
We use cookies to ensure our website works properly and to personalise your experience. Cookies policy
University Institute of Pharmacy, Pt. Ravishankar Shukla University, Raipur, Chhattisgarh- 492010
Alzheimer’s disease [AD], recognized as the leading cause of dementia, is marked by a gradual decline in cognitive function linked to the buildup of amyloid-? [A?] plaques and neurofibrillary tangles [NFTs]. Existing pharmacological treatments, such as the newly developed monoclonal antibodies like Lecanemab, only offer symptomatic benefits and are frequently hindered by inadequate penetration of the blood-brain barrier and safety issues, including amyloid-related imaging abnormalities [ARIA]. These drawbacks highlight the necessity for safer and more effective multi-target therapeutic approaches. Plant-based neuroprotective compounds from traditional practices such as Ayurveda and Traditional Chinese Medicine [TCM] have surfaced as valuable alternatives because of their diverse mechanisms of action. Phytochemicals like curcumin, bacosides from Bacopa monnieri [Brahmi], withanolides from Withania somnifera [Ashwagandha], and triterpenoids from Centella asiatica [Gotu Kola] display properties that are anti-amyloid, antioxidant, anti-inflammatory, and modulate cholinergic activity. Moreover, Melissa officinalis [Lemon Balm] shows acetylcholinesterase inhibition, along with benefits for anxiety and behaviour. Although there is promising preclinical data and some limited clinical evidence, challenges such as low bioavailability and the lack of large-scale randomized controlled trials continue to be significant hurdles. Future investigations should prioritize standardized formulations, nano-delivery techniques, and comprehensive clinical validation to completely utilize the therapeutic potential of these natural compounds in managing Alzheimer’s disease.
Among dementias, Alzheimer's disease [Anti-Alzheimer Disease] is the most common. Its primary characteristic is cognitive impairment, which has an impact on patients' physical and emotional health [1] China Alzheimer Report 2024 [via Beijing Review, March 2025]. Alzheimer's disease affects more than 5% of those aged 60 and older. Projections suggest that there will be 19.11 million Anti-Alzheimer Disease patients in this age group by 2030 [2]. Anti-Alzheimer Disease is a neurological condition that develops clinically and is typified by cognitive impairment-induced memory loss, behavioral abnormalities, and dementia. Anti-Alzheimer Disease, frequently known as the "Plague of the Twenty-First Century [3]. In its severe stages, the disease can cause hallucinations, amnesia, and disorientation in addition to a progressive loss of memory and other cognitive abilities. Malnutrition, aspiration pneumonia, dysphagia, or infection can ultimately cause the patient to pass away [4,5]. Although the precise pathogenetic mechanisms of Anti-Alzheimer Disease are still unknown, it is generally accepted that neurofibrillary tangles [i.e., aggregates of hyperphosphorylated tau protein] and excessive accumulation of insoluble amyloid β protein [Aβ], which forms senile plaques in the extracellular space and on blood vessel walls, are the main factors contributing to its development [6,7,8]. Recent developments in neuropharmacology have accelerated the hunt for multi-targeted therapeutic agents, especially molecules derived from plants that have antioxidant, anti-inflammatory, and neuroprotective qualities[9]. For a long time, AD-related disorders have been treated using traditional Chinese medicine [TCM], which has produced a large body of evidence. According to TCM, the kidneys "support brain function." The "kidney essence," a material said to be produced by the kidneys, is believed to support and sustain the brain's physiological processes. Cognitive decline and a reduction in brain function can be caused by a renal essence shortage [10].
Given that AD is a dynamic and progressive disease and that neuroinflammation plays a role in its onset and progression, HLXLD is thought to be a promising treatment for AD. HLXLD may target multiple amyloid-mediated neuroinflammation and immune response pathways to cure AD in microglial cells and 5xFAD transgenic rats, according to a previous study by Liang Y et al [11].
However, further research is still required to fully understand the underlying mechanism, especially as it relates to altered AD metabolism. Metabolomics is a high-throughput analysis method that uses quantitative analysis of endogenous small molecule metabolites to determine the link between metabolites and physiological and pathological changes. Targeted and untargeted metabolomics are the two primary subfields of metabolomics study. The most traditional type of metabolomics, known as untargeted metabolomics, measures hundreds or even thousands of metabolites and looks for metabolic signatures linked to certain disease states or phenotypes in order to study the entire network that generates metabolic activity. Targeted metabolomics is a very sensitive and accurate quantitative assessment of a particular molecule or metabolic network [12].
2. METHODS
2.1 Underlying Causes and Disease Mechanisms of Alzheimer’s Disease
Significant neuronal loss and interference with inter-neuronal transmission are hallmarks of AD. Numerous biomarkers have been identified as a result of extensive research that has shed light on the important molecular pathways underpinning the pathophysiology of AD. These biomarkers offer vital resources for AD surveillance and early diagnosis. These biomarkers allow for the tracking of disease progression and make it possible to diagnose AD early, even in people who may seem clinically healthy. According to current research, AD biomarkers can be categorized into four key domains: neuropsychological evaluation, metabolic signatures, genetic indicators, and biochemical markers [13].
2.2 Pathobiology of Alzheimer’s Disease
Developing successful treatment options requires an understanding of the various pathways implicated in the mechanisms of AD pathogenesis. Regretfully, the exact mechanisms that underlie the pathophysiology of AD are yet unknown. The type 1 transmembrane glycol-protein, which contains 695–770 amino acids, is thought to be broken down by proteases to produce the Aβ peptide. Extracellular secretase breaks down APP close to the cell membrane, releasing a soluble extracellular fragment called sAPPα. β-secretase-1 [BACE-1] is another protease that breaks down APP, producing a different extracellular soluble fragment called sAPPβ as well as a membrane-attached fragment called C 99. A γ-secretase complex, comprising four proteins [presenilin, nicastrin, anterior pharynx faulty, and presenilin enhancer], further breaks down the C 99 fragment. The catalytic subunit of this complex is presenilin, which is encoded by the PSEN1 or PSEN2 genes. The peptide known as the amyloid intracellular domain is left behind after γ-secretase is broken. The Aβ peptide comes in two different lengths: the low solubility form, which has 42 amino acids [Aβ1–42], and the most common form, which has 40 amino acids [Aβ1–40]. When β amyloid peptides are deposited, oligomers, protofibrils, fibrils, and eventually amyloid plaques form—all of which are characteristic signs of AD pathology. Deposition of Aβ in the brain is thought to be a major initial step in the development of AD, starting in the entorhinal cortex and hippocampal regions. Additionally, tau protein hyperphosphorylation and intracellular accumulation lead to the development of NFT, which exacerbates axonal transport impairment and cytoskeletal disruption [14].
3. CURRENT THERAPEUTIC APPROACHES AND THEIR CONSTRAINTS
3.1 Pharmacotherapy Approaches
The pharmacological perspective, which is based on changes in neurotransmitter levels linked to disease, is described as neuroprotective or symptomatic. With an emphasis on addressing neurotransmitter imbalances that develop as the disease progresses, the current pharmaceutical therapy of AD is primarily symptomatic and neuroprotective.
The goal of these treatments is to improve the current quality of life provided to patients and caregivers by reducing cognitive and behavioural symptoms, even while they do not stop or reverse disease pathology [15]. Memantine, donepezil, galantamine, and rivastigmine are the four approved medications currently available on the market. They belong to the two families of AChE inhibitors and anti-glutaminergics. These medications are used topically or taken orally. AChE inhibitors function by raising the brain's levels of ach, a neurotransmitter implicated in memory and necessary for neuronal communication. These medications are intended to treat the acetylcholine deficit seen in AD patients' central nervous systems [16]. N-methyl-D-aspartate [NMDA] receptors are non-competitive antagonists of anti-glutaminergics, which control glutamate levels Neuronal injury can result from high glutamate levels, a neurotransmitter linked to memory and learning. The objectives of these therapies are to control behavioral symptoms, stabilize or momentarily enhance cognitive abilities, and slow the course of the illness. Despite the fact that these treatments are not curative, they can assist people with AD and their guardians maintain their independence and improve their quality of life. Nevertheless, their effectiveness is restricted and transient, focusing solely on symptoms rather than the fundamental cause of AD [17]. Low oral bioavailability [about 36% for donepezil and 40% for galantamine], poor blood-brain barrier [BBB] penetration, limited therapeutic windows, and variable half-lives [donepezil: ~70 h; rivastigmine: ~1.5 h] are some of its clinical drawbacks. Higher dosages are usually needed since the [BBB] severely limits drug transport to the central nervous system, raising the possibility of side effects [18]. These difficulties show how urgently better CNS-targeted administration methods are needed [19]. Lecanemab and Donanemab are two examples of disease-modifying treatments that have surfaced in recent years. These monoclonal antibodies have the ability to reduce cognitive deterioration in people with early-stage AD by targeting amyloid-β plaques, a defining feature of AD pathogenesis. These medications are not curative, though, and not all patients can benefit from them despite their potential. They carry a number of serious hazards, chief among them being amyloid-related imaging abnormalities [ARIA], which include micro-hemorrhages and brain enlargement. Notwithstanding these developments, the limited advantages and possible adverse effects of the pharmacotherapies now in use highlight the need for more focused and efficient therapeutic approaches [20].
3.2 Non-Pharmacological treatment
Recent studies highlight the potential for small-to-moderate, clinically significant improvements from non-pharmacological therapies for individuals with Alzheimer's disease [AD], particularly when administered for at least 16 weeks and customized to meet behavioural, cognitive, and functional demands. According to high-quality meta-analyses, structured cognitive stimulation therapy [CST; the original 14-session protocol] is an effective core treatment in routine care for mild-to-moderate dementia because it improves working memory, language, global cognition, neuropsychiatric symptoms, and quality of life [21]. One of the best options is still exercise: according to a 2025 BMJ Open meta-analysis of RCTs, aerobic exercise raises quality of life and improves MMSE and ADAS-Cog scores [with the strongest effects when programs run >16 weeks, 3+ sessions/week, ~30-50 minutes each session] [22]. The value of combining exercise modalities to target strength, balance, and endurance in addition to cognition is further supported by a broader 2025 network meta-analysis, which indicates that several exercise modalities [aerobic, resistance, and multicomponent] each contribute and can enhance activities of daily living [23]. Complementary benefits of cognitive rehabilitation include enhanced memory and everyday functioning through goal-oriented, therapist-guided techniques incorporated into routine work [24]. When tailored to individual preferences, music-based therapies for behavioural and psychological symptoms can be used in both home and care-home settings. They can also produce minor cognitive advantages and lessen agitation and despair [25]. Larger trials are still required, but new RCT evidence suggests that complete, lifestyle-based multimodal regimens [exercise, stress management, diet, and social/cognitive engagement] are feasible and may stabilize or slightly enhance cognition and function over a 12-month period. All of these results point to the need for a person-centered, multi-component plan that is anchored by CST and regular exercise and enhanced by cognitive rehabilitation, customized music therapy, and caregiver-supported lifestyle modification. This plan should be delivered with consideration for safety/fall-risk management, caregiver training, adherence, and dose [≥16 weeks] [26].
3.3 Ayurvedic Perspectives on the Treatment of Neurological Disorders
Over traditional medical care, Ayurvedic care can be constructed around lifestyle and mind-body practices, adjunct procedures, and Medhya-Rasayana [nootropic rejuvenation]. A randomized, double-blind, placebo-controlled trial of fenugreek-galactomannan curcumin showed improvements across cognition-related outcomes versus placebo over 8 weeks, suggesting utility as an adjunct in early cognitive decline. However, larger, longer trials are still required. Curcumin, which frequently has enhanced bioavailability, is the botanical that has shown the most recent clinical signal in individuals with dementia or cognitive impairment. [27].
The combination of multi-target pharmacology, acceptable safety profiles, and translational data in Ayurvedic phytopharmaceuticals has stimulated renewed interest in response to Alzheimer's disease and related neurocognitive diseases. Curcumin, especially the more recent, enhanced-bioavailability formulations, has made the most progress in randomized clinical trials among these agents. When formulated to overcome oral bioavailability limitations, optimized curcumin extracts may produce clinically relevant cognitive benefits, according to a randomized, double-blind, placebo-controlled, three-arm trial of a fenugreek-galactomannan curcumin formulation [CGM/CurQfen®] administered as 400 mg twice daily over several months. The trial also showed favourable biomarker trends versus placebo. Mechanistic preclinical research demonstrating anti-amyloid, anti-inflammatory, antioxidant, and mitochondrial protective properties that likely mediate cognitive effects confirm these findings [28].
4. PROSPECTIVE PLANT-BASED MEDICINES
4.1 Ashwagandha [Withania somnifera]
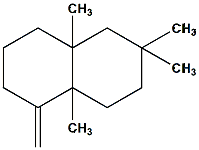
Traditionally categorized as a Rasayana [rejuvenative tonic] for fostering vigor, longevity, and resilience against stress, Withania somnifera often known as Indian ginseng or ashwagandha, is one of the most extensively researched medicinal plants in Ayurveda. It has been used for centuries to treat inflammatory, metabolic, and neurological conditions. It is a member of the Solanaceae family. The plant's wide pharmacological profile is a result of its many different bioactive components, chief among them being sitoindosides, alkaloids, and withanolides. [32].
Ashwagandha, or Withania somnifera, is another phytopharmaceutical that has increasing randomized-trial support for objectives related to stress and cognition. Recent RCTs have shown that standardized extracts administered at doses usually between ~225 and 600 mg/day improve memory, attention, and associated cognitive activities in older adults and MCI groups. They have also been shown to reduce perceived stress and improve sleep parameters. Preclinical research suggests a number of neurodegenerative mechanisms, such as the reduction of oxidative stress and neuroinflammation, the attenuation of the HPA-axis, and neurotrophic/neurogenic effects. These mechanistic findings support ashwagandha as a potential adjunctive treatment in the absence of larger disease-specific RCTs and supplement human trials [29].
4.2 Mandukaparni/Gotu kola [Centella asiatica]
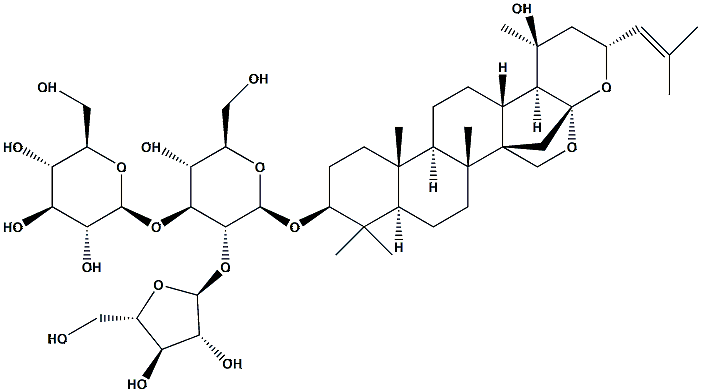
Centella asiatica [L.] Urban, a perennial creeping herb of the Apiaceae family, is also referred to as gotu kola in English and mandukaparni in Ayurveda. For centuries, it has been utilized as a Medhya Rasayana [nootropic and brain tonic] in Ayurveda, Traditional Chinese Medicine, and other ethnomedical systems to improve longevity, memory, and intellect. Widely acknowledged as a revitalizing herb for neurological and psychological health, C. asiatica has long been used to treat anxiety, cognitive decline, skin conditions, and wound healing.
The plant's neuroprotective, antioxidant, anti-inflammatory, and adaptogenic qualities are attributed to a variety of triterpenoid saponins, including asiaticoside, madecassoside, brahmoside, and brahminoside, as well as flavonoids, tannins, and volatile oils [33].
Preclinical and early human research with Centella asiatica [Mandukaparni/Gotu kola] indicates a convergent signal for improving working memory and attentional processing. Mechanistic studies emphasize the modification of synaptic plasticity pathways, support for mitochondrial respiration, and activation of antioxidant genes. Larger, sufficiently powered RCTs are necessary to confirm clinical efficacy and optimal dosing, but small clinical trials and ongoing feasibility studies in older adults and MCI populations report improvements on specific working memory tasks and mood/anxiety measures, suggesting Centella's suitability as a phytopharmaceutical candidate especially where vascular or metabolic contributors to cognitive impairment are suspected [30]
4.3 Brahmi [Bacopa monnieri]
Brahmi, or Bacopa monnieri [L.] Wettst., is a perennial creeping herb that is a member of the Plantaginaceae [previously Scrophulariaceae] family. Traditionally used to improve memory, learning ability, and cognitive function, it is one of the most esteemed Medhya Rasayana [nootropic and intellect-promoting herbs] in Ayurveda. In Indian, Chinese, and other traditional medical systems, the plant has been used extensively to treat ailments like anxiety, epilepsy, sleeplessness, and neurocognitive deterioration. In terms of phytochemistry, B. monnieri is abundant in alkaloids, flavonoids, sterols, and other glycosides in addition to triterpenoid saponins called bacosides [bacoside A and B]. Its neuroprotective, antioxidant, anti-inflammatory, and adaptogenic qualities are mostly due to these bioactive substances [34].
Numerous small trials have shown that Bacopa monnieri [Brahmi] improves memory and processing speed in both healthy persons and people with MCI. It also has strong ethnopharmacological support. Bacopa may be taken into consideration for cognitive complaints and prevention strategies, but without additional high-quality RCTs, the current evidence does not support its use as a monotherapy for established Alzheimer's disease. This is because systematic reviews focusing on populations with Alzheimer's disease report very low-certainty evidence and no consistent benefit over placebo or standard cholinesterase inhibitors in established AD cohorts. Longer follow-up and standardized extract formulations are required to address trial result heterogeneity [31].
4.4 Shankhpushpi [Convolvulus pluricaulis]
In Ayurveda and other traditional medical systems, Convolvulus pluricaulis Choisy, also called Shankhpushpi, is a well-known medicinal herb that is mainly appreciated as a Medhya Rasayana [nootropic and brain tonic]. The plant, which is a member of the Convolvulaceae family, has been used for centuries to improve learning, memory, focus, and general cognitive function. Often used to treat anxiety, sleeplessness, epilepsy, and cognitive decline, Shankhpushpi is regarded in Ayurvedic classics as a powerful rejuvenating agent for neurological and psychological health. Alkaloids [including convolvine and convolamine], flavonoids, glycosides, and coumarins are abundant in C. pluricaulis' phytochemical makeup, which supports its wide range of pharmacological actions [35].
Cholinergic neurotransmission, oxidative stress pathways, and neuroinflammation are all impacted by Convolvulus pluricaulis [shankhpushpi] and a number of other traditional medhya herbs, such as Nardostachys jatamansi and Tinospora cordifolia, which exhibit multi-target neuroprotective activity in both in vitro and animal models. Though human clinical evidence is still limited to small trials or observational reports, network-pharmacology and computational analyses have identified plausible target networks relevant to dementia pathology. To establish therapeutic value and safety in neurodegenerative disease, rigorous RCTs with standardized preparations are required [36].
|
Herb [Co-Name]/ Bio-Name |
Plant Part Used |
Mechanism of Action |
Major Phyto-constituents |
Representative Structure |
Ref |
|
Ashwagandha [Winter Cherry]/Withania somnifera |
Root, Leaves |
Neuroprotection by GABA-mimetic action, antioxidant activity, cortisol reduction, and anti-inflammatory |
Withanolides [Withaferin A, Withanolide D], Alkaloids [Somniferine] |
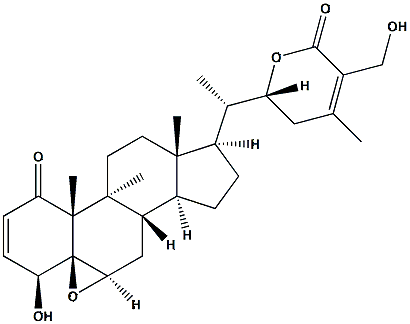
|
[74] |
|
Gotu Kola [Mandukaparni]/ Centella asiatica |
Leaves, Whole plant |
Increases cognition, microcirculatio, antioxidants, and neurite outgrowth. |
Triterpenoid saponins [Asiaticoside, Madecassosid, Flavonoids |
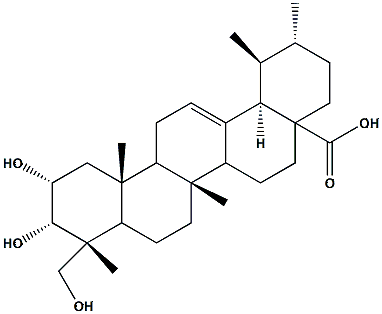
|
[75] |
|
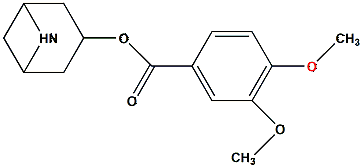
Brahmi/ Bacopa monnieri |
Leaves, Whole plant |
Inhibits β-amyloid accumulation, alters the cholinergic system, and is an antioxidant. |
Bacosides [Bacoside A, Bacoside B], Alkaloids, Saponins |
|
[76] |
|
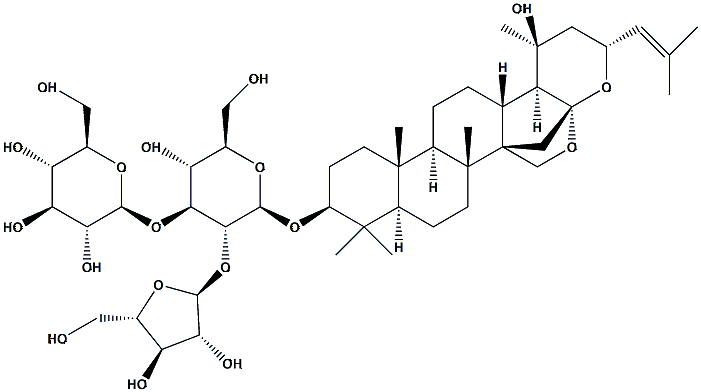
Shankhpushpi/ Convolvulus pluricaulis |
Whole plant |
Anxiolytic, antioxidant, and nootropic through cholinergic modulation |
Alkaloids [Convolvine, Convolamine], Flavonoids, Glycosides |
|
[77] |
Table:1 Prospective Plant-Based Medicines with Neuroprotective and Cognitive-Enhancing Potential
5. HERBAL PLANT AND THEIR PARTS INVESTIGATED FOR ANTI-ALZHEIMER’S EFFECT
5.1 Bacopa monnieri [Brahmi]
The primary materials utilized in preclinical and clinical research are the aerial parts and leaves of the creeping perennial Bacopa monnieri [L.] Wettst. Since they are thought to be the primary neuroactive components, extracts are usually standardized to total bacosides [a family of dammarane-type triterpenoid saponins, including bacoside A components and bacopasaponins]; flavonoids and minor alkaloids are also included. In randomized trials and translational studies, standardized leaf extract formulations—such as CDRI-08, Bacognize®, and Synapsa®—are most commonly used [37].
5.1.1 Pathophysiology
Oxidative stress and malfunctioning mitochondria - In neural models, bacosides and other phenolics lower lipid peroxidation and ROS and boost endogenous antioxidant defenses [upregulate SOD, catalase, and glutathione], protecting mitochondria and maintaining neuronal bioenergetics. Since oxidative damage is a major cause of synaptic dysfunction in AD, bacopa's antioxidant properties offer a tenable way to slow down synapse loss and neuronal death [38].
Amyloid-β [Aβ] and anti-amyloid activity - Bacopa extracts have been shown in both in vitro and animal studies to decrease Aβ-induced neurotoxicity, apoptotic signaling downstream of Aβ exposure, and certain amyloid-related cellular effects through proteostasis and antioxidant pathways. Although there isn't any concrete proof that bacopa lowers plaque burden in AD in humans, these preclinical anti-amyloid effects aid in the explanation of neuroprotective results in model systems [39].
Cholinergic modulation [symptomatic pathway] - As acetylcholinesterase [AChE] inhibitors or modulators of cholinergic signaling, bacoside congeners and other Bacopa constituents have been identified in a number of studies using computational/molecular docking and biochemical assays. The cholinergic deficit at the heart of AD symptomatology can be addressed by temporarily improving attention, memory encoding, and recall through decreased AChE activity and increased acetylcholine availability [40].
Synaptic plasticity and neurotrophic support - When bacopa is administered to rodents, it improves long-term potentiation [LTP]-like measurements and increases the expression of synaptic proteins and neurotrophic indicators [such as BDNF]. These effects help reverse the synaptic disruption that predicts cognitive loss in AD and are likely responsible for gains in working memory, learning, and processing speed seen in clinical trials [41].
Anti-inflammatory/anti-apoptotic effects - Bacopa addresses the neuroinflammatory cascades that spread dementia by lowering caspase-dependent death in neuronal cultures and animal models, as well as pro-inflammatory signaling [reducing cytokines like TNF-α/IL-1β in some studies] [42].
5.2 Nardostachys jatamansi [Jatamansi]:
A perennial member of the Valerianaceae [Caprifoliaceae] family, Nardostachys jatamansi DC. is used extensively in Ayurveda as a Medhya Rasayana [nervine and nootropic tonic]. The main medicinal components under investigation are the rhizomes and roots, which have a rich profile of flavonoids, lignans, neolignans, jatamanvaltrates, and sesquiterpenes [jatamansone/spirojatamol, nardostachone, and aristolone]. Together, these bioactive compounds give it neuroprotective, anxiolytic, antioxidant, and memory-boosting qualities. [44]
5.2.1 Pathophysiology
Oxidative stress and mitochondrial dysfunction - One of the main characteristics of AD is oxidative damage, which causes synapse loss and neuronal death. In mouse brains, jatamansi rhizome extracts decrease lipid peroxidation and increase the activity of endogenous antioxidant enzymes such as glutathione, catalase, and superoxide dismutase. Both neuronal survival and mitochondrial function are preserved by this defense against reactive oxygen species [ROS]. [43]
Neuroinflammation - Neuronal damage in AD is caused by neuroinflammatory pathways that include cytokine release, NF-κB signaling, and microglial activation. In vitro and in animal models, sesquiterpenes such as jatamansone exhibit anti-inflammatory properties by reducing pro-inflammatory cytokines [TNF-α, IL-6]. This modification lessens synaptic damage brought on by neuroinflammation. [45].
Cholinergic neurotransmission - Cholinergic neuron loss is correlated with cognitive deterioration in AD. In docking and enzymatic experiments, extracts of N. jatamansi have demonstrated acetylcholinesterase inhibitory activity, indicating symptomatic relief through increased synaptic acetylcholine availability. This mechanism is similar to the reasoning behind approved AD medications [rivastigmine, donepezil]. [46]
Amyloid-β toxicity and aggregation - According to both silico and in vivo research, jatamansi's phytoconstituents may attenuate Aβ-induced oxidative stress and apoptosis, hence indirectly lowering amyloid-mediated neurotoxicity, even if its direct anti-amyloid properties are less well-characterized than those of bacopa or ashwagandha. [47]
Neuropsychiatric symptoms [NPS] in AD - Common comorbidities in AD include anxiety, sadness, and sleep disorders, all of which exacerbate the course of the illness. In rodent behavioral paradigms [elevated plus maze, forced swim test], jatamansi root extracts demonstrate anxiolytic and antidepressant qualities that are associated with GABAergic modulation and antioxidant activity. Through the treatment of behavioral and psychological symptoms, these effects may enhance the quality of life for AD patients. [48] .
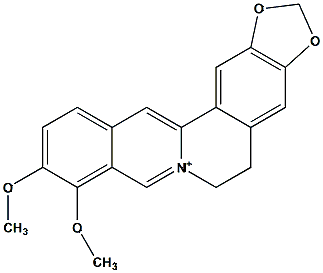
5.3 Tinospora cordifolia [Guduchi]
In Ayurveda, Tinospora cordifolia [Willd.] Miers, often known as Guduchi or Amrita, is a well-known Rasayana plant that is prized for its ability to restore and preserve the nervous system. The main medicinal component is the stem, which is abundant in glycosides, polysaccharides, alkaloids [berberine, magnoflorine], and diterpenoid lactones [tinosporide, cordifolide] that provide a variety of pharmacological effects. The main pathogenic characteristics of Alzheimer's disease [AD] include tau protein hyperphosphorylation, oxidative stress, amyloid-β buildup, cholinergic deficiency, and neuroinflammation. T. cordifolia extracts specifically target these processes. According to preclinical research, stem components preserve cholinergic neurotransmission, which is essential for memory and learning, by inhibiting acetylcholinesterase [AChE] and butyrylcholinesterase. By upregulating glutathione, catalase, and superoxide dismutase, its antioxidant action strengthens endogenous defenses and lessens the harm that free radicals cause to neurons. [53]
Cholinergic Dysfunction: The cholinergic deficit observed in AD is counteracted by stem-derived alkaloids and lactones, which increase acetylcholine levels and improve synaptic transmission by inhibiting acetylcholinesterase [AChE] and butyrylcholinesterase [BChE].[49]
Oxidative Stress: Higher levels of lipid peroxidation and mitochondrial dysfunction are seen in AD brains. Extracts from guduchi stems protect neurons from oxidative damage by increasing the activity of antioxidant enzymes [SOD, catalase, and GSH] and lowering ROS.[50]
Neuroinflammation: In AD, neurodegeneration is caused by persistent microglial activation. Stem polysaccharides reduce neuroinflammation and preserve synaptic plasticity by inhibiting NF-κB-mediated cytokine production [TNF-α, IL-1β, and IL-6].[51]
Amyloid & Tau Pathology: Although primarily preclinical, new research indicates stem components may protect cytoskeletal proteins against tau hyperphosphorylation and prevent amyloid-beta aggregation. [52]
5.4 Gotu Kola [Centella Asiatica]
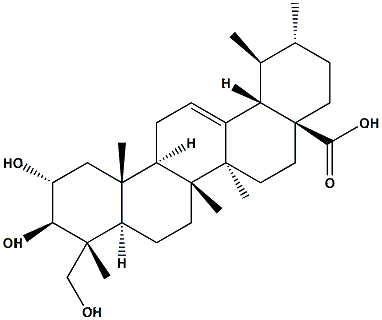
The potential of herbal plants to cure Alzheimer’s disease [AD] by addressing its intricate and multifaceted pathophysiology has been well studied. Centella asiatica, often known as gotu kola, is an herb that has been used for centuries for its ability to improve cognitive function. Bioactive chemicals, mainly pentacyclic triterpenoids such asiaticoside, madecassoside, siatic acid, and madecassic acid, are abundant in the plant’s sections, especially the leaves and aerial parts. The ability of these substances to penetrate the blood-brain barrier is thought to contribute to their effectiveness. They tackle the characteristics of AD using a number of methods. Their anti-amyloid-beta [Aβ] action is one important way by which they shield neurons from the harmful effects of Aβ plaques by preventing their aggregation.[54] Additionally, the triterpenoids have potent antioxidant qualities that aid in scavenging free radicals and lowering oxidative stress, which is a contributing factor to dementia. Additionally, they have anti-inflammatory properties that help to reduce the chronic neuroinflammation linked to AD. Additionally, studies indicate that they may enhance synaptic plasticity and neurogenesis, two critical mechanisms for restoring damaged neurons and enhancing cognitive performance. Although encouraging, a large portion of the data comes from preclinical research; more thorough clinical trials are required to completely validate its effectiveness in AD patients.[55]
Amyloid-beta [Aβ] plaque buildup is one of the defining features of Alzheimer’s disease [AD], which impairs neuronal function and causes neurotoxicity. Asiatic acid and asiaticoside, two of Centella asiatica’s triterpenoid chemicals, have anti-amyloid qualities by disrupting pre-formed fibrils and inhibiting Aβ aggregation. By protecting neurons from Aβ-induced oxidative and excitotoxic stress and lowering plaque burden, this strategy eventually improves memory performance.[56]
5.4.1.2 Antioxidant Mechanisms
A major contributing element to AD pathogenesis is oxidative stress, which is brought on by excessive free radical generation and mitochondrial malfunction. Strong antioxidants found in Centella asiatica boost the activity of enzymes such as glutathione peroxidase, catalase, and superoxide dismutase [SOD]. These substances prevent oxidative damage to neuronal cell membranes, DNA, and mitochondria by scavenging free radicals and reducing lipid peroxidation. Long-term neuronal survival and cognitive resilience are supported by this protective mechanism.[57]
5.4.1.3 Anti-Inflammatory Action
Neuronal loss in AD is accelerated by chronic neuroinflammation, which is mediated by hyperactivated astrocytes and microglia. Centella asiatica’s bioactive triterpenoids decrease the release of cytokines like TNF-α, IL-1β, and IL-6 and inhibit important inflammatory mediators like NF-κB. The herb slows the progression of dementia and maintains neural networks by modifying these inflammatory pathways.[58]
In AD, mitochondrial dysfunction is another important pathophysiological event that results in neuronal death and decreased ATP synthesis. Centella asiatica extracts decrease oxidative stress in the mitochondria, stabilize membrane potential, and improve mitochondrial efficiency. By preserving energy balance in neurons, this promotes healthy synaptic transmission and brain activity.[59]
Loss of plasticity and synaptic dysfunction are intimately related to cognitive decline in AD. It has been demonstrated that Centella asiatica stimulates the CREB signaling pathway and increases Brain-Derived Neurotrophic Factor [BDNF], both of which are critical for hippocampus neurogenesis and synaptic strengthening. The herb enhances learning capacity and memory formation by reestablishing synaptic plasticity and encouraging the growth of new neurons.[60]
One well-known feature of AD pathogenesis is a loss in cholinergic transmission brought on by decreased acetylcholine levels. Acetylcholine availability in synaptic clefts is prolonged by Centella asiatica's mild acetylcholinesterase inhibiting actions. Like traditional AD medications, this approach improves cholinergic neurotransmission to improve cognitive function, but it also has multi-targeted advantages.[61]
5.5 Lemon Balm [Melissa officinalis]
Lemon balm, or Melissa officinalis, is a herb that shows promise in treating Alzheimer's disease [AD] since it targets the pathology of the illness in multiple ways. Several important bioactive substances, including as rosmarinic acid and other terpenoids, are present in the plant's leaves and essential oil and support its medicinal properties. The main way it works is by blocking the enzyme acetylcholinesterase [AChE], which degrades the neurotransmitter acetylcholine. As a typical tactic in traditional AD treatments, Lemon Balm helps raise acetylcholine levels in the brain by inhibiting this enzyme. By scavenging free radicals and shielding neurons from harm, the herb's high antioxidant content—especially rosmarinic acid—allows it to fight oxidative stress.[62] Additionally, it has anti-inflammatory qualities that aid in reducing the long-term neuroinflammation that hastens dementia. Lemon balm is well known for its soothing and anxiolytic properties, which have been demonstrated in clinical trials to help manage the agitation and behavioural problems frequently associated with AD, in addition to these direct neurological advantages. This makes it a useful adjunctive treatment for enhancing patients' quality of life and cognitive performance.[63]
5.5.1.1 Cholinergic Modulation [Acetylcholinesterase Inhibition]
The decrease in acetylcholine [ACh] levels brought on by acetylcholinesterase [AChE] activation is a key characteristic of AD. Bioactive substances found in Melissa officinalis include terpenoids with AChE inhibitory action and rosmarinic acid. Lemon balm improves cholinergic neurotransmission by extending the amount of ACh available in synaptic clefts through the inhibition of AChE. With fewer side effects, this mechanism is comparable to those of traditional AD medications like donepezil and rivastigmine.[64]
A major factor in AD is oxidative stress, which speeds up tau and amyloid pathology and causes neuronal damage. Rosmarinic acid, caffeic acid, and flavonoids, which scavenge free radicals and boost antioxidant defenses, are abundant in Melissa officinalis. This slows down neurodegeneration and maintains neuronal health by lowering lipid peroxidation and mitochondrial oxidative damage.[65]
According to certain experimental research, rosmarinic acid prevents amyloid-beta [Aβ] from aggregating, which lowers plaque buildup and shields neurons from Aβ-induced damage. Furthermore, its neuroprotective properties enhance neuronal survival and maintain synaptic integrity.[67]
In addition to its direct neurological effects, lemon balm is well known for its ability to soothe, relax, and reduce anxiety by interacting with muscarinic and GABAergic receptors. In addition to its cognitive advantages, clinical research reveal that it substantially improves quality of life by lowering agitation, sleeplessness, and behavioural abnormalities in AD patients.[68]
5.5.1.5 Holistic Multi-Targeted Approach
Melissa officinalis treats several pathogenic features of AD, in contrast to single-target medications:
6. The effect of natural products on Alzheimer’s disease
Since natural compounds contain a variety of pharmacological properties, such as neuroprotection, antioxidant defence, anti-inflammatory activity, anti-amyloidogenic potential, and neurotransmitter system control, they have become attractive options for treating Alzheimer's disease [AD]. The main characteristics of Alzheimer's disease, a progressive neurodegenerative illness, include aberrant extracellular buildup of amyloid-β [Aβ] plaques, intracellular tau protein hyperphosphorylation that results in neurofibrillary tangles, chronic oxidative stress, mitochondrial dysfunction, excitotoxicity, and neuroinflammation. Progressive cognitive decline, synaptic malfunction, and neuronal death are the results of these pathogenic alterations. For the treatment of AD, natural chemicals originating from medicinal plants, food sources, and marine species are particularly appealing since they tend to work on several interconnected pathways, in contrast to typical synthetic medications that are frequently single-target in nature.[66]
The substances that have been investigated the most are polyphenolics. It has been demonstrated that curcumin, the active ingredient in curcuma longa [turmeric], can chelate metal ions like copper and iron, which hasten the formation of plaque, decrease amyloid aggregation, and lessen oxidative stress by upregulating antioxidant enzymes. Resveratrol, a stilbene included in red wine and grapes, also has anti-inflammatory properties and stimulates the SIRT1 pathway, which improves mitochondrial activity and guards against neuronal death. Flavonoids that protect against glutamate-induced excitotoxicity, suppress neuroinflammatory cytokines like TNF-α and IL-1β, and improve synaptic plasticity include quercetin [found in onions and apples] and epigallocatechin gallate [EGCG] from green tea.[70]
Alkaloids are important in the treatment of AD as well. The powerful, reversible acetylcholinesterase inhibitor huperzine A, which is extracted from Huperzia serrata, increases acetylcholine levels in the brain, enhancing memory and cognitive function. Additionally, it has antioxidant qualities and reduces the generation of Aβ via modifying the processing of amyloid precursor protein [APP]. The cholinesterase inhibitory effect of galantamine, another alkaloid from the Galanthus species, has also led to its clinical approval for the treatment of AD.[71]
Ginkgo biloba terpenoids, including ginkgolides and bilobalide, enhance cerebral blood circulation, guard against neuronal damage brought on by free radicals, and suppress pro-inflammatory mediators in microglia. Bacopa monnieri [Brahmi] bacosides also improve neurotransmitter modulation, prevent the production of β-amyloid fibrils, safeguard mitochondrial function, and increase neurotrophic factors such as brain-derived neurotrophic factor [BDNF], which promotes synaptic plasticity. Commonly present in Melissa officinalis and Rosmarinus officinalis, phenolic acids like rosmarinic acid and caffeic acid have potent free radical scavenging properties, inhibit lipid peroxidation, and shield neuronal membranes from oxidative damage.[72]
All of these natural substances work together to reduce oxidative stress, reduce inflammation, prevent Aβ aggregation, alter tau pathology, and maintain neurotransmission, providing a multitargeted treatment approach. Nevertheless, issues like low bioavailability, restricted blood-brain barrier penetration, and dosage and formulation variability continue to impede their widespread clinical use, even in the face of encouraging preclinical and early clinical outcomes. Future studies that combine large-scale clinical trials, herbal formulations that work in concert, and delivery technologies based on nanotechnology may be able to get around these restrictions. Therefore, natural products, which bridge the gap between traditional medicine and contemporary drug discovery, show great promise as both preventive agents and supplemental therapy approaches in Alzheimer's disease.[73]
|
Plant [Biological & Common name] |
Plant part used |
Mechanism of action |
Phytoconstituents |
Chemical structure |
Ref |
|
Bacopa monnieri [Brahmi] |
Whole plant [aerial parts, leaves] |
Modulates cholinergic system [↑ Ach availability], antioxidant [scavenges ROS], anti-amyloid effects, neuroprotective, anxiolytic |
Bacosides A & B, Brahmine, Herpestine, Saponins, Alkaloids |
|
[87] |
|
Nardostachya jatamansi [Jatamansi] |
Rhizomes and roots |
GABAergic modulation, possible MAO inhibition, antioxidant & anti-inflammatory, membrane stabilizing — sedative, antidepressant |
Jatamansone [Valeranone], Nardostachone, Sesquiterpenes, Alkaloids, Flavonoids |
|
[88] |
|
Tinospora cordifolia [Guduchi] |
Stem [climber stem] |
Immunomodulatory [macrophage activation, cytokine modulation], antioxidant, anti-inflammatory, adaptogenic; neuroprotective via reduced neuroinflammation |
Tinosporin, Berberine, Magnoflorine, Cordifolioside A, Tinosporaside |
|
[89] |
|
Centella asiatica [Gotu Kola / Mandukaparni] |
Leaves and stems |
Stimulates neuronal outgrowth/BDNF, antioxidant, anti-inflammatory, improves microcirculation — cognitive enhancer & wound healing |
Asiaticoside, Madecassoside, Asiatic acid, Madecassic acid |
|
[90] |
|
Melissa officinalis [Lemon Balm] |
Leaves |
Inhibits acetylcholinesterase; modulates GABAergic tone; antioxidant; anxiolytic and sedative effects |
Rosmarinic acid, Caffeic acid, Flavonoids, Triterpenes, Essential oils [citral, citronellal] |
|
[91] |
Table:2 Phytochemical and Mechanistic Overview of Selected Neuroprotective Herbs
7. FUTURE DIRECTIONS AND RESEARCH OPPORTUNITIES IN AYURVEDIC APPROACHES FOR ANTI-ALZHEIMER’S
Even though there is increasing evidence that Ayurvedic herbs can protect against Alzheimer’s disease [AD], there are still a number of issues that need to be resolved, which presents many chances for further study. According to recent research, herbs including Convolvulus pluricaulis [Shankhpushpi], Centella asiatica [Gotu Kola], Bacopa monnieri [Brahmi], and Withania somnifera [Ashwagandha] have a variety of multifaceted effects, including cholinergic modulation, anti-inflammatory, antioxidant, and anti-amyloidogenic effects. These processes highlight their potential as alternative or complementary therapy by addressing several characteristics of AD pathogenesis.[78]
Plant sources, extraction techniques, and quantities of bioactive compounds vary widely, which presents a significant obstacle to integrating Ayurvedic medicines into standard clinical practice. Standardizing extracts according to certain bioactive markers should be the main goal of future study in order to guarantee uniform potency and repeatability throughout investigations.[79]
The majority of clinical data supporting Ayurvedic treatments is still restricted to brief, small-scale studies. For a variety of patient populations, including individuals with moderate cognitive impairment [MCI] and early-stage AD, large, multicentre, randomized controlled trials [RCTs] with extended follow-up periods are necessary to evaluate cognitive benefits, appropriate dose, safety, and efficacy.[80]
By incorporating metabolomics, proteomics, and transcriptomics into Ayurvedic research, it is possible to gain a better knowledge of the mechanisms by which these herbal ingredients affect amyloid-beta aggregation, tau hyperphosphorylation, neuroinflammatory pathways, and synaptic plasticity. Using systems biology techniques, multi-component herbal compositions may exhibit synergistic effects.[81]
The therapeutic potential of many phytochemicals is hampered by their low oral bioavailability and restricted blood-brain barrier [BBB] penetration. Advanced delivery methods such as liposomal encapsulations and nano-formulations can improve CNS targeting, decrease systemic adverse effects, and increase bioavailability. Future research on such delivery strategies is a potential direction.[82]
By nature, ayurvedic treatments affect several objectives at once. Combinatorial therapies that combine several herbs or combine Ayurvedic substances with traditional pharmaceutical drugs may be the subject of future research. These approaches, which address both symptomatic alleviation and disease change, may have synergistic effects.[83]
Clinical translation can be strengthened by creating and confirming biomarkers to track treatment response, neuroprotection, and cognitive improvement in patients undergoing Ayurvedic therapy. Personalized therapy based on patient profiles and illness stage may also be possible with biomarker-guided techniques.[84]
To determine the long-term safety of Ayurvedic formulations, particularly for chronic administration, thorough toxicological studies are required. To direct the therapeutic application, standardization, and quality control of these herbal products, regulatory frameworks ought to be created.[85]
Ayurveda has a strong emphasis on holistic treatment, which can be used in conjunction with pharmaceutical interventions. This includes stress management, exercise, and food. Future studies should look at how herbal treatments and Ayurvedic lifestyle choices affect AD patients' cognitive abilities and the course of their illness.[86]
Abbreviations
|
AD |
Alzheimer’s Disease |
|
Aβ |
Amyloid-beta |
|
NFTs |
Neurofibrillary Tangles |
|
ARIA |
Amyloid-Related Imaging Abnormalities |
|
BBB |
Blood-Brain Barrier |
|
TCM |
Traditional Chinese Medicine |
|
HLXLD |
Huan-Lian-Xie-Xin Decoction |
|
RCT |
Randomized Controlled Trial |
|
CST |
Cognitive Stimulation Therapy |
|
MMSE |
Mini-Mental State Examination |
|
ADAS-Cog |
Alzheimer’s Disease Assessment Scale – Cognitive Subscale |
|
MCI |
Mild Cognitive Impairment |
|
HPA |
Hypothalamic–Pituitary–Adrenal [axis] |
|
GABA |
Gamma-Aminobutyric Acid |
|
ROS |
Reactive Oxygen Species |
|
APP |
Amyloid Precursor Protein |
|
BACE-1 |
Beta-Site APP Cleaving Enzyme 1 |
|
NMDA |
N-Methyl-D-Aspartate |
|
ACh |
Acetylcholine |
|
AChE |
Acetylcholinesterase |
|
BChE |
Butyrylcholinesterase |
|
CNS |
Central Nervous System |
|
TNF-α |
Tumor Necrosis Factor Alpha |
|
IL-1β |
Interleukin 1 Beta |
|
IL-6 |
Interleukin 6 |
|
NF-κB |
Nuclear Factor Kappa B |
|
BDNF |
Brain-Derived Neurotrophic Factor |
|
LTP |
Long-Term Potentiation |
|
SOD |
Superoxide Dismutase |
|
GSH |
Glutathione |
|
MAO |
Monoamine Oxidase |
|
DNA |
Deoxyribonucleic Acid |
|
RNA |
Ribonucleic Acid |
|
ATP |
Adenosine Triphosphate |
|
CREB |
cAMP Response Element-Binding Protein |
|
GABAergic |
Related to Gamma-Aminobutyric Acid neurotransmission |
|
ROS |
Reactive Oxygen Species |
|
BACE |
Beta-Site APP Cleaving Enzyme |
|
RDA |
Recommended Dietary Allowance [implied in nutrition context] |
|
WHO |
World Health Organization [contextually implied in AD global data] |
CONCLUSION
Alzheimer’s disease [AD] continues to present significant challenges as a neurodegenerative condition distinguished by the buildup of amyloid, tau hyperphosphorylation, oxidative stress, and neuroinflammation. Although there have been improvements in pharmacological treatment, most current therapies only alleviate symptoms, highlighting the necessity for multi-targeted approaches. Plant-derived neuroprotective compounds show great potential due to their diverse pharmacological properties and favorable safety profiles. Botanicals like Withania somnifera, Bacopa monnieri, Centella asiatica, Tinospora cordifolia, and Melissa officinalis demonstrate strong antioxidant, anti-inflammatory, cholinergic-modulating, and anti-amyloidogenic effects that work together to safeguard neurons and improve cognitive function.
Nonetheless, obstacles such as low bioavailability, absence of clinical standardization, and insufficient large-scale research continue to hinder their therapeutic application. Future research should prioritize the implementation of nanocarriers, phytosomal formulations, and omics-based studies to enhance effectiveness and uncover molecular mechanisms. The combination of these herbal compounds with lifestyle changes and pharmacological treatments could provide a comprehensive and sustainable strategy for managing Alzheimer’s disease. In summary, the integration of traditional Ayurvedic insights with contemporary neuropharmacology offers a promising pathway for developing safe, multi-targeted, and effective therapies that may mitigate cognitive decline and enhance the quality of life for those affected by Alzheimer’s disease.
REFERENCES








Abhishek Nand, Bhoomika Swarnkar, Chhavi Rahangdale, Harkesh Dadsena, Lokprabha Hirwani, Pushpendra Kumar, Yashika Israni, Helina Tandon, Umakant Sahu, Vishal Jain*, Plant-Based Neuroprotective Agents In Alzheimer’s Disease: Mechanisms And Prospects, Int. J. Sci. R. Tech., 2026, 3 (6), 17-35. https://doi.org/10.5281/zenodo.20502670
 10.5281/zenodo.20502670
10.5281/zenodo.20502670