Beyond The Numbers: Integrating Statistical Predictors With Lived Experiences Of Mothers Of Low Birth Weight Newborns Delivered In Tertiary Health Care Centre In Central India: A Mixed Method Study
1Department of Community Medicine, Government Medical College, Jalgaon 2Department of Pharmacology, Government Medical College, Akola. 3Department of Obstetrics and Gynaecology, Government Medical College, Alibag.
Background: Birth weight is single most important determinant of chances of survival, healthy growth and development of newborn. India accounts for 40% of LBW births in developing world. Thus, this study aimed to estimate the prevalence and to study lived experiencesperceptions of LBW among mothers. Objectives: To estimate prevalence and to study predictors of LBW among newborns delivered in tertiary health care centre in central India and to study lived experiences of mothers of LBW newborns. Methodology: A mixed method study was conducted during January 2025 to March 2026. Randomly 380 mothers were enrolled, structured proforma used for collection of data and association was analysed using Chi-square test. Qualitative data was gathered through 35 in-depth interviews and analysed via manual content analysis. Results: Mean age ± SD of mothers was 24.69 ±4.03 years, Majority 261 (68.69%) were from 20-30 years age group, 238 (62.63%) were homemakers, 191 (50.26%) Hindu, 118 (31.06%) from socioeconomic class III and 167 (43.95%) primigravida. Prevalence of LBW was 39.47%. Among 380 deliveries, 203 (53.42%) were male babies. Mean weight of baby 2.50 ± 0.61 kg. 274 (72.10%) were delivered at-term, 91 (23.95%) were preterm. Factors like working mothers (OR= 7.97), educated
Keywords
Prevalence, LBW, Newborn, ANC, Predictors.
Introduction
×
Low birth weight (LBW) defined as birth weight less than 2500 grams regardless of gestational age, remains a major public health challenge worldwide, particularly in developing countries1,10. LBW is closely associated with increased neonatal morbidity, mortality, impaired growth and cognitive development and long-term health complications2. According to global estimates, South Asia carries the highest burden of LBW, with India contributing significantly to the overall prevalence3.
Multiple maternal, socioeconomic, nutritional and healthcare-related factors contribute to LBW in India. Maternal anemia, inadequate antenatal care, poor maternal nutrition, low socioeconomic status, maternal age and pregnancy complications are commonly identified predictors4,5. Tertiary healthcare centres in Central India frequently manage high-risk pregnancies and referrals, making them important settings for studying determinants and outcomes related to LBW6.
Although several quantitative studies have examined statistical predictors of LBW, limited attention has been given to the lived experiences of mothers delivering LBW newborns7. Mothers often experience emotional distress, anxiety, financial burden, and challenges in caregiving, especially when newborns require prolonged hospitalization or intensive neonatal care8. Understanding these experiences is essential because maternal involvement plays a crucial role in newborn survival, breastfeeding, kangaroo mother care, and follow-up practices9.
Therefore, this study aimed to estimate the prevalence of Low Birth Weight and predictors of low birth weight and lived experiences of mothers of LBW babies.
AIM AND OBJECTIVES:
To estimate the prevalence of Low Birth Weight among newborn babies delivered in tertiary health care center in central India.
To study predictors of Low Birth Weight in study participants.
To study lived experiences of mothers of LBW babies.
MATERIALS AND METHODS:
Study design & setting:
A mixed method study was conducted among pregnant women delivered in tertiary health care center in central India.
Inclusion criteria: Pregnant women delivered in tertiary health care center and who gave consent to participate in study.
Exclusion criteria: Those who were critically ill or not willing to participate
Study period was extended from January 2025 to March 2026
SAMPLE SIZE & SAMPLING TECHNIQUE:
Considering p = prevalence of Low birth weight, from study conducted by Shobha R, Raje S et al. (2017) i.e. p = 41.9 % and at 95% Level of significance ( z = 1.96), Absolute error e= 5 % using the formula for Sample size, n = z²×pq /e²= 373.92, Thus, the sample size was taken as 380.
Randomly two days in a week were selected for data collection. Ten participants were selected randomly during each visit from delivery list of Obstetrics and Gynecology wards & those who were willing to participate were included in the study.
ETHICAL CONSIDERATION:
Permission was taken from Head of Department of Obstetrics and Gynecology of tertiary health care center. Informed consent from study participants was taken after establishing rapport and explaining the purpose of study. This study was approved by Institutional Ethics Committee.
METHODOLOGY:
Pregnant women from Obstetrics and Gynecology wards delivered in tertiary health care center were enrolled in the study. A face-to-face interview was taken and structured proforma was used for collection of data regarding sociodemographic characteristics, menstrual history, antenatal, postnatal and neonatal history. General & Systemic examination were done.Socioeconomic status was assessed by using Modified B.G. Prasad Scale (March 2025)4.
For the qualitative data, in‑depth interview of mothers of LBW newborns who were willing to talk freely was conducted till the point of saturation achieved.
STATISTICAL ANALYSIS:
Data was entered in MS Excel window version 11 and analysed by using Open-Epi Software. Descriptive statistics, quantitative variables were measured as Mean, Standard Deviation, while qualitative variables were presented in Numbers & Percentage. Bar chart & pai charts were used to summarise baseline characteristics of the study participants. Association between two categorical variables were analysed by using Chi-square (X2) test; p value < 0.05 was considered to be statistically significant, Odds Ratio was calculated. Manual content analysis was done.
Theme 1: The "Eat Last, Eat Least" Paradigm
Theme 2: The Double Burden of Labor
Theme 3: Barriers to Navigating Health Systems
Theme 4: Cultural Perceptions of "Small" Babies
Theme 5: Psychological Stress and Household Agency
RESULTS:
Table 1: Distribution of study participants according to Sociodemographic characteristics (n=380)
Variables
Number
Percentage
1. Age
(in years)
<20
59
15.53
20- 25
129
33.95
25- 30
132
34.74
≥30
60
15.78
2. Residence
Urban
197
51.84
Rural
183
48.16
3. Religion
Hindu
191
50.26
Muslim
102
26.84
Bauddha
73
19.21
Others
14
03.69
4. Type of family
Nuclear
173
45.53
Joint
167
43.94
Three Generation
40
10.53
5. Type of Diet
Vegetarian
214
56.32
Mixed
166
43.68
6. Education
Illiterate
65
17.11
Primary school
56
14.74
Middle school
66
17.37
High school
80
21.05
Intermediate
79
20.79
Diploma
16
04.21
Graduate
11
02.89
Postgraduate
7
01.84
7. Occupation
Homemakers
238
62.63
Unskilled
34
08.95
Semi-skilled
24
06.32
Skilled
84
22.10
8. Socioeconomic Status
(Modified BG Prasad scale, March 2025)
Class I
20
05.26
Class II
112
29.47
Class III
118
31.06
Class IV
79
20.79
Class V
51
13.42
Total 380 study participants were enrolled in the study. Majority were in the age group of 20-30 years 261(68.69%) followed by ≥30 years 60(15.78%). The Mean age was 24.69 years with SD ±4.03 Minimum age was 18 years & maximum was 32 years (Range 14). Majority 197(51.84%) were from urban area, 173(45.53%) from nuclear family.
One hundred ninety-one (50.26%) were from Hindu religion. Regarding education, 65(17.10%) were illiterate, 80(21.05%) were educated upto high school. Majority 238(62.63%) were homemakers, rest were working mothers. As per the Modified BG Prasad scale (March 20252023), mostly belongs to Class III 118(31.06%) followed by class II, 112(29.47%).
Table 2: Obstetrics profile of study participants (n= 380)
1.Parity
Primiparity
304
80.00
Parity 2
53
13.95
Parity 3
17
04.47
Grand multipara
6
01.58
2. Period of Gestation at delivery
(in weeks)
<37 weeks
91
23.95
37- 42 weeks
274
72.10
≥42 weeks
15
03.95
3.Mode of delivery
Normal delivery
209
55.00
Caesarean section
171
45.00
4. Anaemia in pregnancy
Present
179
47.11
Absent
201
52.89
5. Grade of anaemia
(n= 179)
Mild
110
61.45
Moderate
33
18.44
Severe
30
16.76
Profound
6
03.35
6. Number of ANC visits
<4 visits
147
38.68
≥4 visits
233
61.32
7. Number of IFA tablets consumed during pregnancy
Consumed < 100
149
39.21
Consumed ≥ 100
231
60.79
8. Birth spacing in consecutive pregnancies (n= 213)
<18 months
59
27.70
18-24 months
91
42.72
≥ 24 months
63
29.58
9. Pre-pregnancy weight
<55 kg
207
54.47
≥55 kg
173
45.53
12. Weight gain during pregnancy
<9 kg
177
46.58
≥9 kg
203
53.42
13. Anaemia during pregnancy
Mild
235
61.84
Moderate
69
18.16
Severe
65
17.10
Profound
11
02.90
Most of the mothers were primigravida primipara 304(80.00%). Most were term deliveries 274(72.10%), 91(23.95%) were delivered <37 weeks. Most of the deliveries 209(55.00%) were normal vaginal deliveries while 171(45.00%) were caesarean deliveries. One hundred seventy- nine (47.11%) mothers were anaemic, among them 110(61.45%), 33(18.44%), 30(16.76%) & 6(03.35%) were having mild, moderate, severe & profound anaemia respectively. Most of mothers 233(61.32%) done ≥4 ANC visits & 231(60.79%) taken≥ 100 tablets during pregnancy. Majority of mothers 91(42.72%) had 18-24 months of birth spacing in consecutive pregnancies, 207(54.47%) had pre-pregnancy weight less than 55kg & only 177(46.58%) of mothers had gain less than 9kg weight during pregnancy.
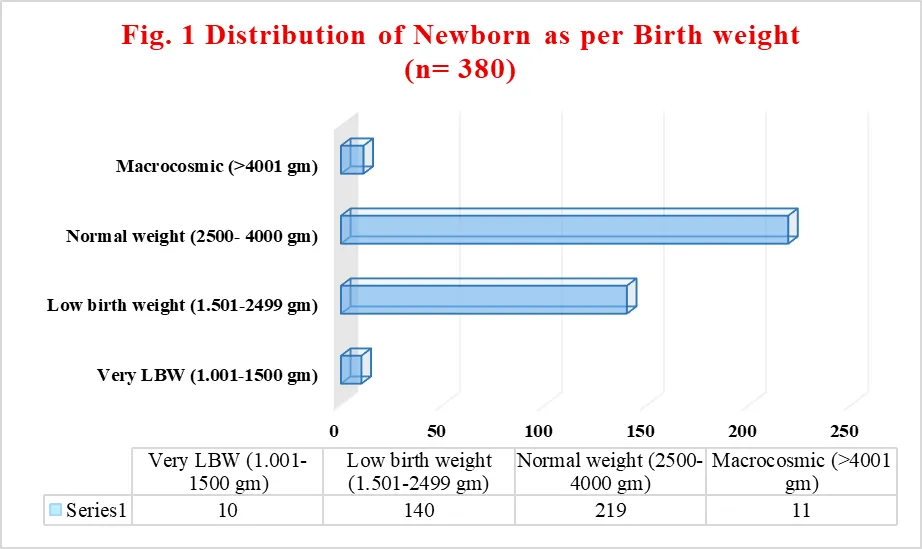
Table 3: Distribution of Newborn as per pregnancy outcome (n=380)
1. Sex of baby
Male
203
53.42
Female
177
46.58
2. Weight of baby
Very LBW (1.001-1500 gm)
10
02.63
Low birth weight (1.501-2499 gm)
140
36.84
Normal weight (2500- 4000 gm)
219
57.63
Macrocosmic (>4001 gm)
11
02.90
3. Gestational age at delivery
Preterm (<37 weeks)
91
23.95
Term (37- 42 weeks)
274
72.10
Post term (≥42 weeks)
15
03.95
Fig. 1 & Table 3 shows, among 380 deliveries, 203(53.42%) were male babies. Prevalence of LBW was found to be 39.47%. Mean weight of baby was 2.50 kg with SD ± 0.61 maximum weight was 4.30 kg & minimum weight was 0.850 kg (Range= 3.45). Most of them 274(72.10%) were delivered at term, only 91(23.95%) were preterm babies.
Table 4 Association between Sociodemographic characteristics & LBW (n= 380)
Variable
Total
LBW
OR
95% CI
p- value
Present
Absent
1. Age of mother (in years)
<20 years & ≥30 year
119
76
43
4.47
2.817, 7.081
0.0000
20- 29 years
261
74
187
2. Place of Residence
Rural
183
81
102
1.47
0.9745, 2.227
0.0826
Urban
197
69
128
3. Religion
Hindu
191
69
122
0.75
0.4992,1.139
0.2164
Others
189
81
108
4. Type of family
Nuclear
173
82
91
1.84
1.215, 2.793
0.0053
Others
207
68
139
5. Education of mother
<high school
187
96
91
2.72
1.775, 4.155
0.0000
≥ high school
193
54
139
6. Occupation of mother
Working mother
142
98
44
7.97
4.979, 12.75
0.0000
Others
238
52
186
7. Socioeconomic status
III, IV, V
248
108
140
1.65
1.06, 2.577
0.0342
I, II
132
42
90
Table 4 shows, Association between sociodemographic characteristics & LBW. Mother of <20years & ≥30 years were found 4.47 times more prone for delivering of LBW babies as compare to those of 20-29 years & the association is statistically significant (OR= 4.47, 95% CI= 2.817- 7.081, p =0.00). Other factors such as mother from nuclear family (OR= 1.84), educated less than high school (OR= 2.72), working mothers (OR= 7.97) & those from lower socioeconomic (III, IV, V) class (OR= 1.65) were at risk of delivering LBW babies & this association is also statistically significant (p- value <0.05).
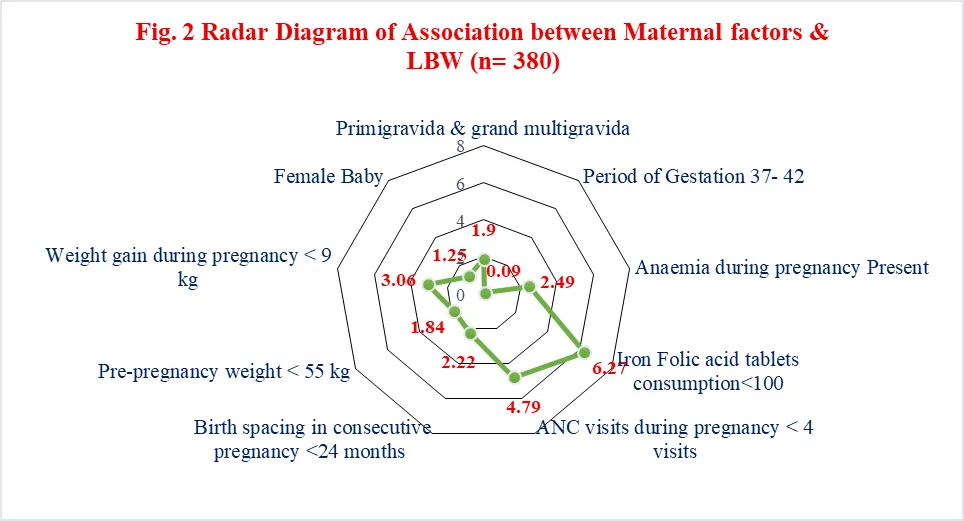
Table 5 Association between Maternal factors & LBW (n= 380)
Variables
Total
LBW
OR
95% CI
p- value
Present
Absent
1. Gravidity
Primigravida & grand multigravida
194
91
103
1.90
1.252, 2.889
0.0034
Others
186
59
127
2. Period of Gestation
37- 42
274
67
207
0.09
0.0523, 0.153
0.0000
Other
106
83
23
3. Anaemia during pregnancy
Present
179
91
88
2.49
1.632, 3.795
0.0000
Absent
201
59
142
4. Iron Folic acid tablets consumption
<100
149
97
52
6.27
3.973, 9.88
0.0000
≥100
231
53
178
5. ANC visits during pregnancy
< 4 visits
147
91
56
4.79
3.071, 7.478
0.0000
≥4 visits
233
59
174
6. Birth spacing in consecutive pregnancy (n= 213)
<24 months
150
79
71
2.22
1.204, 4.112
0.0100
≥24 months
63
21
42
7. Pre-pregnancy weight
< 55 kg
173
82
91
1.84
1.215, 2.793
0.0053
≥ 55 kg
207
68
139
8. Weight gain during pregnancy
< 9 kg
147
82
65
3.06
1.989, 4.71
0.0000
≥ 9 kg
233
68
165
9. Sex of baby
Female
177
75
102
1.25
0.8308, 1.895
0.3298
Male
203
75
128
Fig. 2 & Table 5 shows, Association between Maternal factors, sex of baby & LBW. Mother of primigravida and grand multigravida were 1.9 time more at risk of LBW deliveries as compare to others (OR= 1.90) and the association was statistically significant (p<0.05). Anaemic mothers (OR= 2.49), those who consume <100 IFA tablets during pregnancy (OR= 6.27), those having <4 ANC visits (OR= 4.79) were at risk of delivering a LBW baby (p <0.05). Mother having less birth spacing (OR= 2.22), those having less pre- pregnancy weight (OR= 1.84) and weight gain less than 9 kg during pregnancy (OR= 3.06) were more prone for development of LBW baby as compare to others (p <0.05). Sex of the baby and LBW delivery did not show any statistically significant association (p value= 0.3298)
In-depth interviews of 35 mothers of LBW newborn were taken for qualitative analysis.
Themes
Sub-Themes/ Categories
Illustrative Quote (No. of Respondents)
Theme 1:
The "Eat Last, Eat Least" Paradigm
1. Intrafamilial food distribution
2. Pregnancy food taboos (avoiding "hot" foods)
3. Lack of dietary diversity.
"I only eat what is left after my husband and father-in-law finish. Often, the vegetables are gone, and I just eat roti with salt/ pickle." (16)
"My elders told me not to eat papaya or meat during the second trimester, fearing it would cause a miscarriage, even though the doctor said I needed the protein." (11)
"We cannot afford milk every day; that is reserved for the growing children in the house, not for me." (10)
Theme 2:
The Double Burden of Labor
1. Agricultural workload
2. Domestic drudgery (fetching water/firewood)
3. Lack of "mandatory" rest periods.
"The fields do not wait for my pregnancy. If I don't bend to transplant the rice, we lose our income for the season." (15)
"I carry 20-liter pots of water from the community well/ Tap two times a day. My back aches, but who else will do it?" (07)
Theme 3:
Barriers to Navigating Health Systems
1. Distance decay" (transport issues)
2. Lack of trust in institutional care
3. The cost of "free" healthcare (loss of wages)
The ASHA Tai tells me to go to the Rural hospital, but the bus frequency has reduced. A private auto asks for more than my husband's daily wage just for one trip." (13)
"I went to the clinic, but the machine was broken, and they told me to go to the city. I am a labourer; I cannot afford to lose three days of work just for one sonography” (19)
"The nurse was angry because I missed my last check-up, but I had no one to look after my other three children while I waited in the queue” (08)
Theme 4:
Cultural Perceptions of "Small" Babies
1. Fear of obstructed labour (C-sections)
2. Normalized low birth weight
3. Fatalistic beliefs
"Neighbours tell me that if I eat too much 'Iron' (tablets), the baby's bones will become too hard and I will need an operation (C-section). I want a normal delivery, so I skip the tablets." (11)
"My mother said it is better to have a small baby; it comes out easily. If the baby is too big, they will have to cut my stomach open." (07)
"Everyone in our village has small babies. We are small people, so we expect the child to be small too. It is God’s will." (02)
Theme 5:
Psychological Stress and Household Agency
1. Preference for male children
2. Domestic disharmony
3. Lack of decision-making power
"This is my third girl. The tension in the house makes my stomach tight. I feel no hunger when there is constant shouting." (13)
"I wanted to go for the scan, but my mother-in-law said it was a waste of money and that her generation never needed such things." (21)
DISCUSSION
Total 380 study participants were enrolled in the study. Majority were in the age group of 20-30 years 261(68.69%). Fifty-nine (15.53%) were < 20 years. The Mean age was 24.69 years. Majority 197(51.84%) were from urban area, 173(45.53%) from nuclear family followed by 167(43.94%) from Joint family. One hundred ninety-one (50.26%) were from Hindu religion. Similar findings were seen in the study conducted by Shastri A (2023)14, Keshavrao CM (2023)13, Girish Chavhan (2026)30, Sulakhe R et al21.
Regarding education, 65(17.10%) were illiterate, Majority 238(62.63%) were homemakers, rest were working mothers. As per the Modified BG Prasad scale (March 2025), mostly belongs to Class III 118(31.06%) followed by 112(29.47%), 79(20.79%), 51(13.42%) belong to Class II, Class IV, Class V respectively, Similar findings were seen in the study conducted by Shastri A (2023)14, Keshavrao CM (2023)13, Girish Chavhan (2026)30, Choudhary M et al23, Sulakhe R et al21.
Most of the mothers were Primipara 133(35.00%). Twenty-seven (07.11%) & 6(01.58%) were grand multigravida & grand multipara respectively. Most were term deliveries 274(72.10%). Ninety-one (23.95%) were delivered <37 weeks & 15(03.95%) were delivered at ≥42 weeks of pregnancy. 179(47.11%) mothers were anaemic among them 110(65%), 33(18.44%), 30(16.76%) & 6(03.35%) were having mild, moderate, severe & profound anaemia respectively. Most of mothers 233(61.32%) done ≥4 ANC visits, 231(60.79%) taken≥ 100 tablets during pregnancy. Majority of mothers 91(42.72%) had 18-24 months of birth spacing in consecutive pregnancies, 207(54.47%) had pre-pregnancy weight less than 55kg & only 177(46.58%) mothers had gained weight less than 9 kg during pregnancy, Similar findings were seen in the study conducted by Ghanghas K et al16, Keshavrao CM (2023)13, Rajashree Bhosale33, Girish Chavhan (2026)22, Bhagyashree et al (2026)32.
Among 380 deliveries, 203(53.42%) were male babies & 177(46.58%) were female. Prevalence of LBW was found to be 39.47%. Most of them were delivered at term (37- 42 weeks) 274 (72.10%), only 91(23.95%) were preterm babies similar findings were seen in studies conducted by Thapa P et al17.
Mother of <20years & ≥ 30 years were found 4.47 times more prone for development of LBW babies as compare to those of 20-29 years & the association is statistically significant Other factors such as mother from nuclear family (OR= 1.84), Educated less than high school (OR= 2.72), working mothers (OR= 7.97) & those from lower socioeconomic (III, IV, V) class (OR= 1.65) were at risk of delivering LBW babies & this association is statistically significant (p- value <0.05), Similar findings were seen in the study conducted by Ghanghas K et al16, Rajashree Bhosale33, Ghanghas K et al17, Keshavrao CM (2023)14.
Mother of primigravida and grand multigravida were 1.9 time more at risk of LBW deliveries as compare to others. Anaemic mothers, those who consume <100 IFA tablets, those having <4 ANC visits were at risk of delivering a LBW baby (p <0.05). Mother having less birth spacing, those having less pre- pregnancy weight, gained less than 9 kg weight during pregnancy were more prone for development of LBW baby as compare to others. Sex of the baby and LBW delivery didn’t showed any statistically significant association (p value= 0.3298) similar findings were seen in studies conducted by Patel S19, Choudhary M et al24, Roy A et al26, Sulekhe R et al22.
CONCLUSION
In our study, we found prevalence of LBW among newborns delivered at tertiary health care centre in central India was 39.47%. Pregnancy at early age (<20 years) or delayed pregnancy ≥30 years) were found to be a risk factors for LBW. Others factors such as low education, women working during pregnancy, mothers of lower socioeconomic class, grand multigravida, anaemic and those who had not taking IFA tablets during pregnancy, having less than 4 ANC visits, less birth spacing between consecutive pregnancies, low weight/ BMI in pre-pregnant state were significantly associated with LBW deliveries.
RECOMMENDATIONS:
Provide direct financial incentives to offset lost daily wages, ensuring labour-intensive workers can prioritize mandatory rest and ANC visits.
Shift focus from individual mothers to educating husbands and elders to dismantle "eat last" traditions and debunk myths related to causes difficult deliveries
REFERENCES
World Health Organization. Global nutrition targets 2025: low birth weight policy brief. Geneva: WHO; 2014.
Barua A, Hazarika J, Dutta S. Correlates of low birth weight: a hospital-based study from Gangtok, India. Int J Health Sci Res. 2014;4(12):224-30.
United Nations Children’s Fund, World Health Organization. Low birthweight estimates: levels and trends 2000–2015. Geneva: WHO; 2019.
Singh D, Manna S, Barik M, Rehman T, Kanungo S, Pati S. Prevalence and correlates of low birth weight in India: findings from National Family Health Survey 5. BMC Pregnancy Childbirth. 2023;23:456.
Girotra S, Mohan N, Malik M, Roy S, Basu S. Prevalence and determinants of low birth weight in India: findings from a nationally representative cross-sectional survey (2019–21). Cureus. 2023;15(3):e36717.
Kundu RN, Ghosh A, Chhetri B, Saha I, Hossain MG, Bharati P. Regional with urban-rural variation in low birth weight and its determinants of Indian children: findings from NFHS-5 data. BMC Pregnancy Childbirth. 2023;23:616.
Banerjee A, Sen S, Khan J, Pal M, Bharati P. Decadal change in the association between young mother’s BMI and anaemia with child low birth weight in India. BMC Pregnancy Childbirth. 2022;22:147.
Singh S, Rajak R. Barriers in utilization and provisioning of obstetric care services in India: a mixed-methods systematic review. BMC Pregnancy Childbirth. 2024;24:16.
Mazumder S, Upadhyay RP, Hill Z, Taneja S, Dube B, Kaur J, et al. Kangaroo mother care: using formative research to design an acceptable community intervention. BMC Public Health. 2018;18:307
Dr Amrita Shastri et al. A Glimpse into Geriatric Health: Multimorbidity and Drug Adherence Among Rural Elderly in Central India - A Cross Sectional Study. International Journal of Innovative Research in Technology (IJIRT). 2025;12(4):3906-3914
World Health Organization and United Nations Children's Fund (UNICEF): Low birthweight: country, regional and global estimates. (2004). Accessed: March 11, 2023: https://apps.who.int/iris/handle/10665/43184
Gothi A, Meena A, Dodiyar R et al. Incidence and major risk factors for term low birth weight babies in a southern district of Rajasthan. European Journal of Molecular & Clinical Medicine. 2023;10(2):1921-27
Devaguru A, Gada S, Potpalle D, et al. (May 05, 2023) The Prevalence of Low Birth Weight Among Newborn Babies and Its Associated Maternal Risk Factors: A Hospital-Based Cross-Sectional Study. Cureus 15(5): e38587. DOI 10.7759/cureus.38587
Keshavrao CM, Thakre SS, Thakre S, Jadhao AR, Agrawal S, Shastri A. Prevalence of High-Risk Pregnancies among Women of more than Twenty-weeks of Gestation attending Antenatal Clinic in Tertiary Heath Care Center in Central India: A Cross-Sectional Study. Indian Journal of Basic & Applied Medical Research. 2023 Dec 1;13(1)
Shastri A, Jadhao AR, Agrawal S. Health Status of Elderly, with Special Reference to Nutritional Status: A Cross Sectional Study. Indian Journal of Basic & Applied Medical Research. 2023 Dec 1;13(1)
Islam M, Khan M, Khan A et al. Newborn Care Practices and Associated Factors Influencing Their Health in a Northern Rural India. MDPI Journal. 2023;10(408):1-13.
Ghanghas K, Chauhan M, Kansagara T et al. Analysis of Maternal and Obstetric Factors Affecting Birth Weight of Newborn: A Hospital-Based Cross Sectional Study. International Journal of Scientific Research in Dental and Medical Sciences. 2022;4(2):52-56
Thapa P, Poudyal A, Poudel R et al. Prevalence of low birth weight and its associated factors: Hospital based cross sectional study in Nepal. PLOS Global Public Health. 2022;2(11):1-11
Herawati S, Tridiyawati F. Risk Factor Analysis Of Low Birth Weight Events (LBW) At Kartika Husada Hospital. International Journal of Health and Pharmaceutical. 2021;646-51. https://ijhp.net
Patel S, Verma N, Padhi et al. Retrospective analysis to identify the association of various determinants on birth weight. Journal of Family Medicine & Primary Care.2021;10(1):496-1
Chaithra A, Chiniwar M, Menasinkai S et al. A study on maternal factors affecting low birth weight in institutional deliveries International Journal of Reproduction, Contraception, Obstetrics and Gynecology. 2020;9(10):4245-9
Sulakhe R, Lavanya K, Nageswara R et al. A cross sectional study on demographic factors affecting low birth weight. International Journal of Community Medicine and Public Health. 2019;6(11):4896-900
Tigistu Toru, WalellignAnmut et al. Assessment of Low Birth Weight and Associated Factors Among Neonates in Butajira General Hospital, South Ethiopia, Cross Sectional Study, 2019. International Journal of Pediatrics Volume 2020, Article ID 5841963, 6 pages https://doi.org/10.1155/2020/5841963
Choudhary M, Verma R, Jain S et al. Study of knowledge attitude practices and utilisation of existing health services by families with regard to newborn health at block level in rural India: a community based, cross sectional, observational study International Journal of Contemporary Paediatrics. 2019;6(2):704-12
Chaurasia A, Gautam R et al. A hospital based study on Low birth weight, complication of childbirth and associated risk factor at Sagar district hospital, Madhya Pradesh, India. Anthropological and Behavioral Sciences. 2019; DOI: 10.13140/RG.2.2.25753.44646 https://www.researchgate.net/publication/344781958.
Roy A, Akter MZ, Biswas DC: Trends in prevalence of low-birth-weight babies in India. Int J Contemp Pediatr. 2021, 8:1725-9.
Sumana M, Sreelatha CY, Girija BS, Sundar M, Gowda D: Low birth weight and its determinants in a teaching hospital of Karnataka, India. Int J Community Med Public Health. 2016, 3:610-4. 10.18203/2394- 6040.ijcmph20160484
Talie A, Taddele M, Alemayehu M: Magnitude of low birth weight and associated factors among newborns delivered in Dangla primary hospital, Amhara regional state, Northwest Ethiopia, 2017. J Pregnancy. 2019, 2019:3587239
Appiah PK, Bukari M, Yiri-Erong SN, et al.: Antenatal care attendance and factors influenced birth weight of babies born between June 2017 and May 2018 in the Wa East District, Ghana. Int J Reprod Med. 2020, 2020:1653076. 10.1155/2020/1653076
Girish Chavhan, Mahesh Chavhan*, Amrita Shastri, Bhagyashree Chavan, Prevalence, Determinants, Medication Use Patterns and Lived Experiences of Hypertension Among the Geriatric Population of Eastern Maharashtra: A Mixed-Method Study, Int. J. Sci. R. Tech., 2026, 3 (4), 174-182. https://doi.org/10.5281/zenodo.19413852
Bhagyashree K. Chavan et al. Insights into Maternal Care with Emphasis on High-Risk Pregnancy: A Cross Sectional Study at the Antenatal Clinic of a Tertiary Healthcare Centre in Eastern Maharashtra. IJSDR. 2025; 10 (12): b122-b130 | https://www.ijsdr.org/viewpaperforall.php?paper=IJSDR25121182025; 10 (12): b122-b130 | https://www.ijsdr.org/viewpaperforall.php?paper=IJSDR2512118
Rajashree Bhosale, Bhagyashree Chavan*, Prevalence And Predictors Of Low Birth Weight Among Newborn Delivered In Tertiary Health Care Centre Of South-Western Maharashtra (Civil Hospital, GMC Alibag): A Cross-Sectional Study, Int. J. Sci. R. Tech., 2026, 3 (4), 1238-1248. https://doi.org/10.5281/zenodo.19925559
Reference
World Health Organization. Global nutrition targets 2025: low birth weight policy brief. Geneva: WHO; 2014.
Barua A, Hazarika J, Dutta S. Correlates of low birth weight: a hospital-based study from Gangtok, India. Int J Health Sci Res. 2014;4(12):224-30.
United Nations Children’s Fund, World Health Organization. Low birthweight estimates: levels and trends 2000–2015. Geneva: WHO; 2019.
Singh D, Manna S, Barik M, Rehman T, Kanungo S, Pati S. Prevalence and correlates of low birth weight in India: findings from National Family Health Survey 5. BMC Pregnancy Childbirth. 2023;23:456.
Girotra S, Mohan N, Malik M, Roy S, Basu S. Prevalence and determinants of low birth weight in India: findings from a nationally representative cross-sectional survey (2019–21). Cureus. 2023;15(3):e36717.
Kundu RN, Ghosh A, Chhetri B, Saha I, Hossain MG, Bharati P. Regional with urban-rural variation in low birth weight and its determinants of Indian children: findings from NFHS-5 data. BMC Pregnancy Childbirth. 2023;23:616.
Banerjee A, Sen S, Khan J, Pal M, Bharati P. Decadal change in the association between young mother’s BMI and anaemia with child low birth weight in India. BMC Pregnancy Childbirth. 2022;22:147.
Singh S, Rajak R. Barriers in utilization and provisioning of obstetric care services in India: a mixed-methods systematic review. BMC Pregnancy Childbirth. 2024;24:16.
Mazumder S, Upadhyay RP, Hill Z, Taneja S, Dube B, Kaur J, et al. Kangaroo mother care: using formative research to design an acceptable community intervention. BMC Public Health. 2018;18:307
Dr Amrita Shastri et al. A Glimpse into Geriatric Health: Multimorbidity and Drug Adherence Among Rural Elderly in Central India - A Cross Sectional Study. International Journal of Innovative Research in Technology (IJIRT). 2025;12(4):3906-3914
World Health Organization and United Nations Children's Fund (UNICEF): Low birthweight: country, regional and global estimates. (2004). Accessed: March 11, 2023: https://apps.who.int/iris/handle/10665/43184
Gothi A, Meena A, Dodiyar R et al. Incidence and major risk factors for term low birth weight babies in a southern district of Rajasthan. European Journal of Molecular & Clinical Medicine. 2023;10(2):1921-27
Devaguru A, Gada S, Potpalle D, et al. (May 05, 2023) The Prevalence of Low Birth Weight Among Newborn Babies and Its Associated Maternal Risk Factors: A Hospital-Based Cross-Sectional Study. Cureus 15(5): e38587. DOI 10.7759/cureus.38587
Keshavrao CM, Thakre SS, Thakre S, Jadhao AR, Agrawal S, Shastri A. Prevalence of High-Risk Pregnancies among Women of more than Twenty-weeks of Gestation attending Antenatal Clinic in Tertiary Heath Care Center in Central India: A Cross-Sectional Study. Indian Journal of Basic & Applied Medical Research. 2023 Dec 1;13(1)
Shastri A, Jadhao AR, Agrawal S. Health Status of Elderly, with Special Reference to Nutritional Status: A Cross Sectional Study. Indian Journal of Basic & Applied Medical Research. 2023 Dec 1;13(1)
Islam M, Khan M, Khan A et al. Newborn Care Practices and Associated Factors Influencing Their Health in a Northern Rural India. MDPI Journal. 2023;10(408):1-13.
Ghanghas K, Chauhan M, Kansagara T et al. Analysis of Maternal and Obstetric Factors Affecting Birth Weight of Newborn: A Hospital-Based Cross Sectional Study. International Journal of Scientific Research in Dental and Medical Sciences. 2022;4(2):52-56
Thapa P, Poudyal A, Poudel R et al. Prevalence of low birth weight and its associated factors: Hospital based cross sectional study in Nepal. PLOS Global Public Health. 2022;2(11):1-11
Herawati S, Tridiyawati F. Risk Factor Analysis Of Low Birth Weight Events (LBW) At Kartika Husada Hospital. International Journal of Health and Pharmaceutical. 2021;646-51. https://ijhp.net
Patel S, Verma N, Padhi et al. Retrospective analysis to identify the association of various determinants on birth weight. Journal of Family Medicine & Primary Care.2021;10(1):496-1
Chaithra A, Chiniwar M, Menasinkai S et al. A study on maternal factors affecting low birth weight in institutional deliveries International Journal of Reproduction, Contraception, Obstetrics and Gynecology. 2020;9(10):4245-9
Sulakhe R, Lavanya K, Nageswara R et al. A cross sectional study on demographic factors affecting low birth weight. International Journal of Community Medicine and Public Health. 2019;6(11):4896-900
Tigistu Toru, WalellignAnmut et al. Assessment of Low Birth Weight and Associated Factors Among Neonates in Butajira General Hospital, South Ethiopia, Cross Sectional Study, 2019. International Journal of Pediatrics Volume 2020, Article ID 5841963, 6 pages https://doi.org/10.1155/2020/5841963
Choudhary M, Verma R, Jain S et al. Study of knowledge attitude practices and utilisation of existing health services by families with regard to newborn health at block level in rural India: a community based, cross sectional, observational study International Journal of Contemporary Paediatrics. 2019;6(2):704-12
Chaurasia A, Gautam R et al. A hospital based study on Low birth weight, complication of childbirth and associated risk factor at Sagar district hospital, Madhya Pradesh, India. Anthropological and Behavioral Sciences. 2019; DOI: 10.13140/RG.2.2.25753.44646 https://www.researchgate.net/publication/344781958.
Roy A, Akter MZ, Biswas DC: Trends in prevalence of low-birth-weight babies in India. Int J Contemp Pediatr. 2021, 8:1725-9.
Sumana M, Sreelatha CY, Girija BS, Sundar M, Gowda D: Low birth weight and its determinants in a teaching hospital of Karnataka, India. Int J Community Med Public Health. 2016, 3:610-4. 10.18203/2394- 6040.ijcmph20160484
Talie A, Taddele M, Alemayehu M: Magnitude of low birth weight and associated factors among newborns delivered in Dangla primary hospital, Amhara regional state, Northwest Ethiopia, 2017. J Pregnancy. 2019, 2019:3587239
Appiah PK, Bukari M, Yiri-Erong SN, et al.: Antenatal care attendance and factors influenced birth weight of babies born between June 2017 and May 2018 in the Wa East District, Ghana. Int J Reprod Med. 2020, 2020:1653076. 10.1155/2020/1653076
Girish Chavhan, Mahesh Chavhan*, Amrita Shastri, Bhagyashree Chavan, Prevalence, Determinants, Medication Use Patterns and Lived Experiences of Hypertension Among the Geriatric Population of Eastern Maharashtra: A Mixed-Method Study, Int. J. Sci. R. Tech., 2026, 3 (4), 174-182. https://doi.org/10.5281/zenodo.19413852
Bhagyashree K. Chavan et al. Insights into Maternal Care with Emphasis on High-Risk Pregnancy: A Cross Sectional Study at the Antenatal Clinic of a Tertiary Healthcare Centre in Eastern Maharashtra. IJSDR. 2025; 10 (12): b122-b130 | https://www.ijsdr.org/viewpaperforall.php?paper=IJSDR25121182025; 10 (12): b122-b130 | https://www.ijsdr.org/viewpaperforall.php?paper=IJSDR2512118
Rajashree Bhosale, Bhagyashree Chavan*, Prevalence And Predictors Of Low Birth Weight Among Newborn Delivered In Tertiary Health Care Centre Of South-Western Maharashtra (Civil Hospital, GMC Alibag): A Cross-Sectional Study, Int. J. Sci. R. Tech., 2026, 3 (4), 1238-1248. https://doi.org/10.5281/zenodo.19925559
Amrita Shastri
Corresponding author
Department of Community Medicine, Government Medical College, Jalgaon
Mahesh Chavhan
Co-author
Department of Community Medicine, Government Medical College, Jalgaon
Girish Chavhan
Co-author
Department of Pharmacology, Government Medical College, Akola.
Bhagyashree Chavan
Co-author
Department of Obstetrics and Gynaecology, Government Medical College, Alibag.
Mahesh Chavhan1, Amrita Shastri*1, Girish Chavhan2, Bhagyashree Chavan3, Beyond The Numbers: Integrating Statistical Predictors With Lived Experiences Of Mothers Of Low Birth Weight Newborns Delivered In Tertiary Health Care Centre In Central India: A Mixed Method Study, Int. J. Sci. R. Tech., 2026, 3 (6), 349-361. https://doi.org/10.5281/zenodo.20555669




 10.5281/zenodo.20555669
10.5281/zenodo.20555669