
We use cookies to ensure our website works properly and to personalise your experience. Cookies policy
Department of Pharmacy, Shri Ram College of Pharmacy, Muzaffarnagar, Uttar Pradesh, India
Insomnia is one of the most prevalent sleep disorders and has emerged as a major public health concern owing to its growing prevalence and substantial impact on physical health, mental well-being, cognitive performance, and quality of life. Increasing evidence suggests that insomnia is not merely a symptom secondary to other medical or psychiatric conditions but a distinct clinical disorder characterized by persistent sleep disturbance and daytime functional impairment. Rapid advances in sleep neuroscience have significantly improved the understanding of the neurobiological mechanisms underlying insomnia, including hyperarousal, circadian rhythm dysregulation, and alterations in neurotransmitter systems. Simultaneously, evolving diagnostic criteria and the development of novel therapeutic approaches have transformed the clinical management of this disorder. This review critically summarizes the contemporary evidence on the epidemiology, classification, pathophysiology, risk factors, clinical presentation, diagnostic evaluation, associated comorbidities, and current treatment strategies for insomnia. Particular emphasis is placed on evidence supporting cognitive behavioral therapy for insomnia (CBT-I), conventional pharmacological agents, emerging orexin receptor antagonists, and digital therapeutic interventions. Recent advances, ongoing challenges, and future perspectives in insomnia research are also discussed to provide a comprehensive overview of the evolving landscape of sleep medicine. By integrating findings from recent clinical studies, systematic reviews, and international guidelines, this review aims to provide clinicians, pharmacists, researchers, and healthcare professionals with an updated evidence-based resource to support informed clinical decision-making and encourage future research in insomnia management.
Sleep is a fundamental biological process that is essential for maintaining physical health, cognitive performance, emotional well-being, and overall quality of life. Adequate sleep plays a vital role in memory consolidation, immune regulation, metabolic homeostasis, hormonal balance, and tissue repair. Conversely, persistent disturbances in sleep can adversely affect nearly every organ system, contributing to impaired daytime functioning and an increased risk of chronic diseases. Among the various sleep disorders, insomnia is the most prevalent and clinically significant condition encountered in healthcare settings.
Insomnia is characterized by persistent difficulty in initiating sleep, maintaining sleep, or experiencing restorative sleep despite adequate opportunity and appropriate circumstances for sleep. These nocturnal symptoms are accompanied by daytime consequences such as fatigue, impaired attention, reduced work or academic performance, mood disturbances, and diminished quality of life. Although transient insomnia may occur in response to acute stress or environmental changes, chronic insomnia is a persistent disorder that requires comprehensive clinical evaluation and evidence-based management.
Over the past two decades, the understanding of insomnia has evolved considerably. Earlier, insomnia was frequently regarded as a secondary symptom of medical, neurological, or psychiatric illnesses. Contemporary evidence, however, recognizes insomnia as an independent clinical disorder with complex interactions among neurobiological, psychological, behavioral, and environmental factors. The current conceptual framework emphasizes persistent hyperarousal, dysregulation of the sleep–wake regulatory system, circadian rhythm disturbances, cognitive dysfunction, and maladaptive sleep-related behaviors as key mechanisms contributing to the development and maintenance of chronic insomnia.
The burden of insomnia extends far beyond sleep disturbance alone. Individuals with persistent insomnia often experience impaired cognitive function, emotional instability, reduced occupational productivity, and decreased social functioning. In addition, insomnia commonly coexists with psychiatric disorders such as anxiety and depression, as well as chronic medical conditions including cardiovascular disease, diabetes mellitus, chronic pain syndromes, respiratory disorders, and neurodegenerative diseases. This bidirectional relationship highlights the importance of recognizing insomnia as both a potential consequence and a contributing factor in multiple chronic health conditions.
Advances in sleep medicine have substantially improved the understanding of the neurobiology of insomnia. Research has identified the involvement of several neurotransmitter systems, including gamma-aminobutyric acid (GABA), glutamate, serotonin, dopamine, norepinephrine, histamine, melatonin, adenosine, and orexin, in regulating the sleep–wake cycle. Furthermore, alterations in the hypothalamic–pituitary–adrenal axis, increased sympathetic nervous system activity, and circadian rhythm disruption have been implicated in the pathophysiology of chronic insomnia. These discoveries have facilitated the development of novel therapeutic approaches targeting specific biological pathways.
Management strategies for insomnia have also undergone significant transformation. Cognitive Behavioral Therapy for Insomnia (CBT-I) is now widely recommended as the first-line treatment for chronic insomnia because of its sustained clinical benefits and favorable safety profile. Pharmacological interventions remain valuable in selected patients when carefully individualized according to symptom severity, comorbidities, and treatment objectives. More recently, the introduction of dual orexin receptor antagonists, digital CBT-I platforms, and personalized therapeutic approaches has expanded the range of evidence-based treatment options available to clinicians.
Given the increasing prevalence of insomnia and its substantial impact on individual and public health, an updated synthesis of current scientific evidence is essential. This review critically examines the contemporary literature on the epidemiology, classification, pathophysiological mechanisms, clinical presentation, diagnostic evaluation, associated comorbidities, and current management of insomnia. In addition, recent advances in pharmacological and non-pharmacological therapies, emerging research trends, and future perspectives are discussed to provide clinicians, pharmacists, researchers, and healthcare professionals with a comprehensive evidence-based understanding of this complex sleep disorder.
2. EPIDEMIOLOGY OF INSOMNIA
Insomnia is one of the most common sleep disorders and represents a growing public health challenge worldwide. It affects individuals of all ages and socioeconomic backgrounds, although its prevalence varies according to the diagnostic criteria used, study population, and geographical region. While occasional sleep disturbances are experienced by many individuals during periods of stress or illness, persistent insomnia is associated with significant impairment in physical, psychological, social, and occupational functioning.
The occurrence of insomnia increases with age and is reported more frequently in women than in men. Hormonal changes, pregnancy, menopause, and a higher prevalence of anxiety and depressive disorders are among the factors that contribute to the increased susceptibility of women to insomnia. In older adults, age-related changes in sleep architecture, multiple chronic medical conditions, polypharmacy, and reduced circadian rhythm stability further increase the risk of developing chronic insomnia.
The prevalence of insomnia is also influenced by lifestyle and occupational factors. Shift workers, healthcare professionals, students, military personnel, and individuals working irregular schedules are at greater risk because of circadian rhythm disruption and prolonged exposure to psychological stress. Modern lifestyle habits, including excessive screen time, prolonged use of electronic devices before bedtime, irregular sleep schedules, high caffeine consumption, and reduced physical activity, have further contributed to the increasing burden of sleep disturbances across different populations.
Several medical and psychiatric disorders are strongly associated with insomnia. Individuals with depression, anxiety disorders, chronic pain, cardiovascular diseases, respiratory disorders, neurodegenerative diseases, diabetes mellitus, and substance use disorders frequently report sleep disturbances. The relationship is often bidirectional, where insomnia may increase the risk of developing these conditions, while these disorders can also contribute to the onset and persistence of insomnia. This complex interaction highlights the importance of early recognition and comprehensive management.
Beyond its clinical consequences, insomnia imposes a considerable socioeconomic burden. Persistent sleep disturbances are associated with reduced workplace productivity, increased absenteeism, impaired academic performance, occupational and road traffic accidents, and increased healthcare utilization. The economic impact extends beyond direct medical costs and includes substantial indirect costs related to loss of productivity and long-term disability. Consequently, insomnia has become an important public health issue requiring greater awareness, timely diagnosis, and evidence-based intervention.
Overall, the epidemiological evidence underscores that insomnia is not merely an isolated sleep complaint but a common chronic disorder with wide-ranging health, social, and economic implications. Understanding its distribution and associated risk factors is essential for developing effective preventive strategies and improving patient outcomes.
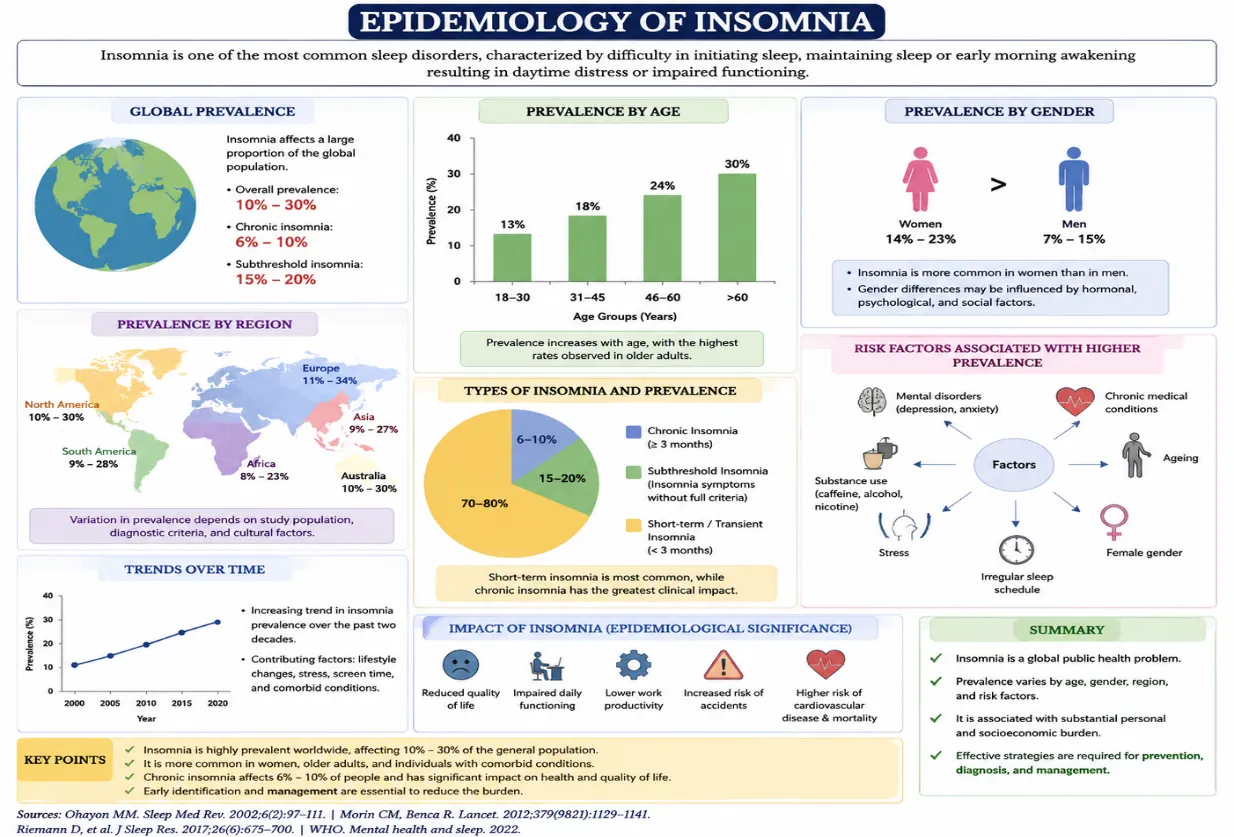
Figure 1 Epidemiology of Insomnia
3. CLASSIFICATION OF INSOMNIA
Insomnia is a heterogeneous sleep disorder with diverse clinical presentations, durations, and underlying causes. A clear classification is essential for accurate diagnosis, appropriate treatment selection, and improved patient outcomes. Contemporary classification systems recognize insomnia as a disorder that may occur independently or coexist with other medical, psychiatric, or sleep-related conditions. The two most widely accepted classification systems are the International Classification of Sleep Disorders, Third Edition, Text Revision (ICSD-3-TR) and the Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition, Text Revision (DSM-5-TR).
Based on the duration of symptoms, insomnia is commonly categorized as short-term (acute) or chronic. Short-term insomnia typically develops in response to identifiable stressors such as illness, emotional distress, travel, or major life events and generally resolves once the precipitating factor subsides. In contrast, chronic insomnia is characterized by persistent sleep disturbances occurring on a regular basis for an extended period and is often maintained by a combination of biological, psychological, and behavioral factors. Chronic insomnia usually requires structured clinical evaluation and evidence-based interventions.
From an etiological perspective, insomnia may be associated with medical disorders, psychiatric illnesses, medication use, substance consumption, circadian rhythm disturbances, or environmental factors. However, current diagnostic frameworks emphasize that chronic insomnia should be considered a distinct clinical disorder even when it coexists with other health conditions, as effective treatment of insomnia may improve overall health outcomes and quality of life.
Clinically, insomnia may present as difficulty initiating sleep (sleep-onset insomnia), difficulty maintaining sleep with frequent awakenings (sleep-maintenance insomnia), or early morning awakening with an inability to return to sleep. Many patients experience a combination of these symptoms, highlighting the multifaceted nature of the disorder.
The ICSD-3-TR classifies insomnia primarily into chronic insomnia disorder, short-term insomnia disorder, and other insomnia disorder, while the DSM-5-TR defines insomnia disorder based on persistent sleep complaints associated with clinically significant daytime impairment. Although these systems differ slightly in terminology, both emphasize symptom persistence, adequate opportunity for sleep, and the exclusion of insufficient sleep as the primary cause of symptoms.
Recognizing the specific type and underlying contributors to insomnia is fundamental for selecting appropriate therapeutic strategies, predicting prognosis, and preventing long-term complications.
|
Basis of Classification |
Type |
Key Characteristics |
|
Duration |
Short-term (Acute) Insomnia |
Usually lasts for a limited period, commonly associated with temporary stress, illness, or environmental changes. |
|
Chronic Insomnia |
Persistent sleep disturbance occurring regularly over an extended duration and associated with daytime impairment. |
|
|
Clinical Presentation |
Sleep-Onset Insomnia |
Difficulty initiating sleep at bedtime. |
|
Sleep-Maintenance Insomnia |
Frequent awakenings or difficulty maintaining sleep throughout the night. |
|
|
Early Morning Awakening Insomnia |
Awakening earlier than desired with inability to resume sleep. |
|
|
Etiology |
Primary (Independent) Insomnia |
Sleep disturbance not directly attributable to another identifiable disorder. |
|
Secondary/Associated Insomnia |
Occurs in association with medical illnesses, psychiatric disorders, medications, or substance use. |
|
|
ICSD-3-TR |
Chronic Insomnia Disorder |
Persistent insomnia with significant daytime consequences requiring clinical management. |
|
Short-Term Insomnia Disorder |
Temporary insomnia related to identifiable stressors or acute conditions. |
|
|
Other Insomnia Disorder |
Sleep complaints not fulfilling the complete diagnostic criteria for the above categories. |
Abbreviations: ICSD-3-TR, International Classification of Sleep Disorders, Third Edition, Text Revision; DSM-5-TR, Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition, Text Revision.
Table 1. Classification of Insomnia
4. PATHOPHYSIOLOGY OF INSOMNIA
Insomnia is a complex disorder resulting from the interaction of neurobiological, psychological, behavioral, and environmental factors. Rather than being caused by a single abnormality, chronic insomnia is now understood as a disorder of persistent hyperarousal, in which the brain and body remain in an increased state of activation during both wakefulness and sleep. This state interferes with normal sleep initiation, sleep maintenance, and the restorative functions of sleep
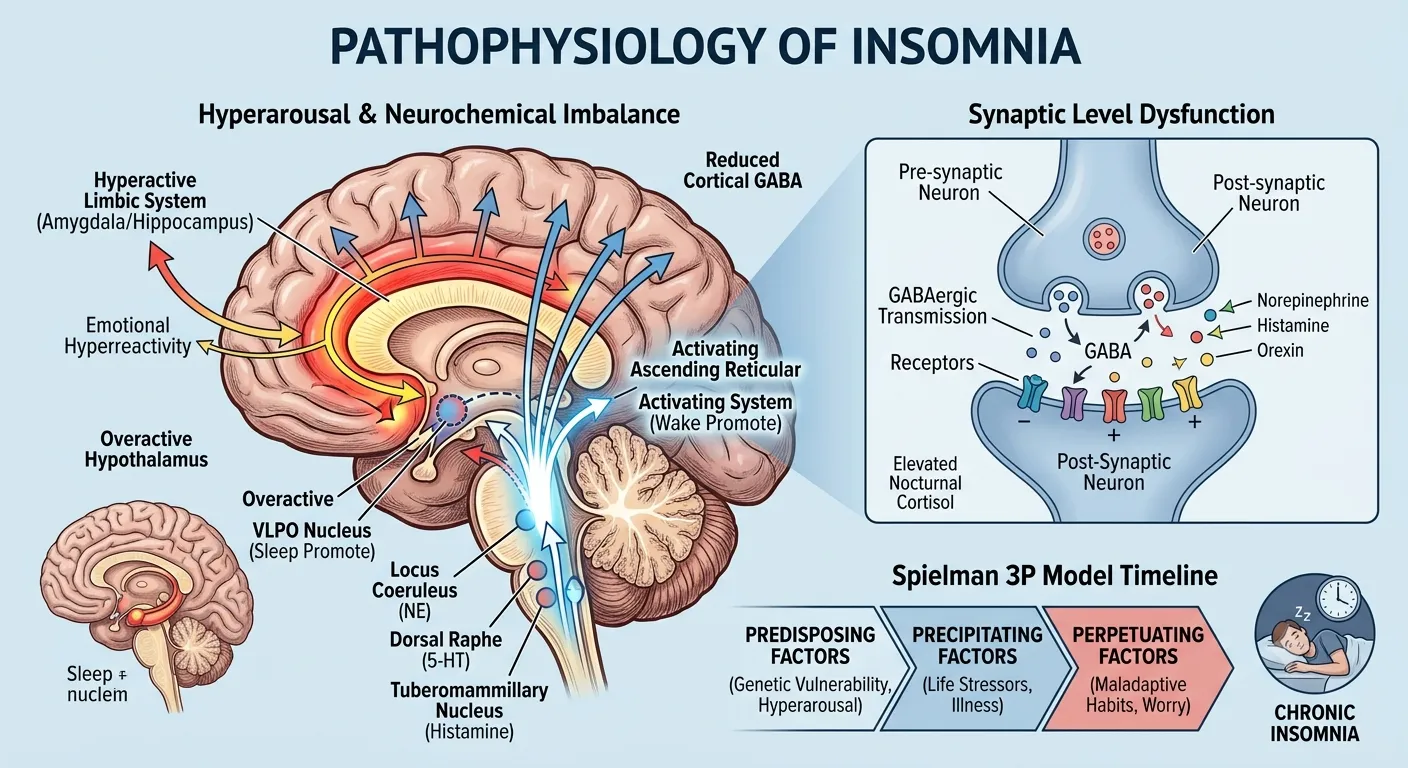
Figure 2: Pathophysiology of Insomnia
4.1 Hyperarousal Theory
The hyperarousal model is the most widely accepted explanation for chronic insomnia. Individuals with insomnia often exhibit increased physiological, cognitive, and emotional arousal that persists throughout the day and night. Excessive worrying, heightened stress responses, increased sympathetic nervous system activity, and elevated metabolic activity in the brain contribute to difficulty falling asleep and frequent nocturnal awakenings. Neuroimaging studies have demonstrated that certain brain regions remain more active during sleep in individuals with chronic insomnia than in healthy sleepers, supporting the concept of continuous central nervous system hyperactivation.
4.2 Neurotransmitter Dysregulation
Normal sleep depends on a delicate balance between sleep-promoting and wake-promoting neurotransmitters. Disruption of this balance plays a central role in the development of insomnia.
The inhibitory neurotransmitter γ-aminobutyric acid (GABA) promotes sleep by suppressing neuronal excitability. Reduced GABAergic activity may contribute to increased cortical arousal and impaired sleep initiation. In contrast, wake-promoting neurotransmitters such as orexin (hypocretin), norepinephrine, dopamine, histamine, and acetylcholine maintain alertness and wakefulness. Excessive activation of these systems may prolong wakefulness and fragment sleep.
Other neurotransmitters, including serotonin, melatonin, glutamate, and adenosine, also participate in regulating the sleep–wake cycle. Alterations in their physiological functions may further impair sleep continuity and circadian regulation.
4.3 Circadian Rhythm Dysregulation
The circadian rhythm is regulated by the suprachiasmatic nucleus (SCN) of the hypothalamus, which synchronizes the sleep–wake cycle with the external light–dark environment. Disruption of circadian timing due to shift work, jet lag, irregular sleep schedules, or excessive evening exposure to artificial light may delay sleep onset and reduce sleep quality. Altered melatonin secretion further contributes to circadian misalignment and chronic sleep disturbances.
4.4 Hypothalamic–Pituitary–Adrenal (HPA) Axis Activation
Psychological stress is an important precipitating factor for insomnia. Persistent activation of the HPA axis increases the secretion of cortisol and stimulates sympathetic nervous system activity. Elevated nighttime cortisol levels may interfere with normal sleep initiation, reduce slow-wave sleep, and promote repeated awakenings during the night. Sustained HPA axis activation is considered one of the biological mechanisms responsible for maintaining chronic insomnia.
4.5 Cognitive and Behavioral Mechanisms
Maladaptive cognitive processes play an important role in perpetuating insomnia. Many individuals develop excessive concern about sleep, unrealistic expectations regarding sleep duration, and anxiety related to the consequences of poor sleep. These negative beliefs increase emotional arousal and create a cycle in which attempts to sleep paradoxically make sleep more difficult.
Behavioral factors such as irregular bedtime schedules, prolonged daytime napping, excessive caffeine intake, nighttime screen exposure, and spending excessive time awake in bed further reinforce chronic insomnia by disrupting normal sleep regulation.
4.6 The 3P Model of Insomnia
The 3P Model, proposed by Arthur Spielman, provides a useful framework for understanding the development and persistence of insomnia. According to this model, insomnia results from the interaction of:
Initially, insomnia is triggered by precipitating events; however, perpetuating factors often maintain the disorder even after the original stressor has resolved.
|
Mechanism |
Underlying Changes |
Clinical Significance |
|
Hyperarousal |
Persistent physiological and cognitive activation |
Difficulty initiating and maintaining sleep |
|
Neurotransmitter imbalance |
Reduced sleep-promoting activity and increased wake-promoting signaling |
Sleep fragmentation and prolonged wakefulness |
|
Circadian rhythm disruption |
Misalignment of the biological clock with the sleep schedule |
Delayed sleep onset and poor sleep quality |
|
HPA axis activation |
Increased cortisol secretion and sympathetic activity |
Stress-related insomnia and reduced restorative sleep |
|
Cognitive dysfunction |
Excessive worry, rumination, and sleep-related anxiety |
Persistence and recurrence of chronic insomnia |
|
Behavioral factors |
Poor sleep hygiene, irregular sleep schedule, excessive screen exposure |
Maintenance of chronic insomnia despite resolution of initial triggers |
Table 2. Major Pathophysiological Mechanisms of Insomnia
5. RISK FACTORS FOR INSOMNIA
Insomnia is a multifactorial disorder that develops through the interaction of biological, psychological, behavioral, environmental, and medical factors. Although transient sleep disturbances may occur in response to temporary stressors, persistent exposure to multiple risk factors substantially increases the likelihood of developing chronic insomnia. Identification of these factors is essential for early intervention, prevention, and individualized treatment planning.
5.1 Biological Factors
Several biological characteristics influence an individual's susceptibility to insomnia. Increasing age is associated with alterations in sleep architecture, including reduced slow-wave sleep, frequent nocturnal awakenings, and decreased sleep efficiency. Women are more frequently affected than men, partly because of hormonal fluctuations during the menstrual cycle, pregnancy, postpartum period, and menopause. Genetic predisposition has also been implicated, suggesting that inherited variations in sleep regulation and stress responsiveness may contribute to insomnia in susceptible individuals.
5.2 Psychological Factors
Psychological conditions are among the strongest contributors to insomnia. Persistent stress, anxiety, depression, excessive worrying, emotional distress, and maladaptive coping mechanisms commonly interfere with normal sleep. Individuals who exhibit heightened emotional reactivity or cognitive hyperarousal often experience difficulty initiating or maintaining sleep. Negative beliefs about sleep and fear of not sleeping may further perpetuate the disorder.
5.3 Lifestyle and Behavioral Factors
Modern lifestyle habits have significantly contributed to the increasing prevalence of insomnia. Irregular sleep schedules, prolonged exposure to electronic devices before bedtime, excessive caffeine or nicotine consumption, inadequate physical activity, and daytime napping may disrupt normal sleep regulation. Poor sleep hygiene, such as using the bed for work or entertainment, inconsistent bedtime routines, and sleeping in unsuitable environments, further increases the risk of chronic insomnia.
5.4 Medical and Psychiatric Disorders
Numerous medical conditions are associated with insomnia. Chronic pain disorders, cardiovascular diseases, respiratory illnesses, gastroesophageal reflux disease, endocrine disorders, neurological diseases, and cancer frequently impair sleep quality. Psychiatric disorders, particularly anxiety disorders, depression, bipolar disorder, post-traumatic stress disorder, and substance use disorders, are strongly associated with persistent insomnia. The relationship is often bidirectional, with each condition potentially exacerbating the other.
5.5 Medication- and Substance-Related Factors
Several medications may contribute to sleep disturbances as an adverse effect. Stimulants, corticosteroids, certain antidepressants, decongestants, and some bronchodilators may interfere with sleep initiation or maintenance. Excessive consumption of caffeine, nicotine, alcohol, and recreational substances may also disrupt normal sleep architecture and reduce overall sleep quality.
5.6 Environmental and Occupational Factors
Environmental conditions significantly influence sleep quality. Excessive noise, bright light, uncomfortable room temperature, and unsuitable sleeping environments may impair sleep continuity. Occupational factors such as rotating shift work, night duty, frequent international travel, and irregular working hours disrupt circadian rhythm synchronization and increase the likelihood of insomnia. Healthcare professionals, emergency workers, and shift-based employees are particularly vulnerable because of repeated circadian misalignment.
The coexistence of multiple risk factors substantially increases the probability of developing chronic insomnia. Consequently, a comprehensive clinical assessment should include evaluation of biological characteristics, psychological health, lifestyle habits, medical conditions, medication history, and environmental influences to facilitate individualized management and improve long-term treatment outcomes.
|
Category |
Risk Factors |
Potential Impact on Sleep |
|
Biological |
Advanced age, female sex, genetic predisposition |
Altered sleep architecture and increased susceptibility to insomnia |
|
Psychological |
Stress, anxiety, depression, excessive worry, emotional distress |
Increased cognitive and physiological arousal |
|
Lifestyle & Behavioral |
Irregular sleep schedule, excessive screen time, poor sleep hygiene, caffeine, nicotine, daytime naps |
Delayed sleep onset and fragmented sleep |
|
Medical Conditions |
Chronic pain, cardiovascular disease, diabetes, respiratory disorders, neurological disorders |
Sleep disruption secondary to underlying illness |
|
Psychiatric Disorders |
Anxiety disorders, depression, bipolar disorder, PTSD, substance use disorders |
Persistent insomnia with significant daytime impairment |
|
Medications & Substances |
Corticosteroids, stimulants, bronchodilators, alcohol, caffeine, nicotine |
Reduced sleep quality and disturbed sleep continuity |
|
Environmental & Occupational |
Noise, excessive light, uncomfortable temperature, shift work, jet lag |
Circadian rhythm disruption and poor sleep quality |
Table 3. Major Risk Factors Associated with Insomnia
6. CLINICAL MANIFESTATIONS OF INSOMNIA
The clinical presentation of insomnia extends beyond disturbed nocturnal sleep and encompasses a broad spectrum of daytime impairments that significantly affect an individual's physical, cognitive, emotional, and social functioning. Although the severity and pattern of symptoms vary among patients, persistent sleep disturbance accompanied by daytime consequences remains the hallmark of insomnia disorder.
6.1 Night-Time Symptoms
The primary symptoms of insomnia occur during the sleep period. Patients commonly report difficulty initiating sleep despite adequate opportunity to sleep, prolonged sleep latency, frequent nocturnal awakenings, difficulty returning to sleep after awakening, or waking earlier than intended. Many individuals also describe their sleep as light, fragmented, or non-restorative, even when the total sleep duration appears adequate.
The pattern of sleep disturbance may differ among individuals. Some patients predominantly experience difficulty falling asleep (sleep-onset insomnia), whereas others report repeated awakenings during the night (sleep-maintenance insomnia) or persistent early morning awakening. In chronic insomnia, these symptoms often occur several nights each week and may persist for months or years if left untreated.
6.2 Daytime Consequences
The effects of insomnia extend well beyond the nighttime period. Inadequate or poor-quality sleep frequently results in excessive daytime fatigue, reduced energy levels, impaired concentration, memory difficulties, decreased attention, and slower cognitive processing. These impairments may adversely affect academic performance, occupational productivity, and decision-making abilities.
Emotional disturbances are also common. Patients with insomnia frequently experience irritability, mood fluctuations, anxiety, frustration, and reduced stress tolerance. Persistent insomnia may contribute to the development or worsening of depressive symptoms and other mental health conditions.
6.3 Functional and Social Impact
Chronic insomnia significantly affects daily functioning and overall quality of life. Individuals often report reduced work efficiency, increased absenteeism, impaired interpersonal relationships, and decreased participation in social and recreational activities. Sleep deprivation also increases the risk of workplace errors, motor vehicle accidents, and occupational injuries because of impaired alertness and delayed reaction time.
In addition to its psychosocial consequences, chronic insomnia has been associated with adverse physical health outcomes, including impaired immune function, increased cardiovascular risk, metabolic disturbances, and reduced overall well-being. These widespread effects emphasize that insomnia should be recognized as a disorder affecting multiple dimensions of health rather than merely a complaint of poor sleep.
Timely recognition of both nocturnal and daytime symptoms is essential for accurate diagnosis, assessment of disease severity, and selection of appropriate therapeutic interventions.
|
Domain |
Clinical Manifestations |
Clinical Significance |
|
Night-Time Symptoms |
Difficulty initiating sleep |
Increased sleep latency |
|
Frequent nocturnal awakenings |
Fragmented sleep |
|
|
Difficulty returning to sleep |
Reduced sleep continuity |
|
|
Early morning awakening |
Shortened total sleep duration |
|
|
Non-restorative or poor-quality sleep |
Feeling unrefreshed after waking |
|
|
Daytime Symptoms |
Fatigue and low energy |
Reduced physical performance |
|
Excessive daytime sleepiness or tiredness |
Impaired daily functioning |
|
|
Poor concentration and memory |
Reduced academic and occupational performance |
|
|
Irritability, anxiety, mood disturbances |
Emotional instability |
|
|
Reduced productivity |
Impaired work efficiency |
|
|
Increased accident risk |
Decreased alertness and slower reaction time |
|
|
Long-Term Consequences |
Reduced quality of life |
Chronic functional impairment |
|
Increased healthcare utilization |
Greater clinical and economic burden |
Table 4. Clinical Manifestations of Insomnia
7. DIAGNOSIS OF INSOMNIA
Accurate diagnosis of insomnia is essential for identifying the underlying causes of sleep disturbance, distinguishing insomnia from other sleep disorders, and selecting appropriate treatment strategies. The diagnosis is primarily clinical and is based on a detailed sleep history, assessment of daytime impairment, and evaluation of contributing medical, psychiatric, behavioral, and environmental factors. Laboratory investigations are not routinely required unless another sleep disorder or underlying medical condition is suspected.
7.1 Clinical Assessment
A comprehensive clinical assessment is the cornerstone of insomnia diagnosis. The evaluation should include the onset, duration, frequency, and severity of sleep complaints, together with information regarding bedtime habits, sleep schedule, lifestyle factors, medication use, caffeine and alcohol intake, occupational history, and psychosocial stressors. Particular attention should be paid to the presence of daytime symptoms such as fatigue, impaired concentration, irritability, mood changes, and reduced work or academic performance.
Healthcare professionals should also screen for medical disorders, psychiatric illnesses, chronic pain, neurological diseases, respiratory disorders, and other sleep disorders that may contribute to insomnia or mimic its symptoms.
7.2 Diagnostic Criteria
The diagnosis of chronic insomnia is generally based on internationally accepted criteria. According to current clinical recommendations, insomnia is characterized by persistent difficulty in sleep initiation, sleep maintenance, or early morning awakening despite adequate opportunity for sleep, accompanied by significant daytime impairment. Symptoms should occur regularly over a prolonged period and should not be better explained by another untreated sleep disorder, substance use, or an underlying medical condition.
7.3 Sleep History and Sleep Diary
A detailed sleep history provides valuable information regarding sleep patterns and potential precipitating factors. Patients are often encouraged to maintain a sleep diary for one to two weeks, recording bedtime, wake-up time, sleep latency, nocturnal awakenings, total sleep duration, daytime naps, and factors that may influence sleep. Sleep diaries are inexpensive, non-invasive, and useful for monitoring treatment response.
7.4 Standardized Assessment Tools
Several validated questionnaires assist in evaluating insomnia severity and its impact on daily functioning.
These instruments complement, but do not replace, a comprehensive clinical assessment.
7.5 Actigraphy
Actigraphy involves the use of a wrist-worn device that continuously records body movements over several days or weeks. It provides objective information regarding sleep–wake patterns, sleep duration, and circadian rhythm disturbances in the patient's usual environment. Actigraphy is particularly useful in patients with irregular sleep schedules or suspected circadian rhythm sleep–wake disorders.
7.6 Polysomnography (PSG)
Polysomnography is the gold standard investigation for many sleep disorders; however, it is not routinely indicated for uncomplicated chronic insomnia. It is recommended when conditions such as obstructive sleep apnea, periodic limb movement disorder, parasomnias, or other complex sleep disorders are suspected. PSG records multiple physiological parameters during sleep, including brain activity, eye movements, muscle activity, heart rhythm, respiratory effort, oxygen saturation, and limb movements.
7.7 Differential Diagnosis
Several conditions may present with symptoms similar to insomnia and should be considered during evaluation. These include circadian rhythm sleep–wake disorders, obstructive sleep apnea, restless legs syndrome, periodic limb movement disorder, narcolepsy, medication-induced sleep disturbances, and sleep problems secondary to psychiatric or neurological disorders. Identifying these conditions is essential because management strategies differ considerably.
A systematic diagnostic approach enables clinicians to identify contributing factors, assess symptom severity, and develop individualized treatment plans that address both the sleep disturbance and any associated comorbid conditions.
|
Diagnostic Tool |
Purpose |
Clinical Utility |
|
Clinical history |
Assessment of sleep complaints and contributing factors |
First-line diagnostic evaluation |
|
Sleep diary |
Daily recording of sleep patterns |
Monitors sleep habits and treatment response |
|
Insomnia Severity Index (ISI) |
Measures severity of insomnia |
Evaluates symptom intensity and outcomes |
|
Pittsburgh Sleep Quality Index (PSQI) |
Assesses subjective sleep quality |
Identifies poor sleep quality |
|
Epworth Sleepiness Scale (ESS) |
Measures daytime sleepiness |
Screens for excessive daytime sleepiness |
|
Actigraphy |
Objective assessment of sleep–wake rhythm |
Useful for circadian rhythm disorders |
|
Polysomnography (PSG) |
Comprehensive overnight sleep study |
Reserved for suspected coexisting sleep disorders |
Table 5. Diagnostic Tools Used in the Evaluation of Insomnia
8. MANAGEMENT OF INSOMNIA
The primary goals of insomnia management are to improve sleep quality, reduce sleep latency, minimize nocturnal awakenings, restore daytime functioning, and enhance overall quality of life. Effective management requires an individualized approach that addresses the underlying causes, contributing factors, and patient-specific clinical characteristics. Current clinical guidelines recommend a combination of non-pharmacological and pharmacological interventions, with treatment selection based on symptom severity, duration of insomnia, comorbid conditions, patient preference, and potential treatment risks.
8.1 Treatment Goals
The principal objectives of insomnia treatment include:
8.2 Non-Pharmacological Management
Non-pharmacological interventions are considered the first-line treatment for chronic insomnia because they provide sustained clinical benefits without the adverse effects associated with long-term medication use. These approaches target the behavioral, cognitive, and environmental factors that contribute to persistent sleep disturbances.
8.2.1 Cognitive Behavioral Therapy for Insomnia (CBT-I)
Cognitive Behavioral Therapy for Insomnia (CBT-I) is the most effective evidence-based psychological treatment for chronic insomnia. It aims to modify maladaptive thoughts and behaviors that interfere with normal sleep while promoting healthy sleep habits.
The major components of CBT-I include:
Numerous clinical studies have demonstrated that CBT-I improves sleep latency, sleep efficiency, total sleep time, and daytime functioning, with benefits that are often maintained long after treatment has ended.
8.2.2 Sleep Hygiene Education
Sleep hygiene consists of behavioral and environmental practices that promote healthy sleep. Although sleep hygiene alone is usually insufficient for treating chronic insomnia, it forms an important component of comprehensive management.
Common sleep hygiene recommendations include:
8.2.3 Stimulus Control Therapy
Stimulus control therapy is designed to re-establish a strong association between the bed and sleep while reducing conditioned wakefulness.
Patients are advised to:
8.2.4 Sleep Restriction Therapy
Sleep restriction therapy aims to improve sleep efficiency by temporarily limiting the amount of time spent in bed to approximately match actual sleep duration. As sleep efficiency improves, time in bed is gradually increased under professional supervision. Although patients may initially experience increased daytime sleepiness, this approach has demonstrated significant long-term effectiveness in chronic insomnia.
8.2.5 Relaxation Therapy
Relaxation techniques reduce physiological and psychological arousal that interferes with sleep.
Common techniques include:
These interventions are particularly beneficial for individuals with stress-related insomnia or excessive pre-sleep anxiety.
|
Intervention |
Primary Objective |
Major Benefits |
|
Cognitive Behavioral Therapy for Insomnia (CBT-I) |
Modify maladaptive thoughts and behaviors |
First-line treatment with sustained long-term benefits |
|
Sleep Hygiene Education |
Promote healthy sleep habits |
Improves sleep environment and daily routine |
|
Stimulus Control Therapy |
Strengthen bed–sleep association |
Reduces conditioned wakefulness |
|
Sleep Restriction Therapy |
Improve sleep efficiency |
Consolidates sleep and reduces fragmented sleep |
|
Relaxation Therapy |
Reduce physiological and cognitive arousal |
Improves sleep initiation in stress-related insomnia |
|
Mindfulness-Based Interventions |
Improve emotional regulation |
Reduces anxiety and enhances sleep quality |
Table 6. Non-Pharmacological Interventions for Insomnia
CONCLUSION
Insomnia is a common and multifactorial sleep disorder that affects individuals across all age groups and has profound implications for physical health, mental well-being, cognitive performance, and overall quality of life. Contemporary evidence recognizes insomnia as an independent clinical disorder involving complex interactions among neurobiological, psychological, behavioral, and environmental factors, rather than merely a symptom secondary to other medical or psychiatric conditions. The disorder is frequently associated with significant daytime impairment and an increased risk of chronic diseases, emphasizing the importance of early recognition and timely intervention.
Advances in sleep medicine have considerably improved the understanding of the underlying mechanisms of insomnia, leading to more accurate diagnostic approaches and the development of targeted therapeutic strategies. Comprehensive clinical assessment remains the cornerstone of diagnosis, enabling clinicians to identify contributing factors and coexisting medical or psychiatric conditions that may influence treatment outcomes.
Current evidence supports Cognitive Behavioral Therapy for Insomnia (CBT-I) as the preferred first-line treatment for chronic insomnia because of its sustained efficacy and favorable safety profile. Pharmacological therapy continues to play an important role in selected patients, particularly for short-term symptom relief or when behavioral interventions alone are insufficient. Appropriate medication selection should be individualized, considering patient characteristics, comorbidities, treatment goals, and potential adverse effects. Recently introduced therapies, including dual orexin receptor antagonists and digital CBT-I, have further expanded the therapeutic options available for managing insomnia.
Despite significant progress, important challenges remain regarding early diagnosis, long-term management, treatment accessibility, and individualized care. Future research should focus on identifying reliable biomarkers, improving precision-based treatment approaches, and evaluating the long-term effectiveness and safety of emerging therapies. Strengthening public awareness, promoting healthy sleep practices, and integrating evidence-based interventions into routine clinical practice will be essential to reduce the global burden of insomnia and improve patient outcomes.
REFERENCES

Girendra Kumar Gautam, Km. Sweta*, Beyond Sleepless Nights: Integrating Neurobiology, Clinical Burden, And Emerging Therapeutic Advances In Insomnia: A Comprehensive Evidence-Based Review, Int. J. Sci. R. Tech., 2026, 3 (7), 519-533. https://doi.org/10.5281/zenodo.21412648
 10.5281/zenodo.21412648
10.5281/zenodo.21412648