Emphasis is placed on pit and fissure sealants, resin infiltration, casein phosphopeptide–amorphous calcium phosphate (CPP ACP), hydroxyapatite, bioactive glass, theobromine, arginine, xylitol, probiotics, and selected antimicrobial agents. The mechanisms of action, clinical applications, advantages, limitations, and current evidence supporting these agents are discussed. Collectively, non fluoridated approaches offer effective, biologically sound, and patient friendly alternatives or adjuncts to fluoride, aligning with the principles of modern preventive and minimally invasive dentistry.
Oral health is a fundamental component of general health and quality of life, enabling essential functions such as mastication, speech, and social interaction. Dental caries is a biofilm‑mediated, sugar‑driven, multifactorial disease characterized by alternating phases of demineralization and remineralization of the tooth hard tissues. Despite significant global reductions in caries prevalence over recent decades, the disease remains highly prevalent among children and other high‑risk groups. (Rošin-Grget K et al, 2013).
Historically, caries management relied predominantly on surgical removal of diseased tooth structure and placement of restorations. Advances in cariology have shifted this paradigm toward prevention, early diagnosis, and non‑invasive or minimally invasive interventions. Remineralization‑based strategies now form the foundation of modern caries management, focusing on arresting or reversing early lesions rather than restoring cavitated defects.
Fluoride has played a central role in caries prevention due to its ability to inhibit demineralization and enhance remineralization. However, excessive fluoride exposure may lead to adverse outcomes such as dental fluorosis, particularly in young children. Additionally, growing public concern regarding systemic fluoride intake has prompted exploration of effective non‑fluoridated alternatives. This review aims to synthesize current evidence on non‑fluoridated caries preventive agents and technologies, highlighting their mechanisms, clinical effectiveness, and role in contemporary dental practice.
Demineralization- Remineralization Dynamics
Dental caries results from a dynamic imbalance between pathological factors (acidogenic bacteria, fermentable carbohydrates, and reduced salivary flow) and protective factors (saliva, calcium, phosphate, and preventive interventions). (Featherstone JDB 2004). Acid production by cariogenic microorganisms such as Streptococcus mutans lowers plaque pH below the critical threshold (~5.5), resulting in dissolution of hydroxyapatite crystals and subsurface enamel demineralization.
Enamel demineralization initially manifests as non‑cavitated white spot lesions, characterized by increased porosity beneath a relatively intact surface layer. Importantly, this process is reversible. When pH returns to neutral and adequate calcium and phosphate ions are available, remineralization can occur, restoring mineral content and improving enamel resistance to future acid attacks.
Saliva plays a pivotal role in this balance by buffering acids, supplying minerals, and facilitating clearance of carbohydrates and microorganisms. Modern preventive strategies aim to enhance remineralization, stabilize biofilms, and maintain favorable oral environmental conditions to prevent lesion progression. (ten Cate JM 2001)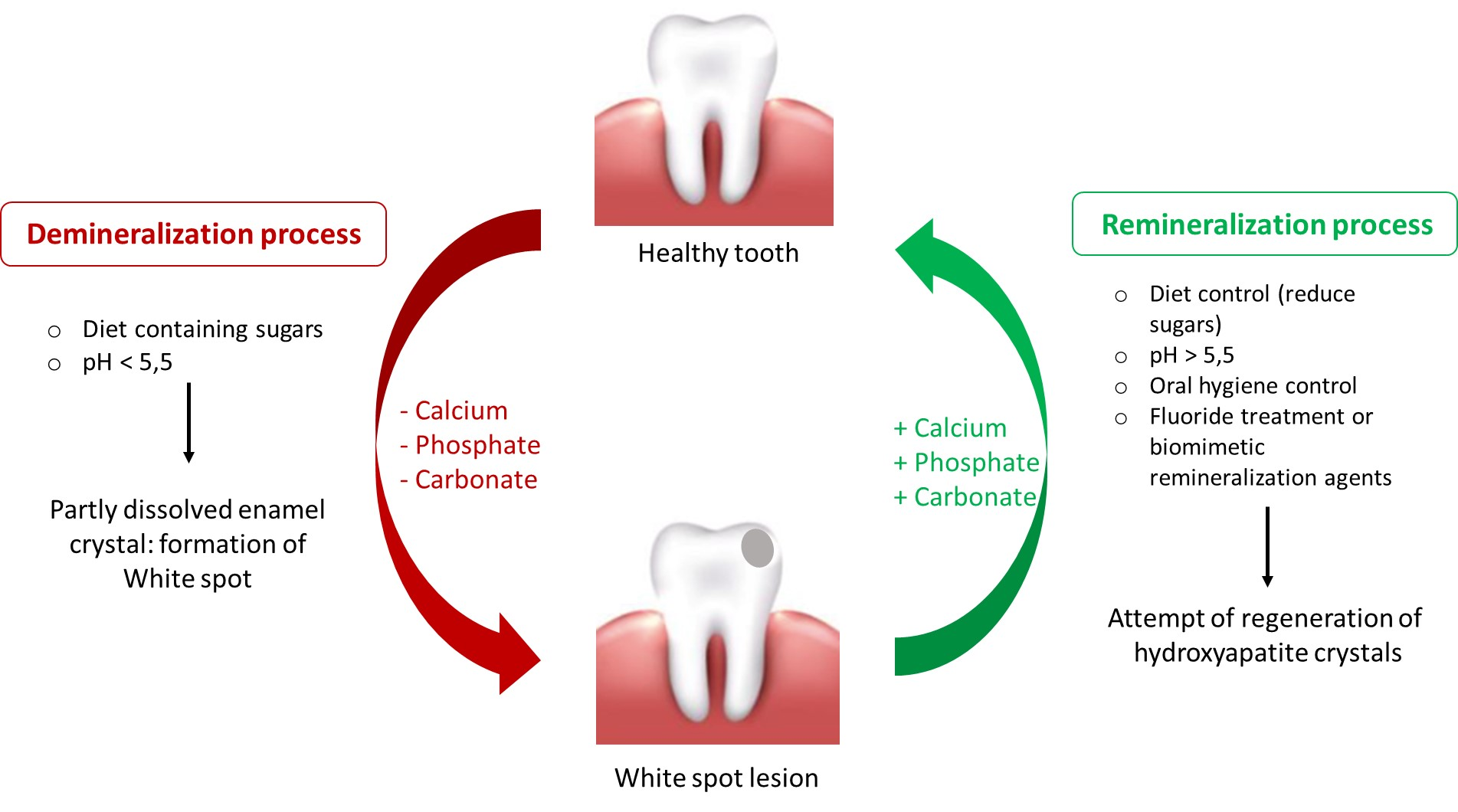
Figure 1: Demineralization and remineralization dynamics
Modern Caries Management Philosphy
The contemporary approach to caries management is guided by the principle of “preserve tooth structure and restore only when necessary.” This philosophy emphasizes risk assessment, early lesion detection, and the use of preventive or micro‑invasive techniques to arrest disease progression. Non‑fluoridated agents support this paradigm by offering safer options for susceptible populations while maintaining efficacy in caries prevention and control. (Schwendicke F, Frencken JE, Bjørndal L, et al. 2016)
Classification of Non-Fluoridated Caries Preventive Agents
Non‑fluoridated caries preventive strategies can be broadly categorized based on their primary mechanism of action:
PHYSICAL BARRIERS
Pit and fissure sealants are resin‑ or glass ionomer‑based materials applied to occlusal pits and fissures of caries‑susceptible teeth, forming a protective barrier that prevents bacterial colonization and nutrient access. Sealants are a cornerstone of preventive dentistry, particularly in children and adolescents. (Simonsen RJ 2002)

Figure 2: Resin sealant placement technique
1.1 Types of Sealants
1.2 Clinical Effectiveness
Long‑term studies demonstrate significant reductions in occlusal caries incidence when sealants are properly applied and maintained. Although glass ionomer sealants show lower retention rates compared to resin‑based materials, their caries‑preventive effect may persist due to residual material in fissures and ion release.
Resin infiltration is a micro‑invasive technique designed to arrest non‑cavitated enamel lesions by infiltrating a low‑viscosity resin into the porous lesion body. (Paris S, Meyer-Lueckel H. 2010). The commercially available system (Icon®, DMG) utilizes hydrochloric acid etching, ethanol drying, and resin infiltration to occlude diffusion pathways for acids.

Figure 3: Components of Icon
2.1 Mechanism of Action
The infiltrant penetrates enamel porosities via capillary action, polymerizes within the lesion, and forms a diffusion barrier that inhibits further demineralization. Additionally, resin infiltration improves the optical properties of white spot lesions by matching the refractive index of sound enamel.
2.2 Clinical Applications
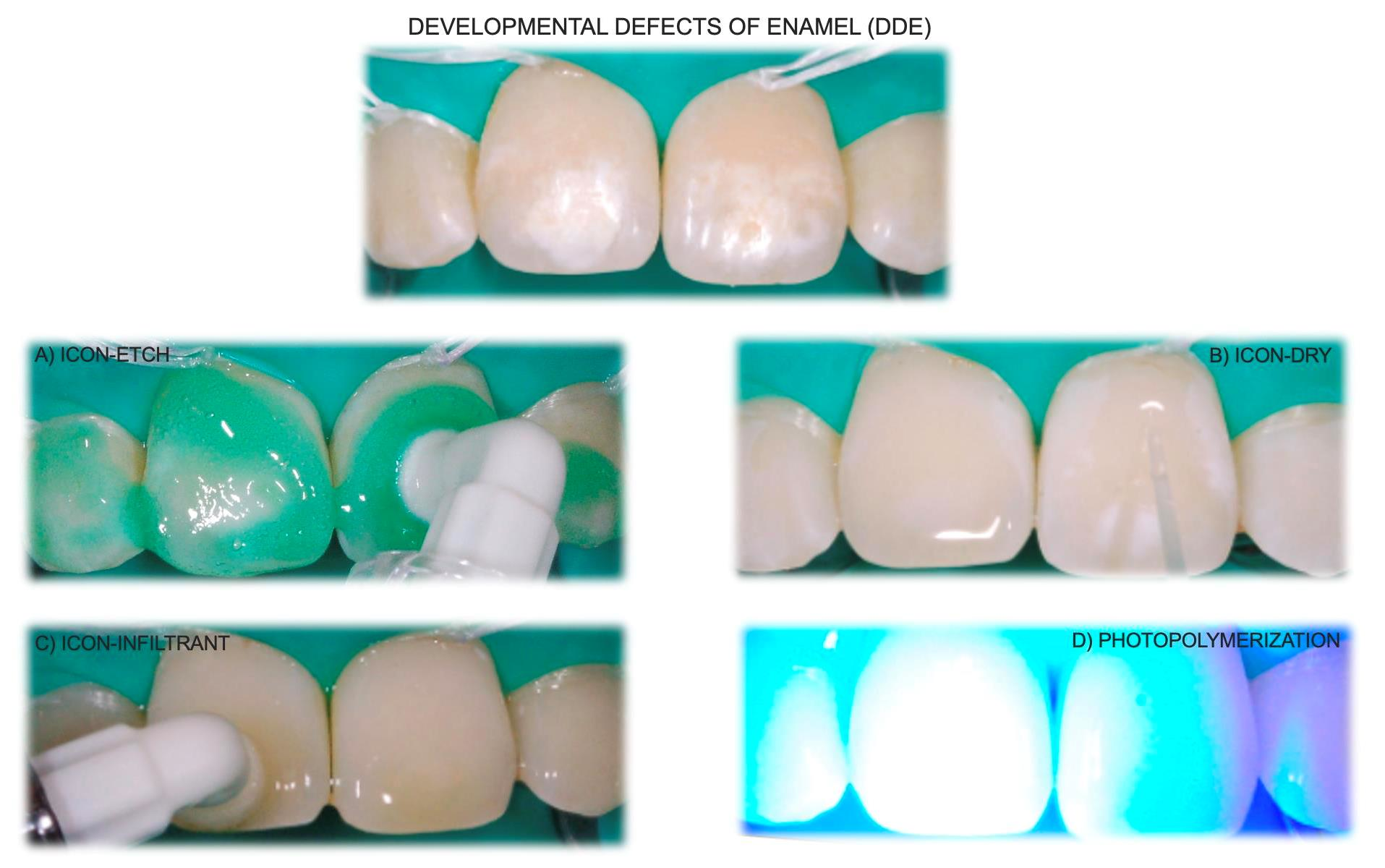 Figure 4: Icon resin infiltration technique
Figure 4: Icon resin infiltration technique
2.3 Limitations
Limited penetration into dentin, potential long‑term discoloration, and technique sensitivity are recognized drawbacks. Ongoing research focuses on enhancing resin formulations with antibacterial and remineralizing components.
MINERAL ENHANCERS
CPP‑ACP is a milk‑derived remineralizing agent that stabilizes calcium and phosphate ions in an amorphous, bioavailable form. It acts as a reservoir of minerals within dental plaque and enamel, promoting remineralization and inhibiting demineralization. (Reynolds EC. 1997)
Clinical studies demonstrate its effectiveness in reversing white spot lesions and enhancing enamel resistance, particularly when used as topical creams or chewing gums. (Beerens MW, van der Veen MH, van Beek H, ten Cate JM 2010)
Synthetic hydroxyapatite mimics the natural mineral structure of enamel. Nano‑hydroxyapatite particles can penetrate enamel defects, fill micro‑porosities, and promote surface remineralization. Its excellent biocompatibility and absence of toxicity make it suitable for long‑term use. (Amaechi BT AbdulAzees PA, Alshareif DO et al, 2019)

Figure 5: Schematic overview showing the modes of action of HAP in the remineralization and protection of enamel
Bioactive glass releases calcium, phosphate, and sodium ions in aqueous environments, leading to the formation of a hydroxycarbonate apatite layer on the tooth surface. This process enhances remineralization and provides a protective effect against acid challenges.

Figure 6: Remineralizing characteristics of Bioglass
Theobromine, a natural alkaloid found in cocoa, has been shown to enhance enamel crystallinity and hardness. It promotes the formation of larger, more acid‑resistant apatite crystals and represents a promising fluoride‑free alternative.
BIOFILM MODIFIERS
Arginine metabolism by arginolytic bacteria produces ammonia, increasing plaque pH and counteracting acidogenic challenges. Arginine‑containing products have demonstrated reduced caries activity and improved plaque ecology.
Xylitol is a non‑fermentable sugar alcohol that inhibits Streptococcus mutans growth and adhesion. Regular xylitol use enhances salivary flow and reduces cariogenic bacterial load.
(Zero DT. Sugars 2009)

Figure 7: Bi-facet therapeutic efficacy of xylitol on dental caries
Probiotics aim to restore microbial balance by introducing beneficial bacteria that compete with cariogenic species. Emerging evidence supports their adjunctive role in caries prevention.
ANTIMICROBIAL AGENTS
Natural agents such as propolis, green tea catechins, and essential oils, as well as synthetic agents like chlorhexidine, contribute to caries prevention by reducing microbial load and inhibiting biofilm formation. Their role is primarily adjunctive within comprehensive preventive regimens.
DISCUSSION
Non‑fluoridated caries preventive strategies align well with modern concepts of minimally invasive dentistry. These agents address multiple aspects of the caries process, including mineral loss, biofilm dysbiosis, and surface vulnerability. While fluoride remains highly effective, non‑fluoridated alternatives provide valuable options for individuals at risk of fluorosis, those with specific medical or social considerations, and populations seeking fluoride‑free preventive care
CONCLUSION
A multifaceted strategy is essential for preventing caries in children, typically commencing with appropriate oral hygiene practices such as brushing twice daily and rinsing to eliminate plaque build-up. In addition, managing dietary intake and ensuring regular dental visits can support children in maintaining healthy teeth, fostering a positive relationship with oral hygiene, and preventing the onset of more serious dental issues down the line. Moreover, the use of remineralizing agents in caries prevention represents a significant advancement in modern dentistry. Unlike traditional fluoride methods, non-fluoridated agents work by replenishing essential minerals, such as calcium and phosphate, while also offering alternative approaches to enhance enamel strength and repair microscopic damage. Thus, by integrating these innovative strategies into oral care routines, dentists and researches aim to create a proactive defense system that not only prevents caries but also promotes long-term oral health. (Walsh T, Worthington HV, Glenny AM, et al 2010)
Caries preventive strategies employ a range of mechanisms, among which pit and fissure sealants and resin infiltration are notable for their barrier mechanism. Sealants are applied in the pits and fissures of teeth to inhibit the development of caries, providing essential protection for children with an increased risk of cavities, whereas resin infiltration is commonly used to address early carious lesions on smooth surfaces, particularly white spot lesions on the facial surfaces of anterior teeth. Some compounds utilize a mechanism to elevate mineral saturation, which encompasses CPP-ACP, hydroxyapatite, bioactive glass, and theobromine. These agents provide bioavailable calcium and phosphate ions to demineralized regions, facilitating the restoration of mineral balance and the enhancement of tooth structure integrity. Another approach employed by remineralizing agents involves the alteration of biofilm through pH and microbial modulation. Compounds such as arginine and xylitol function as pH modifiers, creating a more alkaline environment that counteracts the acidogenic activity of cariogenic bacteria, thereby preventing caries. Probiotics, in contrast, play a crucial role in maintaining a balanced oral microbiome by suppressing harmful bacteria and fostering beneficial strains. In addition, agents like chlorhexidine, triclosan, povidone iodine, propolis etc, exhibit antimicrobial properties that can be incorporated into a non-fluoridated prevention plan.
Thus, encouraging awareness and consistency in these practices, not only prevent caries but also enhance children's well-being and self-esteem through a healthier smile.
REFERENCES

Gursimran Kaur*, Varinder Goyal, Puneet Goyal, Shaveta, Non Fluoridated Materials For Caries Prevention: A Comprehensive Review, Int. J. Sci. R. Tech., 2026, 3 (4), 1134-1139. https://doi.org/10.5281/zenodo.19881827
 10.5281/zenodo.19881827
10.5281/zenodo.19881827