
We use cookies to ensure our website works properly and to personalise your experience. Cookies policy
Saveetha Medical College Hospital, Saveetha Nagar Thandalam, Poonamallee Road NH 48, Chennai - 602105, Tamil Nadu
Diabetic retinopathy (DR) continues to be recognized as one of the foremost causes of preventable blindness worldwide, particularly among working-age adults. Despite the transformative impact of established clinical interventions—most notably pan-retinal photocoagulation (PRP) and intravitreal vascular endothelial growth factor (VEGF) inhibitors—several therapeutic limitations remain unresolved. These include incomplete or variable clinical responses across patient subgroups, the heavy burden of repeated intravitreal injections, progression of localized ischemia despite therapy, and the inability of current treatments to address the underlying multifactorial nature of the disease. DR is not solely a vascular disorder; it is increasingly understood as a complex interplay of metabolic dysregulation, neurodegenerative changes, and chronic inflammatory cascades. This narrative review synthesizes clinical and preclinical literature published between 2015 and 2026, mapping the rapid evolution of the therapeutic landscape. It highlights the transition from conventional anti-VEGF monotherapy toward next-generation multi-target biologics engineered to simultaneously modulate angiogenesis and vascular stability. Beyond VEGF inhibition, novel pathogenic pathways are explored, including the Semaphorin 3A (Sema3A) axis, Tie2 receptor modulators, and inflammatory mediators, which collectively represent promising avenues for disease modification rather than symptomatic control. Neuroprotective strategies, such as encapsulated cell technology delivering ciliary neurotrophic factor (CNTF), and sustained-release corticosteroid implants, are discussed as adjuncts to preserve retinal neuronal integrity. Equally important are breakthroughs in innovative drug delivery systems (DDS). Liposomal nanocarriers, bio-responsive hydrogels incorporating two-dimensional MXenes, and gene therapy vectors are designed to provide sustained intraocular therapeutic levels, reduce patient burden, and potentially achieve “one-and-done” treatment paradigms. These advances are complemented by translational research integrating ultra-widefield optical coherence tomography angiography (UWF-OCTA) and artificial intelligence (AI)-driven risk stratification, which together enable earlier, more precise intervention before irreversible microvascular destruction occurs..
Diabetic retinopathy (DR) has long been described as a microvascular complication of diabetes, characterized by capillary leakage, microaneurysms, hemorrhages, and neovascularization. This classical view, however, is increasingly recognized as incomplete. Contemporary translational research reframes DR as a multifactorial neurovascular disease involving metabolic dysregulation, oxidative stress, chronic inflammation, and neurodegeneration in addition to vascular pathology. Large-scale epidemiological studies confirm the global burden of DR, with prevalence estimates ranging from 35–40% among diabetic populations, making it a leading cause of preventable blindness in working-age adults [1]. The systemic nature of DR is underscored by evidence that metabolic and inflammatory cascades precede clinically visible vascular lesions, suggesting that early neuronal and glial dysfunction play a pivotal role in disease initiation [2].
METABOLIC AND BIOCHEMICAL PATHWAYS
Persistent hyperglycemia initiates a series of biochemical disturbances that converge on oxidative stress and mitochondrial dysfunction:
Polyol pathway activation leads to sorbitol accumulation, osmotic stress, and impaired antioxidant defenses.
Protein kinase C (PKC) signaling alters vascular permeability, promotes abnormal angiogenesis, and disrupts endothelial function.
Advanced glycation end products (AGEs) cross-link proteins, destabilize extracellular matrix integrity, and trigger pro-inflammatory signaling cascades.
Oxidative stress amplifies mitochondrial damage, leading to apoptosis of retinal neurons and breakdown of the blood-retinal barrier (BRB) [3].
These processes collectively drive BRB breakdown, neuronal apoptosis, and upregulation of angiogenic mediators, reinforcing the concept that DR is not merely a vascular complication but a systemic disease with profound neurovascular consequences.
PATHOPHYSIOLOGY BEYOND VEGF
Hypoxia-induced VEGF expression remains central to pathological neovascularization, yet VEGF inhibition alone is insufficient. Anti-VEGF therapies reduce macular edema and stabilize vision but fail to address parallel mechanisms such as systemic inflammation, lipid peroxidation, and neurosensory degeneration. Clinical evidence demonstrates inconsistent efficacy in managing macular ischemia and capillary non-perfusion (CNP), with some cohorts showing progressive widening of the foveal avascular zone (FAZ) despite therapy [4]. This paradox has driven exploration of alternative upstream and parallel pathways:
Semaphorin 3A (Sema3A): A chemorepellent molecule overexpressed during hypoxic stress that prevents physiological revascularization. While anti-VEGF agents suppress vessel growth globally, they inadvertently halt healthy vascular repair. Sema3A acts selectively, driving endothelial cells away and blocking normal vessels from repairing ischemic "dead zones" while allowing leaky, pathological neovascularization to persist. Targeting this axis can selectively restore physiological revascularization [5].
Tie2 receptor modulators: Agents preserving endothelial integrity under metabolic stress.
Inflammatory cascades: Therapies targeting macrophage recruitment and glial activation to mitigate leakage and fibrosis [6].
Together, these insights emphasize the need for next-generation therapeutics that move beyond VEGF-centric paradigms toward multi-target biologics, neuroprotective strategies, and innovative drug delivery systems.
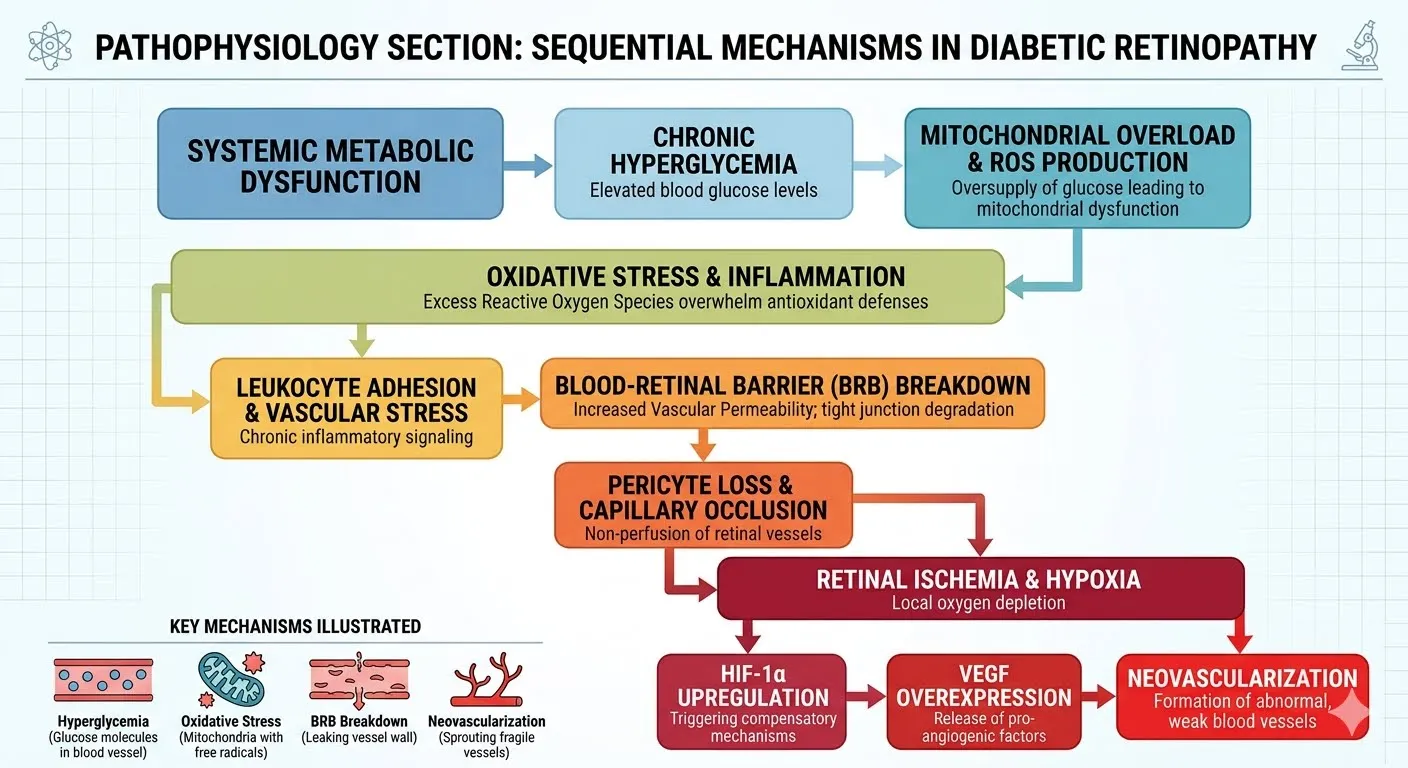
Figure 1 : Pathophysiology Beyond VEGF
METABOLIC OPTIMIZATION AND GLYCEMIC CONTROL FOR PREVENTION
The cornerstone of preventing the onset and progression of diabetic retinopathy (DR) lies in the aggressive management of systemic metabolic parameters. Chronic hyperglycemia is the primary driver of oxidative stress, mitochondrial dysfunction, and subsequent blood-retinal barrier (BRB) breakdown, ultimately leading to neural apoptosis and microvascular damage [2,3]. Large-scale clinical trials, including the Diabetes Control and Complications Trial (DCCT) and the UK Prospective Diabetes Study (UKPDS), have consistently demonstrated that intensive glycemic control significantly reduces the long-term risk of microvascular complications, including DR.
Importantly, the phenomenon of “metabolic memory”—where prior periods of poor glycemic control continue to exert deleterious effects even after normalization of HbA1c—underscores the need for early and sustained intervention [1]. Beyond glucose regulation, management of comorbid conditions such as hypertension and dyslipidemia is essential. Systemic vascular health directly influences the rate of capillary non-perfusion (CNP) and ischemic progression in the retina [4]. Achieving stable, target-range HbA1c levels, alongside optimal blood pressure and lipid control, provides a critical primary defense that complements advanced pharmacological and biological therapies currently under development.
1. The Anti-VEGF Evolution and Novel Biologics
To overcome the short intraocular half-life and limited binding affinity of first-generation agents such as ranibizumab and bevacizumab, structural engineering has yielded highly stable, multi-potent biologics.
These innovations mark a transition from monotherapy toward dual-pathway biologics and sustained-release platforms, reducing treatment burden while improving long-term outcomes.
2. Emerging Therapeutic Targets Beyond VEGF Inhibition
The Semaphorin 3A (Sema3A) Pathway
Traditionally known as an axonal guidance molecule, Sema3A plays a pathological role in retinal remodeling. Under hypoxic and hyperglycemic stress, Sema3A is overexpressed, acting as a potent chemorepellent that drives endothelial cells away, prevents physiological revascularization, and increases vascular permeability [5].
By targeting Sema3A, this therapy aims to restore physiological revascularization, potentially modifying disease course in ways traditional anti-VEGF agents cannot.
Other Molecular Targets
3. Neuroprotective and Anti-Inflammatory Strategies in Diabetic Retinopathy
Retinal neurodegeneration often precedes vascular lesions, positioning neuroprotection and anti-inflammatory modulation as complementary to vascular therapies.
Neurotrophic Support: CNTF via encapsulated cell technology offers sustained intravitreal release. Mechanism: Activates JAK/STAT, enhances mitochondrial resilience, reduces excitotoxicity. Clinical relevance: Preserves photoreceptor and ganglion cell function in early degeneration. Long-term delivery systems are currently navigating Phase II/III translational verification trials.
Anti-Inflammatory Modulation: Corticosteroid implants suppress TNF alpha, IL1 beta, and VEGF to reduce edema and neuronal stress. Non-steroidal options include minocycline (microglial inhibition), IL6 , TNF alpha antagonists, and systemic SGLT2 inhibitors.
Glutamate Excitotoxicity Control: Excess glutamate drives ganglion cell death, leading to ongoing Phase I and Phase II proof-of-concept studies of NMDA modulators like memantine and riluzole.
Oxidative Stress Mitigation: Antioxidants such as alpha-lipoic acid and N-acetylcysteine reduce ROS damage, with targeted nanocarriers being explored for optimal retinal delivery.
4. Innovative Drug Delivery Systems (DDS)
4.1 Liposomal Nanocarriers
4.2 Two-Dimensional (2D) MXenes
Platform: Transition metal carbides/nitrides.
Mechanism: High conductivity, tunable functionalization for biomolecule immobilization. Unlike passive polymer hydrogels, MXenes possess ultrathin metallic conductivity, high surface-area-to-volume ratios for smart, on-demand drug release, and intrinsic singlet oxygen/ROS scavenging capabilities that actively neutralize local oxidative stress.
Advantages: Integrated into hydrogels and microneedle patches for controlled release and wearable biomarker sensing [9].
4.3 Gene Therapy Vectors
Platform: Adeno-associated virus (AAV).
Mechanism: Induce endogenous anti-angiogenic protein production.
Advantages: Designed as a permanent “one-and-done” therapy to eliminate recurrent injection burdens. Investigational assets are currently entering early-stage Phase I/II human trials to confirm sustained safety and long-term expression profiles.
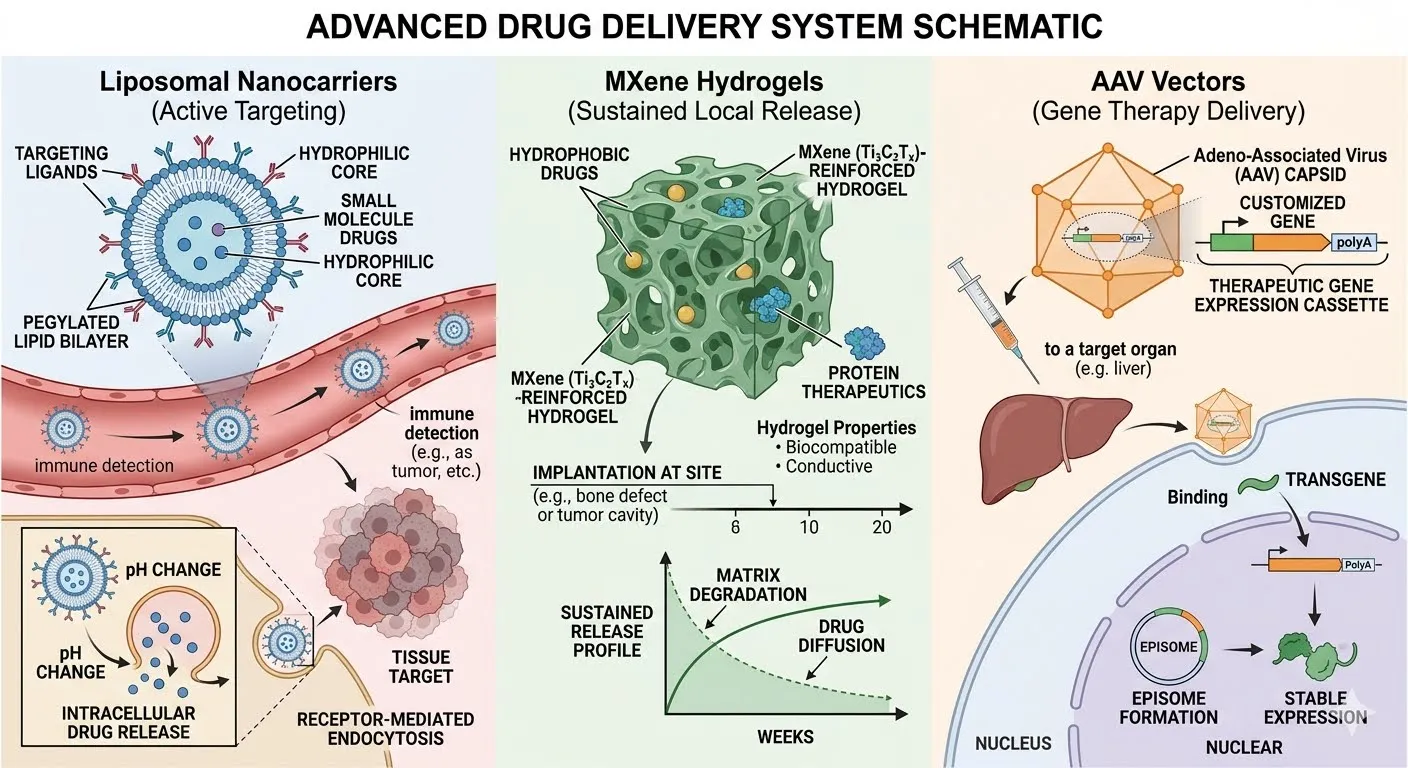
Figure 2: Innovative Drug Delivery Systems (DDS)
5. Translational Research and Future Directions
The therapeutic evolution of diabetic retinopathy is increasingly supported by diagnostic innovation and predictive analytics, forming translational bridges between laboratory advances and clinical practice.
Advanced Imaging Modalities
Ultra-widefield optical coherence tomography angiography (UWF-OCTA) has emerged as a pivotal tool for quantifying peripheral capillary non-perfusion (CNP) and foveal avascular zone (FAZ) distortion with unprecedented precision [10]. Unlike conventional OCT, UWF-OCTA captures peripheral ischemic zones that often precede central vision loss, enabling earlier detection of disease progression and more accurate monitoring of therapeutic response.
Artificial Intelligence Integration
Artificial intelligence (AI) models are now being integrated into multimodal frameworks that combine fundus imaging, OCTA metrics, and electronic health records (EHRs). These systems achieve screening AUCs exceeding 97%, offering high-accuracy risk stratification [11]. Importantly, AI-driven analytics can identify patients most likely to benefit from neuroprotective or non-VEGF therapies, allowing intervention before irreversible microvascular destruction occurs.
Predictive and Personalized Medicine
The convergence of imaging and AI heralds a shift toward precision ophthalmology. Predictive algorithms not only stratify risk but also guide therapeutic selection—whether anti-VEGF, anti-Sema3A, or neuroprotective implants—based on individualized disease profiles. This personalization reduces overtreatment, optimizes resource allocation, and enhances patient outcomes.
Future Outlook
By 2030, translational research is expected to integrate:
FDA-Approved Treatment Strategies and Clinical Usage
Modern management of diabetic retinopathy (DR) and diabetic macular edema (DME) has shifted from surgical interventions such as pan-retinal photocoagulation (PRP) and pars plana vitrectomy (PPV) toward molecularly targeted pharmacotherapies. First-generation anti-VEGF monotherapies like ranibizumab and aflibercept demonstrated efficacy in stabilizing the blood-retinal barrier, but their frequent dosing schedules imposed a significant treatment burden.
Recent clinical trials have established more durable innovations. The YOSEMITE and RHINE Phase 3 trials confirmed that faricimab, a bispecific antibody targeting VEGF-A and Angiopoietin-2, can safely extend dosing intervals up to 16 weeks while maintaining efficacy in DME patients [12]. Similarly, the PHOTON trial demonstrated that high-dose aflibercept (8 mg) provides intensified VEGF suppression with extended durability compared to standard 2 mg dosing [13].
Earlier pivotal studies such as VISTA and VIVID validated aflibercept’s long-term efficacy in DME, showing sustained anatomical and functional benefits over 148 weeks [14]. To further reduce injection frequency, the Susvimo port delivery system for ranibizumab was developed, offering continuous intraocular release with refills required only every nine months, as outlined in the PAGODA and PAVILION Phase 3 designs [15].
For patients with refractory inflammation or pseudophakia, intravitreal corticosteroid implants remain valuable adjuncts. The fluocinolone acetonide implant (Iluvien) provides sustained steroid release for up to 36 months, offering a “one-and-done” therapeutic profile validated in long-term studies [16].
Together, these FDA-approved strategies represent a paradigm shift toward durable, multi-pathway interventions that reduce treatment burden while improving long-term visual outcomes.
|
Therapeutic Class |
Drug / Intervention |
FDA-Approved Indication(s) for DR/DME |
Standard Clinical Usage & Dosing Regimen |
|
1.First-Generation Anti-VEGF Monotherapy |
Ranibizumab (Lucentis 0.3 mg) |
All forms of Diabetic Retinopathy (with or without DME); Diabetic Macular Edema. |
Administered via monthly (every 4 weeks) intravitreal injection. Often transitioned to a customized "treat-and-extend" protocol in stabilized patients. |
|
Next-Generation Anti-VEGF / VEGF Traps |
Aflibercept (Eylea 2 mg) |
Diabetic Retinopathy; Diabetic Macular Edema. |
Typically initiated with 5 monthly loading doses, followed by maintenance injections every 8 weeks (2 months). Can be dosed flexibly based on anatomical response |
|
|
High-Dose Aflibercept (Eylea HD 8 mg) |
Diabetic Retinopathy; Diabetic Macular Edema |
Initiated with 3 monthly loading doses, followed by extended maintenance intervals of every 12 to 16 weeks, drastically reducing injection frequency. |
|
Dual-Pathway Bispecific Biologics |
Faricimab (Vabysmo 6 mg) |
Diabetic Macular Edema. |
Simultaneously inhibits VEGF-A and Angiopoietin-2 (Ang-2). Initiated with 4 monthly loading doses; maintenance intervals can be extended up to every 16 weeks based on OCT monitoring. |
|
Sustained-Release Port Delivery Platforms |
Sustained-Release Ranibizumab (Susvimo 100 mg/mL) |
Diabetic Retinopathy (without center-involved DME) |
A refillable eye implant surgically placed via a one-time outpatient procedure. Delivers continuous ranibizumab with scheduled clinical refills required only once every 9 months |
|
Intravitreal Corticosteroids |
Dexamethasone Implant (Ozurdex 0.7 mg) |
Diabetic Macular Edema. |
Biodegradable intravitreal implant providing sustained steroid release over several months. Primarily used for anti-VEGF refractory cases or pseudophakic patients. |
|
|
Fluocinolone Acetonide Implant (Iluvien 0.19 mg) |
Diabetic Macular Edema (in patients previously treated with a course of corticosteroids without a significant rise in IOP) |
Non-biodegradable intravitreal implant providing low-dose micro-hydration steroid release for up to 36 months ("one-and-done" profile for macular swelling). |
|
Conventional Surgical / Laser Options |
Pan-retinal Photocoagulation (PRP) / Focal Laser |
Proliferative Diabetic Retinopathy (PDR) and clinically significant DME. |
Non-pharmacological thermal laser ablation targeting ischemic peripheral retina (PRP) to halt neovascularization, or micro-pulsed/focal laser targeting leaking microaneurysms. |
|
|
Pars Plana Vitrectomy (PPV) |
Advanced Proliferative DR complications (e.g., non-clearing vitreous hemorrhage, tractional retinal detachment). |
Surgical removal of the vitreous gel, clearance of intraocular blood, and mechanical segmentation of fibrovascular membranes to restore anatomical structure. |
CONCLUSION
Diabetic retinopathy (DR) is no longer viewed solely as a microvascular complication of diabetes but as a multifactorial neurovascular disease driven by metabolic dysregulation, oxidative stress, inflammation, and neurodegeneration. While conventional therapies such as pan-retinal photocoagulation and anti-VEGF agents have transformed outcomes in proliferative DR and diabetic macular edema, their limitations—including incomplete efficacy, injection burden, and inability to address upstream pathways—necessitate a paradigm shift.
Recent advances highlight the promise of multi-target biologics (e.g., Faricimab, high-dose aflibercept), non-VEGF therapies (e.g., anti-Sema3A monoclonal antibodies, Tie2 modulators), and neuroprotective strategies (CNTF delivery, corticosteroid implants) in addressing both vascular and neuronal dimensions of DR. Complementing these pharmacological innovations are bioengineered drug delivery systems—liposomal nanocarriers, MXene-based hydrogels, and gene therapy vectors—that aim to reduce treatment burden and provide sustained intraocular therapeutic levels.
Equally transformative is the integration of advanced imaging modalities such as ultra-widefield OCT angiography and AI-driven predictive analytics, which enable precise quantification of ischemia, early risk stratification, and personalized therapeutic selection. Together, these translational bridges are reshaping DR management into a precision medicine model, where interventions are tailored to individual disease profiles and initiated before irreversible microvascular destruction occurs.
Looking ahead, the convergence of biologics, innovative delivery platforms, and AI-guided diagnostics offers the potential to redefine DR care by 2030. However, critical challenges remain: ensuring cost-effectiveness, accessibility in low-resource settings, and regulatory approval pathways for novel therapies and AI systems. Addressing these barriers will be essential to translate scientific breakthroughs into equitable global practice.
In summary, the future of DR management lies in a multidimensional approach that integrates systemic metabolic control, advanced pharmacology, bioengineering, and predictive diagnostics. Such a strategy holds the promise not only of preserving vision but of fundamentally altering the natural history of diabetic retinopathy.
REFERENCES

Akshay Gali*, Recent Advances In The Treatment, Emerging Therapies, And Innovative Drug Delivery Systems For Diabetic Retinopathy: A Narrative Review, Int. J. Sci. R. Tech., 2026, 3 (6), 1238-1246. https://doi.org/10.5281/zenodo.20796427
 10.5281/zenodo.20796427
10.5281/zenodo.20796427