
We use cookies to ensure our website works properly and to personalise your experience. Cookies policy
SCPM College of Nursing and Paramedical Science, Gonda, Uttar Pradesh
Background: Lower back pain (LBP) is one of the most prevalent musculoskeletal conditions globally, significantly affecting individuals' quality of life and contributing to healthcare burdens. It is a multifactorial condition caused by structural, occupational, and lifestyle factors, with disc degeneration, spondylolisthesis, and fractures being common causes. Despite advancements in diagnostic imaging, the correlation between radiographic findings and clinical symptoms remains inconsistent, posing challenges in diagnosis and management. Objectives: The objectives of the study are to determine the prevalence of structural abnormalities associated with LBP, analyze the distribution of LBP across age groups and genders, and assess the correlation between radiographic findings and clinical symptoms. Methodology: A descriptive cross-sectional design was adopted for this study, conducted at SCPM Hospital, Gonda, India. A total of 100 patients aged 17 years and above, presenting with LBP, were recruited using non-probability convenience sampling. Data collection involved a structured questionnaire capturing demographic and clinical information and radiographic analysis of lumbosacral spine X-rays. The inclusion criteria included patients willing to provide informed consent and meeting the diagnostic criteria for radiographic imaging, while those with prior similar study participation or unwillingness to participate were excluded. The data were analyzed using descriptive statistics to summarize the findings and inferential statistics, including chi-square tests and logistic regression, to identify significant associations. Results : The results revealed that 50% of participants reported chronic pain, with moderate severity being most common (50%). Radiographic findings indicated that disc degeneration was the most prevalent abnormality (50%), followed by spondylolisthesis (20%) and osteophytes (10%). The correlation between age and radiographic abnormalities was significant, with older participants (above 45 years) exhibiting higher rates of degenerative changes. Occupational factors also played a critical role, as sedentary workers reported the highest prevalence of moderate pain, while manual laborers experienced severe pain. Gender-specific differences were observed, with males showing higher rates of disc degeneration and females exhibiting more fractures, likely due to osteoporosis.
Overview of Lower Back Pain (LBP):
Lower back pain (LBP) is one of the most prevalent musculoskeletal conditions worldwide, significantly impacting individuals' quality of life and imposing a substantial burden on healthcare systems. According to the National Institute of Neurological Disorders and Stroke (NINDS), LBP is defined as pain or discomfort localized below the costal margin and above the inferior gluteal folds, often accompanied by restricted mobility or functional limitation. It can be classified into three categories based on duration: acute pain (lasting a few days to weeks), subacute pain (lasting between 4 and 12 weeks), and chronic pain (lasting over 12 weeks)
Definition and Classification of Lower Back Pain:
The term "lower back pain" broadly encompasses pain originating from the lumbar spine or its associated structures. According to Casiano et al. (2023), "LBP is a heterogeneous condition characterized by a spectrum of pain intensities and functional impairments that vary across individuals and etiological factors." [3] Acute LBP is often self-limiting and typically results from mechanical injuries or muscle strain, whereas chronic LBP may stem from degenerative changes, structural abnormalities, or systemic conditions such as osteoporosis and rheumatoid arthritis. [8] Classification systems also consider pain patterns, such as nociceptive pain (caused by tissue damage), neuropathic pain (resulting from nerve irritation or compression), and mixed pain types (combining elements of both). These classifications assist clinicians in identifying appropriate diagnostic and therapeutic approaches tailored to the underlying cause.
Causes and Risk Factors of Lower Back Pain (LBP):
Lower back pain (LBP) is a multifactorial condition with a wide range of underlying causes and risk factors. It can arise from mechanical, traumatic, pathological, and lifestyle-related factors, often presenting diagnostic challenges due to overlapping etiologies. According to Vincent et al. (2023), “LBP is a complex interplay of structural, environmental, and behavioral factors, requiring a holistic approach to diagnosis and treatment. [10]” Understanding these causes and risk factors is critical for developing targeted interventions.
Role of Radiographic Imaging in LBP :
Diagnosis Radiographic imaging plays a crucial role in diagnosing lower back pain (LBP), aiding in identifying structural abnormalities and ruling out serious underlying conditions. It provides clinicians with valuable insights into the anatomy and pathology of the lumbar spine. According to AlAteeq et al. (2020), “Imaging is an indispensable tool in the evaluation of LBP, particularly when clinical findings alone are insufficient for accurate diagnosis.” [1] This section discusses the various imaging modalities, their benefits and limitations, and the correlation between radiographic findings and clinical symptoms.
Types of Imaging Modalities: X-rays, CT, MRI The three primary imaging modalities used in the assessment of LBP are X- rays, computed tomography (CT), and magnetic resonance imaging (MRI), each offering unique diagnostic capabilities.
Advantages and Limitations of Radiographs in LBP Diagnosis:
Radiographs are widely used in LBP diagnosis due to their simplicity, rapid availability, and ability to detect common spinal pathologies such as fractures, osteophytes, and abnormal curvatures. They are particularly effective in ruling out severe conditions such as vertebral fractures and metastatic lesions. However, radiographs have significant limitations. They offer poor sensitivity in detecting soft tissue abnormalities such as disc herniation, ligament injuries, or nerve compression. Furthermore, there is often a weak correlation between radiographic findings and clinical symptoms in non-specific LBP. As highlighted by Shetty et al. (2017), “A normal X-ray does not preclude significant pathology, while abnormal findings may not always correlate with pain severity.” [8] Another limitation is radiation exposure, particularly in younger patients or those requiring frequent imaging. Advances such as digital radiography and automatic exposure control systems have mitigated some of these concerns by optimizing radiation doses
Correlation Between Radiographic Findings and Clinical Symptoms:
The relationship between radiographic findings and clinical symptoms in LBP is complex and often inconsistent. While imaging can reveal structural abnormalities, their presence does not always correspond to the severity or type of pain experienced by the patient. For example, disc degeneration and osteophytes are frequently observed on X-rays, yet they are also common in asymptomatic individuals, particularly in older populations [4]. Conversely, significant symptoms such as radiculopathy or neurological deficits may arise in patients with minimal radiographic abnormalities. As Zalatimo (2023) emphasizes, “The challenge lies in distinguishing incidental findings from clinically significant pathology, underscoring the need for a holistic approach that integrates imaging with patient history and physical examination .[11]” Radiographic imaging is most effective when used in conjunction with clinical findings, guiding further diagnostic or therapeutic interventions. For instance, a plain X-ray may identify spondylolisthesis in a patient with chronic LBP, prompting advanced imaging like MRI to evaluate nerve involvement.
METHODOLOGY
The methodology section outlines the systematic approach adopted to investigate the causes of lower back pain (LBP) using radiographic imaging. This ensures the study is scientifically sound, replicable, and aligned with ethical research principles.
Methodology Flow Chart:
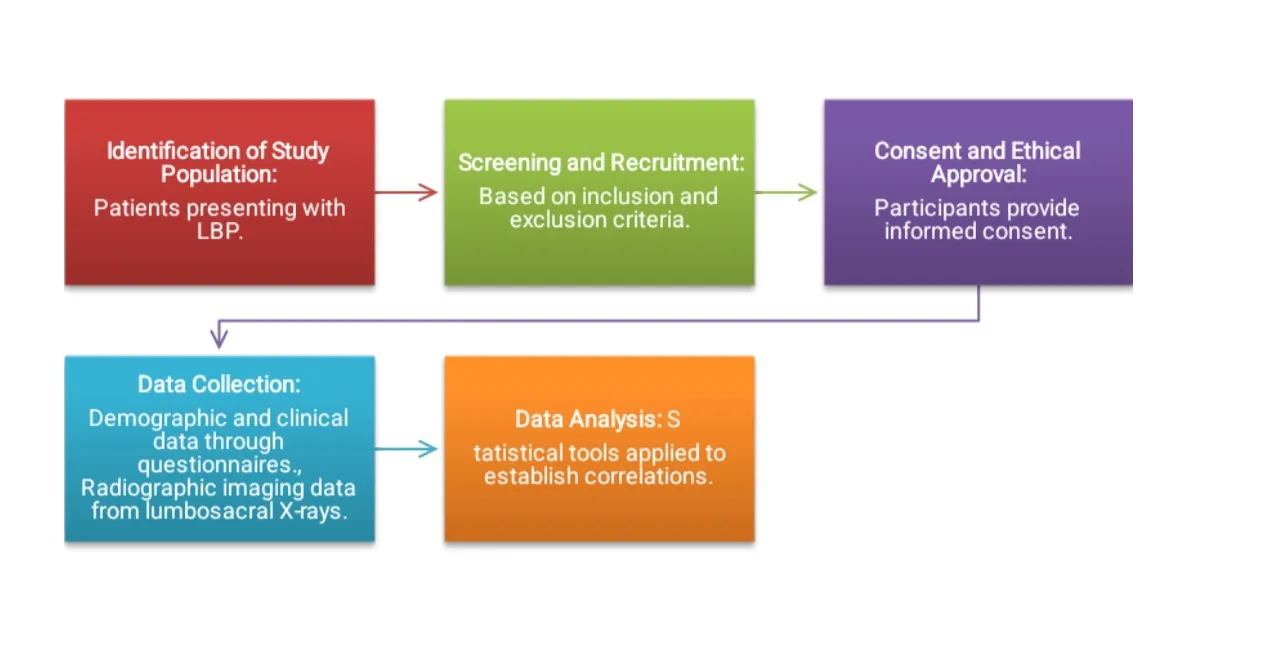
Research Design:
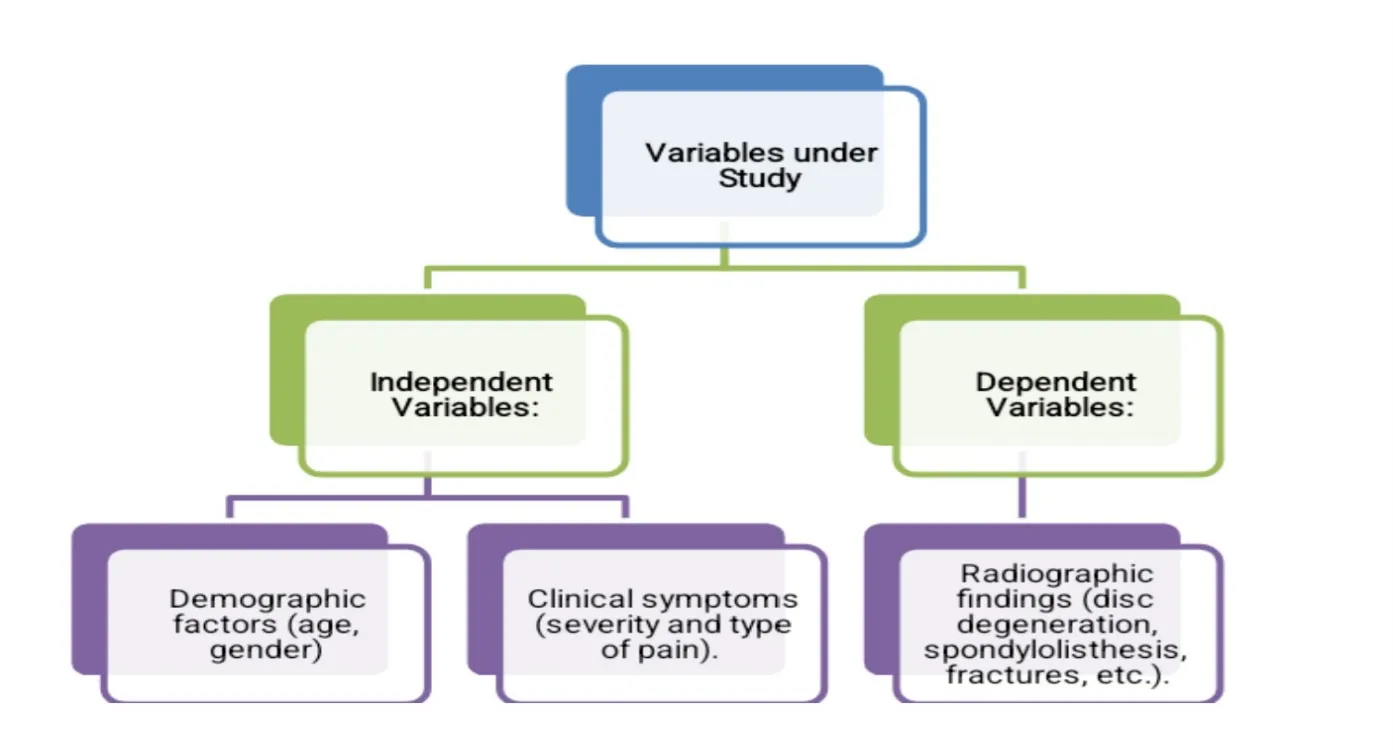
A descriptive cross-sectional design was chosen to analyze data at a single point in time. This design is ideal for identifying the prevalence of radiographic abnormalities in patients with LBP and exploring associations with demographic and clinical variables. Variables under Study
1. Independent Variables: Demographic factors (age, gender), clinical symptoms (severity and type of pain)
2. Dependent Variables: Radiographic findings (disc degeneration, spondylolisthesis, fractures, etc.).
MAJOR FINDINGS AND RESULT
This section presents the major findings of the study and provides a comprehensive discussion of their implications. The analysis integrates quantitative results, existing literature, and clinical relevance to highlight critical insights into the causes of lower back pain (LBP) based on radiographic findings, patient demographics, and clinical symptoms. The study revealed critical insights into the prevalence, causes, and correlates of LBP, focusing on radiographic findings, demographic patterns, and clinical symptoms. Key findings include:
1. Demographics: The majority of participants were between 31 and 45 years old (40%), with males constituting 60% of the sample. Occupation played a significant role, with sedentary workers (45%) and manual laborers (35%) being the most affected, highlighting the dual risk of inactivity and physical strain.
2. Pain Characteristics: Chronic pain was the most common type, reported by 50% of participants, with moderate severity being predominant (50%). Acute and subacute pain affected 20% and 30% of participants, respectively, indicating that most cases persisted over time, reflecting inadequate early intervention.
3. Radiographic Abnormalities: Disc degeneration was the most prevalent abnormality (50%), followed by spondylolisthesis (20%) and osteophytes (10%). Only 15% of participants had normal radiographs,emphasizing the structural nature of LBP. Age-related changes were apparent, with degenerative findings increasing significantly in older age groups.
4. Occupational Influence: Sedentary workers reported the highest prevalence of moderate pain, while manual laborers experienced more severe pain, underscoring the role of ergonomic challenges and physical strain in LBP.
5. Gender Differences: Disc degeneration was more common in males (30%), while fractures were exclusively observed in females, likely due to osteoporosis and bone health issues.
These findings align with existing literature and underscore the multifactorial nature of LBP, necessitating tailored, multidisciplinary approaches for effective diagnosis and management.
CONCLUSION
The study concludes that LBP is a multifactorial condition requiring a comprehensive and multidisciplinary approach to diagnosis and management. Radiographic imaging is instrumental in identifying structural causes of LBP, but clinical evaluations must complement imaging to ensure accurate diagnosis and avoid unnecessary interventions. Early intervention strategies, such as ergonomic adjustments, physical therapy, and public health initiatives promoting bone health and physical activity, are essential for reducing the burden of LBP. The findings underscore the need for tailored interventions addressing age, gender, and occupation-specific risks.
This research contributes to the growing body of evidence on LBP, emphasizing the importance of integrating clinical, radiographic, and demographic data for effective management. Further studies with larger and more diverse populations, incorporating advanced imaging modalities, are recommended to provide a more holistic understanding of LBP and its underlying causes.
REFERENCES


Abhishek Kumar Maurya*, Jyoti Yadav, Sandhya Verma, Shubhanshi Rani, Shivam Kumar, Detection Of Lower Back Pain Causes By Clinical Impairment Of Lumbar Spine Through Lumbar Spine Radiograph, Int. J. Sci. R. Tech., 2026, 3 (6), 1175-1179. https://doi.org/10.5281/zenodo.20773602
 10.5281/zenodo.20773602
10.5281/zenodo.20773602