
We use cookies to ensure our website works properly and to personalise your experience. Cookies policy
1Department of Pharmaceutics, C.L. Baid Metha College of Pharmacy, Chennai, India.
2Department of Pharmacology, C.L. Baid Metha College of Pharmacy, Chennai, India.
3Department of Microbiology, Madras Christian College, Chennai, India.
Background: Sodium-glucose cotransporter-2 inhibitors (SGLT2i) have cardiovascular benefits in type 2 diabetes mellitus (T2DM), but the mechanisms are not fully understood. This study aimed to identify potential cardiovascular targets using network pharmacology and molecular docking. Methods: Targets of nine SGLT2 inhibitors were collected from SwissTargetPrediction and DrugBank. T2DM, heart failure (HF) and coronary artery disease (CAD) targets were obtained from GeneCards and DisGeNET. PPI network, GO/KEGG enrichment and molecular docking analysis of common targets. Results: A total of 116 were identified as common targets. Candidate targets were EGFR, MAPK1, PIK3CA, and PIK3CD, after excluding hepatic metabolic enzymes (CYP, UGT families) KEGG analysis indicated enrichment in the AGE-RAGE signaling and lipid/atherosclerosis pathways. Molecular docking yielded weak binding energies (-2.58 to -5.88 kcal/mol), below the typical high confidence threshold (? -7.0 kcal/mol). The strongest interaction was ipragliflozin-MAPK1 (-5.88 kcal/mol). Conclusions: SGLT2 inhibitors may potentially interact with EGFR, MAPK1, PIK3CA, and PIK3CD in T2DM-associated HF and CAD. Nevertheless, the poor docking findings indicate that these hypotheses require experimental confirmation. This research provides a hypothesis-generating framework, not conclusive evidence.
The Diabetes mellitus (DM) is a metabolic illness marked by elevated blood sugar levels brought on by partial or total insulin insufficiency as well as/or insulin resistance [1]. Because of changes in dietary patterns, lifestyles of the populace, and economic progress, DM has been diagnosed in around 537 million individuals globally. Up to 11.3% in 2030 and 12.2% in 2045, the incidence rate is predicted to increase [2]. DM causes a variety of long-term issues that significantly impact the health and well-being of those who have it, in addition to elevated blood glucose levels. DM can cause cardiovascular disorders (CVD), which is one of the most concerning aspects of the condition. People with diabetes are disproportionately affected by cardiovascular disorders, which include heart failure, stroke, and coronary artery disease. Research has repeatedly demonstrated that those with diabetes have a two to four times higher risk of developing CVD than those without the disease [3]. Among the cardiovascular risks of DM, Heart failure (HF) and Coronary artery disease (CAD) are the frequently overlooked complications [4, 5].
According to the latest studies, persons with DM have a 2- to 5-fold higher risk of HF and 2- to 4-fold higher risk of CAD than people without DM [6, 7]. Despite receiving therapy for this comorbid illness, the individuals continue to be at risk for CVD. So it is necessary to replace the therapy with some other medications. Sodium-glucose cotransporter 2 (or) sodium glucose-linked transporter inhibitors (SGLT2Is) are oral anti-diabetic drugs (OADs) that improve glycemic control in people with type 2 diabetes (T2DM). About 90% of the reabsorption of filtered glucose is carried out by the renal proximal convoluted tubule, and their mechanism of action includes the blockage of SGLT2 channels there [8]. Due to its hypoglycemic properties as well as its effect on protecting the heart and kidneys, SGLT2I has emerged as a potentially beneficial family of drugs. The United States Food and Drug Administration (USFDA) has approved several SGLT2Is, including Bexagliflozin (BEXA), Canagliflozin (CANA), Empagliflozin (EMPA), Dapagliflozin (DAPA), and Ertugliflozin (ERTU), and the Japan Pharmaceuticals and Medical Devices Agency (PMDA) has approved medications like Ipragliflozin (IPRA), Tofogliflozin (TOFO), Luseogliflozin (LUSEO), and Sotagliflozin (SOTA) for the treatment of DM [9-13] . Large-scale clinical studies have shown the cardiovascular advantages of SGLT2Is. There is the possibility that these profits have something to do with better glycemic management, which is precisely the processes behind these profits are being extensively studied. Treatment with one of the SGLT2Is, EMPA, decreased the risk of CV death and hospitalization for HF in diabetic patients. Hospitalizations for HF were assessed as a secondary outcome, with the composite of cardiovascular mortality, nonfatal MI, and nonfatal stroke serving as the primary outcome. Of the 7020 type-2 diabetes patients who were randomized to receive either empagliflozin or a placebo, 490 of 4687 patients (10.5%) experienced the primary endpoint, while approximately 2300 patients (12%) in the placebo group experienced 282 events hazard ratio (HR): 0.86, 95% confidence interval (CI): 0.74-0.99, p = 0.04). At a median of 3.1 years, there was a 35% reduction in HF hospitalisation (HR 0.65, 95% CI: 0.50-0.85).Both those at risk for HF and those with a confirmed diagnosis of HF experienced this impact, according to the first major SGLT2 inhibitor trial Empagliflozin Cardiovascular Outcome Event Trial in Type 2 Diabetes Mellitus Patients–Removing Excess Glucose (EMPA-REG OUTCOME) study[14]. In the CANVAS (Canagliflozin Cardiovascular Assesment Study and Canagliflozin Cardivascular Assesment Study- Renal) trial, 10142 individuals with type 2 diabetes and a high cardiovascular risk were randomized to receive canagliflozin versus a placebo. The main result was a composite endpoint consisting of nonfatal myocardial infarction, nonfatal stroke, or death from cardiovascular causes[15] . The biggest study population of type 2 diabetes mellitus with atherosclerotic cardiovascular disease or at risk for it (n = 17,160) was included in the DECLARE TIMI-58 (Dapagliflozin Effect on Cardiovascular Events-Thrombolysis in Myocardial Infarction 58) experiment. Compared to placebo, the key composite effectiveness objective of cardiovascular mortality or hospitalization for heart failure (HR 0.83; 95% CI: 0.73–0.95) was significantly lower in the study with dapagliflozin. This reduction was primarily due to a substantial decrease in HF hospitalizations (HR 0.73, 95% CI: 0.61–0.88)[16]. In DAPA-HF (Dapagliflozin and Prevention of Adverse Outcomes in Heart Failure) study, dapagliflozin vs placebo was randomly given to 4,744 patients with HF New York Heart Association (NYHA) class II-IV with an ejection fraction of around 40%, regardless of diabetes, in addition to the best available medical treatment for HF. When compared to placebo, dapagliflozin decreased the individual endpoints of worsening heart failure event (HR:0.70; 95% CI: 0.59- 0.83, NNT= 27) and cardiovascular mortality (HR: 0.82; 95% CI: 0.69-0.98) as well as the primary endpoint of Worsening heart failure or cardiovascular mortality (HR: 0.74; 95% CI: 0.65-0.85). This impact was shown over the course of the 18.2 month trial period and was unaffected by the existence of diabetes[17]. These four major trials suggest that SGLT2Is are a significant new treatment strategy for at-risk individuals with or without DM in treating HF and CAD. Although these studies have recommended medications (SGLT2Is) for the treatment of CVD, their primary targets and methods of action remain unclear, and understanding them is very important. Network pharmacology is a field of study grounded on multidirectional pharmacology and systems biology. It is used to perform target analysis and drug molecular design using particular nodes and biomolecular network analysis techniques. Network pharmacology is based on a complete methodology that is more effective for examining the target and route interactions between medications and disorders than standard experimental pharmacology methods[18]. Thus, in this work, we employed network pharmacology analysis to systemically identify putative SGLT2I targets on the CV protection of T2DM. this will offer a strong foundation for more comprehensive research into the mechanism of action of SGLT2Is on T2DM with CAD and HF.
MATERIALS AND METHODS:
SGLT2 Inhibitor-Related Targets:
The Canonical SMILES of SGLT2Is namely BEXA, DAPA, EMPA, CANA, ERTU, IPRA, TOFO, LUSEO, and SOTA were gathered using Pubchem (https://pubchem.ncbi.nlm.nih.gov/), which is a favoured chemical knowledge source with many different uses. PubChem has had several updates during the last two years. Over 120 data sources have contributed data to PubChem. PubChem comprises a diverse range of chemical entities, including lipids, polysaccharides, siRNA, miRNA, and chemically modified biopolymers, however small molecules make up the majority of its contents [19]. Then the SMILES datas were entered into the SwissTargetPrediction database (http://www.swisstargetprediction.ch/), by which Nine SGLT2 inhibitors' possible targets were determined by entering their Canonical SMILES into a target prediction algorithm. The Swiss target prediction technique estimates almost all of a small molecule's macromolecular targets while providing details on chemical constituents and biological activities [20]. In addition to SwissTargetPrediction database, we used another database known as DrugBank (https://go.drugbank.com/) to gather SGLT2Is related Genes. DrugBank is a distinct bioinformatics and chemical informatics database that includes information on 11,628 pharmaceuticals together with chemical properties, pharmacological targets, protein data, and other relevant information [21]. According to the data collected from these 2 databases, Duplicate genes present in each drug data were removed by using Excel and the resultant data of all the drugs were used.
Drug-Disease-Targets Prediction:
The terms T2DM, HF, CAD were retrieved from GeneCards (https://www.genecards.org/) and Disgenet (https://www.disgenet.org/) in order to identify potential target genes. Over 7000 human genes are included in the GeneCards database, and moreover, every single gene has a recognized gene symbol[22] and DisGeNET is a comprehensive platform for discovery created to answer a range of queries related to the genetic basis of human disorders. DisGeNET is one of the largest collections of its sort currently accessible, with over 380,000 correlations between over 16,000 genes and 13,000 disorders[23]. According to the data collected from these 2 databases, Duplicate genes present in each disease data were removed by using Excel, and the resultant data of all the diseases were used. According to the Targets of SGLT2Is and the disorders, we obtained a Venn diagram on Bioinformatics & Evolutionary Genomics (https://bioinformatics.psb.ugent.be/webtools/Venn/) and the intersected Genes were obtained known as HubGenes.
Construction of the Network Model:
Two network models, which include 1) a network model between nine SGLT2 inhibitors and their corresponding targets, and 2) a network model between the points where medications and diseases intersect, were constructed using a software tool called Cytoscape v3.10.1. Cytoscape can effectively represent the interactions between proteins, DNA, and genes in order to show network linkages[24].
Core-Target screening for SGLT2 inhibitors in the management of diabetes mellitus with HF and CAD:
Analysis of protein-protein interactions inside the PPI network can identify core regulatory genes. One useful resource for finding PPI information is the STRING database (https://stringdb.org/), which has a plethora of data regarding known and predicted protein-protein interactions of different species[25]. HubGenes were loaded into the STRING database, "Multiproteins" was chosen, and "Homo Sapiens" was chosen as the organism. The results were filtered with an interaction score of >0.9, disconnected nodes in the network were removed, and the remaining parameters were left unchanged. The TSV file was exported into the Cytoscape 3.10.1 application for additional analysis. The degrees of targets were determined using the Cytohubba plugin, which is based on Cytoscape, in order to identify the core targets in the common targets between drugs and diseases.
Protein-Protein Interaction (PPI) Network Construction of Core-Targets:
The STRING internet platform was used to build the PPI network of critical targets. The Gene Name list of target proteins was uploaded to the network once the multiple proteins module was chosen, confining the species to Homo sapiens and setting the confidence score to > 0.9. The PPI diagram has solid circles for each gene, with the protein structure shown in the center of each circle and lines of various colors connecting the circles. Each line depicts a biological event that occurs between two proteins, such as signal transmission, gene expression regulation, cell migration, and so forth [24].
Functional Enrichment Analysis:
Genes are categorized by gene ontology (GO) into three groups: molecular function (MF), cellular component (CC), and biological process (BP). The signaling pathways implicated in genes were examined using the Kyoto Encyclopedia of Genes and Genomes (KEGG) [26]. For the GO and KEGG pathway studies in this work, the Database for Annotation, Visualization, and Integrated Discovery (David) (https://david.ncifcrf.gov/summary.jsp) was utilized. The SRplot was used to visualize the Bar and Bubble chart of GO and KEGG Functional enrichment analysis.
Molecular docking analysis:
SGLT2 inhibitors were molecularly docked to the top two targets in the PPI network and the first 3 key targets in the "pathway-Target" network. The Protein Data Bank (PDB, https://www.rcsb.org/) provided the 3D structure of the main targets (Homo sapiens mode and X-Ray diffraction value less than 3) in PDB format. Additionally, the Pubchem Database (https://pubchem.ncbi.nlm.nih.gov/) provided the 3D structure of the drugs. According to the discussion by Rizvi et al in 2013, the Autodock tool 1.5.7 platform was used to carry out the molecular docking study [27, 28].
RESULTS:
Exploring SGLT2 Inhibitors' Potential Related Targets
The Canonical SMILES of SGLT2Is namely BEXA, DAPA, EMPA, CANA, ERTU, IPRA, TOFO, LUSEO, and SOTA were gathered using PubChem online platform (Table 1). By importing their Canonical SMILES into SwissTargetPrediction database, we obtained 100 Targets for Bexagliflozin, 100 Targets for Dapagliflozin, 100 Targets for Empagliflozin, 100 Targets for Canagliflozin, 100 Targets for Ertugliflozin, 100 Targets for Ipragliflozin, 100 Targets for Tofogliflozin, 100 Targets for Luseogliflozin, and 100 targets for Sotagliflozin. 7 Bexagliflozin Targets, 11 Dapagliflozin Targets, 10 Empagliflozin Targets, 8 Canagliflozin Targets, 0 Ertugliflozin Target, 0 Ipragliflozin Target, 0 Tofogliflozin Target, 0 Luseogliflozin Target, and 0 Sotagliflozin Target were obtained using DrugBank database. After deduplicating each drug targets retrieved from the two databases and combining, a total of 932 SGLT2Is targets were found (Table 2). Then entering them into Cytoscape v3.10.1 to construct a network model between nine SGLT2 inhibitors and their corresponding targets. There are 277 nodes (268 predicted targets and 9 drugs) and 932 edges. Where the SGLT2 inhibitors are shown as Blue-colored V nodes, drug targets (predicted targets) are represented by Orange nodes, and interactions between the medications and targets are represented by the edges (Figure 1). This illustrates a potential way that SGLT2 inhibitors and various targets interact.
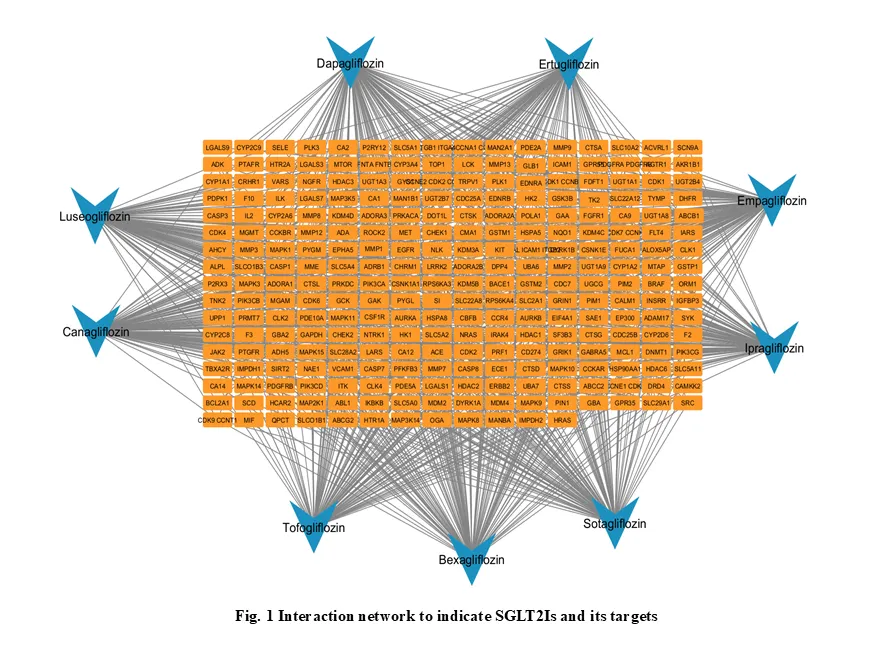
Figure 1 Interaction network to indicate SGLT2Is and its targets
|
SGLT2i |
Pubchem (cid) |
Molecular Formula |
CANONICAL SMILES |
|
Bexagliflozin |
25195624 |
C24H29ClO7
|
C1CC1OCCOC2=CC=C(C=C2)CC3=C(C=CC(=C3)C4C(C(C(C(O4)CO)O)O)O)Cl |
|
Canagliflozin |
24812758 |
C24H25FO5S
|
CC1=C(C=C(C=C1)C2C(C(C(C(O2)CO)O)O)O)CC3=CC=C(S3)C4=CC=C(C=C4)F |
|
Empagliflozin |
11949646 |
C23H27ClO7
|
C1COCC1OC2=CC=C(C=C2)CC3=C(C=CC(=C3)C4C(C(C(C(O4)CO)O)O)O)Cl |
|
Dapagliflozin |
9887712 |
C21H25ClO6
|
CCOC1=CC=C(C=C1)CC2=C(C=CC(=C2)C3C(C(C(C(O3)CO)O)O)O)Cl |
|
Ertugliflozin |
44814423 |
C22H25ClO7
|
CCOC1=CC=C(C=C1)CC2=C(C=CC(=C2)C34C(C(C(C(O3)(CO4)CO)O)O)O)Cl |
|
Ipragliflozin |
10453870 |
C21H21FO5S
|
C1=CC=C2C(=C1)C=C(S2)CC3=C(C=CC(=C3)C4C(C(C(C(O4)CO)O)O)O)F |
|
Tofogliflozin |
46908929 |
C22H26O6
|
CCC1=CC=C(C=C1)CC2=CC3=C(COC34C(C(C(C(O4)CO)O)O)O)C=C2 |
|
Luseogliflozin |
11988953 |
C23H30O6S
|
CCOC1=CC=C(C=C1)CC2=CC(=C(C=C2C)OC)C3C(C(C(C(S3)CO)O)O)O |
|
Sotagliflozin |
24831714
|
C21H25ClO5S
|
CCOC1=CC=C(C=C1)CC2=C(C=CC(=C2)C3C(C(C(C(O3)SC)O)O)O)Cl
|
Table 1 – Information on nine SGLT2 inhibitors from pubchem
|
Drugs |
Swiss target prediction (stp) |
Drug bank (db) |
Targets before de-duplicating |
Duplicates |
Removed |
Targets after de-duplication |
|
Bexagliflozin
|
100 |
7 |
107 |
1 |
1 |
106 |
|
Canagliflozin
|
100 |
8 |
108 |
1 |
1 |
107 |
|
Empagliflozin
|
100 |
10 |
110 |
1 |
1 |
109 |
|
Dapagliflozin
|
100 |
11 |
111 |
1 |
1 |
110 |
|
Ertugliflozin
|
100 |
0 |
100 |
0 |
0 |
100 |
|
Ipragliflozin
|
100 |
0 |
100 |
0 |
0 |
100 |
|
Tofogliflozin
|
100 |
0 |
100 |
0 |
0 |
100 |
|
Luseogliflozin
|
100 |
0 |
100 |
0 |
0 |
100 |
|
Sotagliflozin
|
100 |
0 |
100 |
0 |
0 |
100 |
Table 2 Total drug targets
Exploring the network model between the intersectional targets of illnesses and medications
Following de-duplication and merging, searches via the Genecards and DisGeNet databases yieldedan aggregate of 36,924 T2DM-related targets, 17,575 CAD-related targets, and 20,498 HF-related targets.The 116 SGLT2Is that intersected with the diseases were found using a Venn diagram (Figure 2a). To create a network model connecting the intersection targets of illnesses and medications, the 116 targets were put into Cytoscape v3.10.1. orange-colored V nodes represent diseases, there were 120 nodes (116 nodes represent targets, 1 node represent SGLT2 inhibitors, and 3 nodes represent Diseases) and 464 edges shown in the network. A single green-colored V node represents nine SGLT2 inhibitors, and the three orange and numerous blue-colored nodes represent putative targets (Figure 3).
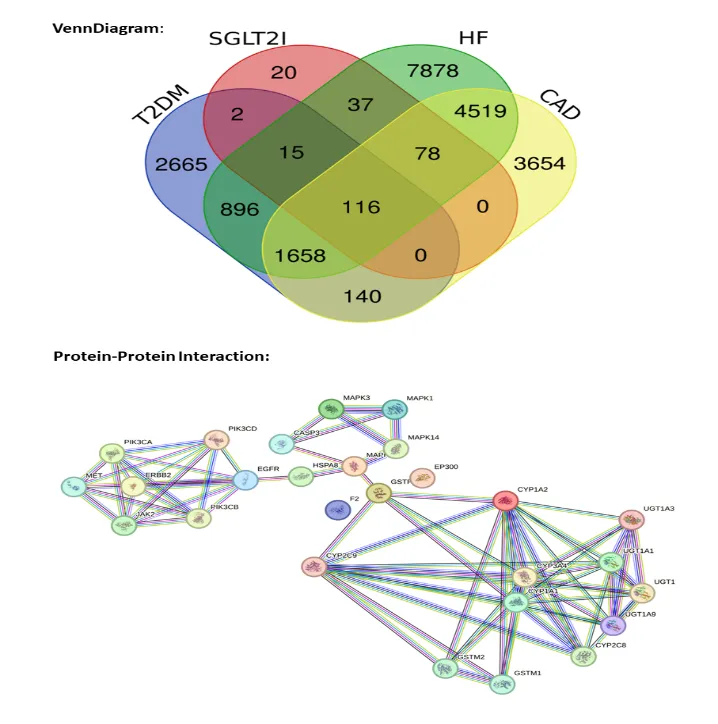
Figure 2a Venn Diagram and 2b Protein-protein Interaction
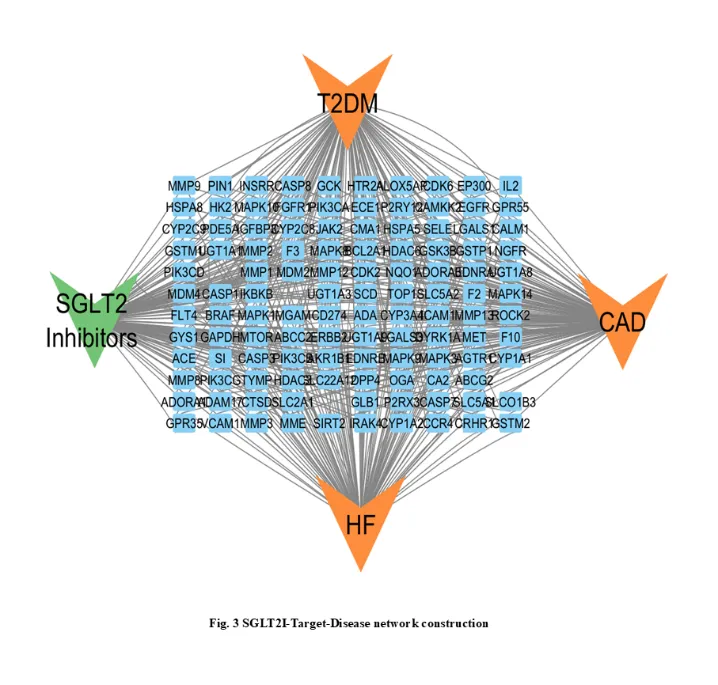
Figure 3 SGLT2I-Target-Disease network construction
Core-Targets of SGLT2 Inhibitors in the Treatment OF DM with HF and CAD:
The STRING online platform received 116 common targets in total, and an export file in the "TSV" format was produced. After that, it was imported into Cytoscape v3.10.1, where the "Cytohubba" plugin was used to determine the core targets by calculating the degree of each target. Red, orange, and yellow nodes in the screen of 27 key targets of SGLT2Is for the management of T2DM with HF and CAD indicate the degree value is progressively lowered from huge to small reduction in the degree value from large to small (Table 3).
|
SR. NO |
GENE NAME |
RANK |
SCORE |
|
1 |
EGFR |
1 |
12 |
|
2 |
CYP1A2 |
1 |
12 |
|
3 |
CYP3A4 |
3 |
11 |
|
4 |
PIK3CA |
3 |
11 |
|
5 |
CYP1A1 |
3 |
11 |
|
6 |
PIK3CD |
6 |
10 |
|
7 |
PIK3CB |
6 |
10 |
|
8 |
CYP2C9 |
6 |
10 |
|
9 |
UGT1A8 |
9 |
8 |
|
10 |
UGT1A1 |
9 |
8 |
|
11 |
UGT1A9 |
11 |
7 |
|
12 |
UGT1A3 |
12 |
6 |
|
13 |
CASP3 |
12 |
6 |
|
14 |
MAPK8 |
12 |
6 |
|
15 |
JAK2 |
12 |
6 |
|
16 |
CYP2C8 |
12 |
6 |
|
17 |
F2 |
17 |
5 |
|
18 |
GSTP1 |
17 |
5 |
|
19 |
MAPK1 |
17 |
5 |
|
20 |
MAPK3 |
17 |
5 |
|
21 |
ERBB2 |
17 |
5 |
|
22 |
HSPA |
17 |
5 |
|
23 |
MET |
17 |
5 |
|
24 |
EP300 |
17 |
5 |
|
25 |
GSTM2 |
17 |
5 |
|
26 |
GSTM1 |
17 |
5 |
|
27 |
MAPK14 |
17 |
5 |
Table 3 - Specific information for top-ranked targets (including metabolic enzymes later excluded)
Since these CYP and UGT genes are mostly involved in drug metabolism, they were later removed from the cardioprotective target study.
Analysis of Protein-Protein Interaction (PPI) of 27 key Targets
The 27 primary targets of SGLT2Is-HF-T2DM-CAD were loaded and a network of target protein interactions was created using the STRING database platform. The final protein-protein interaction network was produced by choosing the species "Homo sapiens" and establishing a combined score > 0.9 criterion. As seen in (Figure 2b), there are a total of 27 solid circles in various colors, each of which represents a significant target gene. The target gene's protein structure is displayed in the middle of each circle. Degree scores indicate that the top 5 Hub targets are EGFR, CYP1A2, CYP3A4, PIK3CA, and CYP1A1. Nevertheless, as CYP1A2, CYP3A4, and CYP1A1 are mostly hepatic drug-metabolizing enzymes, they were not taken into account as direct cardioprotective targets. The remaining targets such as EGFR and PIK3CA may be crucial for SGLT2 inhibitors when treating diabetes mellitus with HF and CAD.
Analysis of GO and KEGG enrichment analysis for Targets
A total of 138 items—including 84 terms related to biological processes (BP), 11 terms related to cell composition (CC), and 43 terms related to molecular functions (MF)—were recovered from 27 core targets in the GO enrichment analysis with a P value <0.05 and an FDR <0.05. Following screening, a bar graph shows the top 10 CC, BP, and MF terms based on Fold enrichment (Figure 4). The top 10 biological processes include xenobiotic metabolic process, signal transduction, estrogen metabolic process, cell surface receptor signaling pathway, positive regulation of gene expression, xenobiotic catabolic process, retinoic acid metabolic process, steroid metabolic process, positive regulation of protein kinase B signaling, and protein phosphorylation. The top 10 Cellular components include cytoplasm, plasma membrane, cytosol, endoplasmic reticulum membrane, intracellular membrane-bounded organelle, focal adhesion, ficolin-1-rich granule lumen, phosphatidylinositol 3-kinase complex, class IA, phosphatidylinositol 3-kinase complex, and basal plasma membrane. And moreover, the top 10 molecular functions include enzyme binding, ATP binding, protein serine/threonine/tyrosine kinase activity, heme binding, kinase activity, protein kinase activity, protein homodimerization activity, aromatase activity, monooxygenase activity, and pathways, endocrine resistance, lipid and atherosclerosis, cancer pathways, chemical carcinogenesis protein phosphatase binding. A total of 139 KEGG signaling pathways in diabetic complications, such as EGFR tyrosine kinase inhibitor resistance, metabolic- reactive oxygen species, and AGEs-RAGE signaling pathway, may be associated with the cardiovascularprotective effect of SGLT2 inhibitors (Figure 5). In order to create a pathways-targets network, In Cytoscape 3.10.1, the most significant Twenty enriched pathways were loaded (Figure 6). The output showed that the core 10 targets connected to the enriched pathways are PIK3CA, PIK3CD, MAPK1, MAPK3, GSTM1, EGFR, GSTP1, MAPK8, PIK3CB, and CASP3.
Molecular docking
First target in the PPI network and the first 3 core targets in the “pathway-Target” network PIK3CA, PIK3CD, MAPK1, and EGFR were docked to SGLT2Is molecularly. Based on the lowest binding affinity, we examined the stability of the docking configuration. More persistent compound-ligand binding and a higher likelihood of interaction are associated with lower binding affinities. Following (table 4) indicated all 36 docking results, from which the top 10 Protein-ligand Complexes were chosen for Visual analysis. Using Molegro-molecular viewer, we were able to acquire 3D representations of the hydrophobic pockets of the complex as well as 2D maps of the interactions (Figure 7).
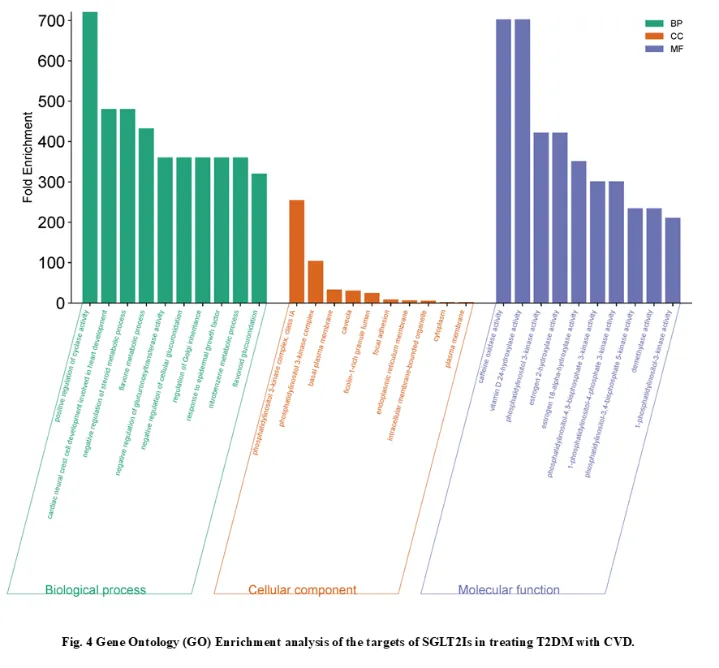
Figure 4 Gene Ontology (GO) Enrichment analysis of the targets of SGLT2Is in treating T2DM with CVD.
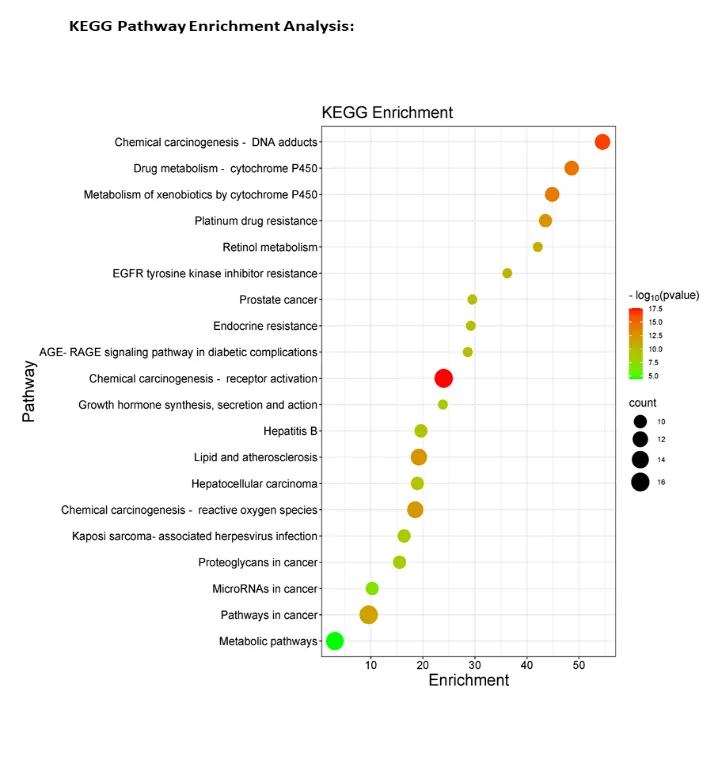
Figure 5 KEGG Pathway Enrichment analysis of the targets of SGLT2Is in treating T2DM with CVD.
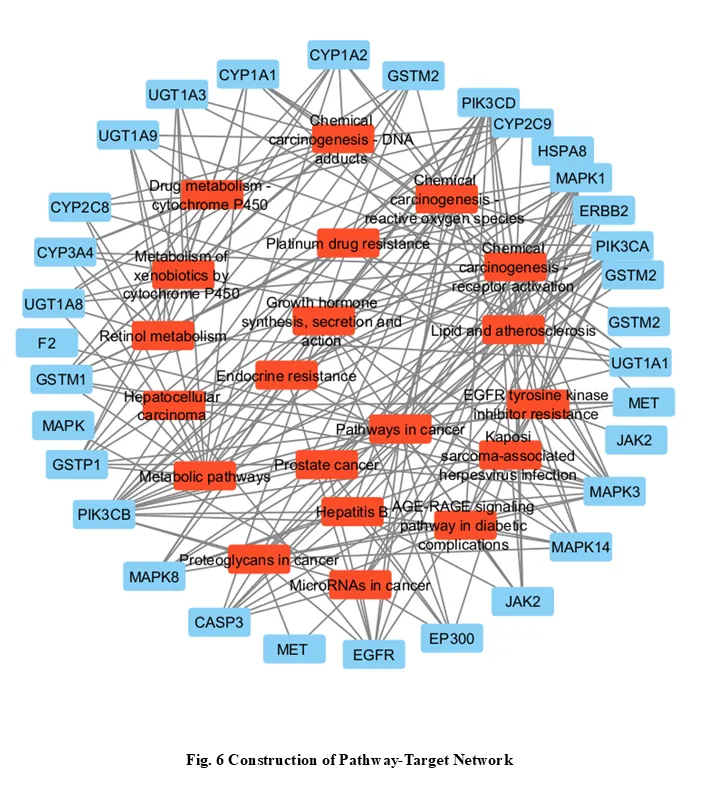
Figure 6 Construction of Pathway Target Network.
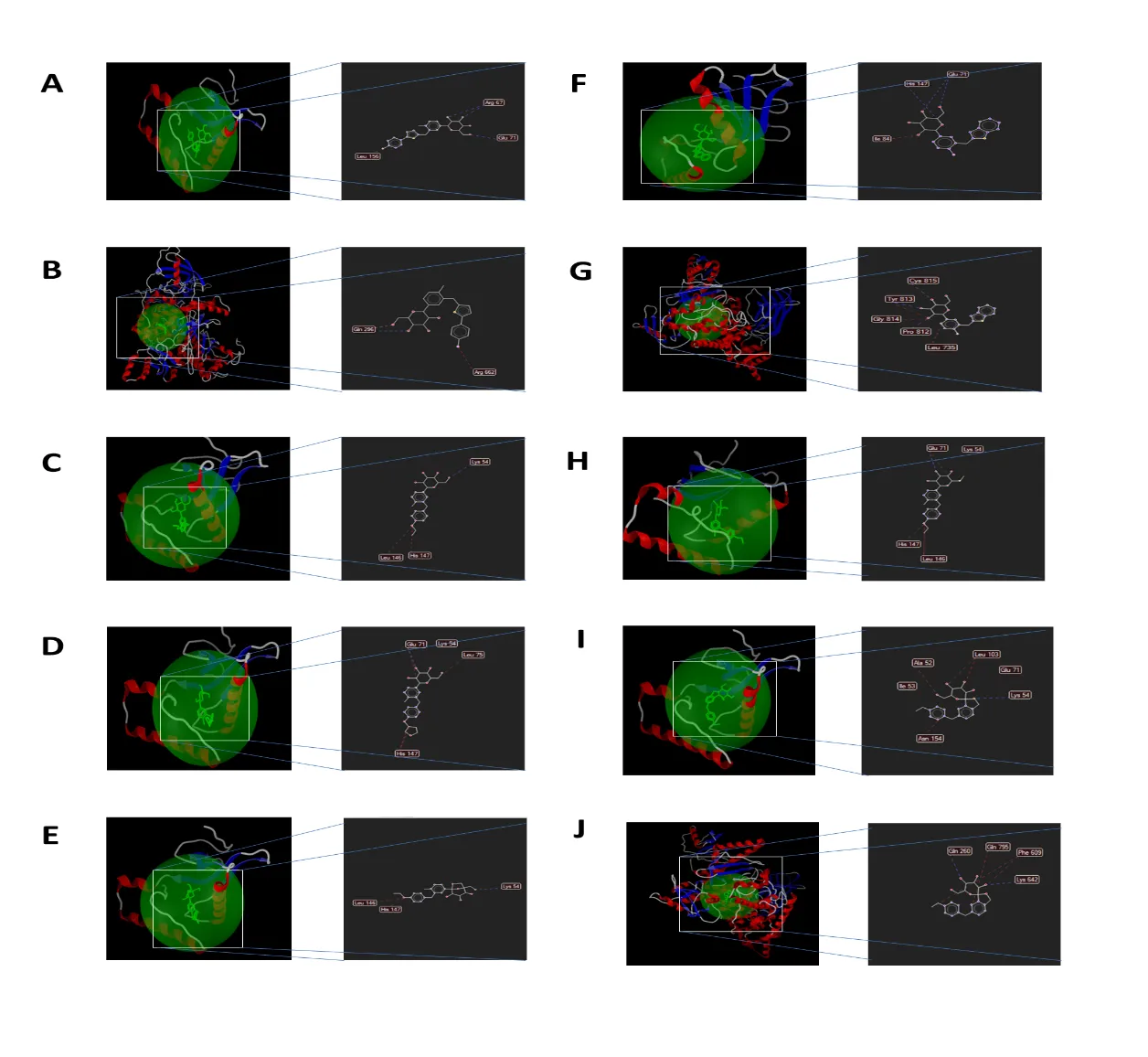
Figure 7 Molecular Docking study A) Ipragliflozin-MAPK1; B) Sotagliflozin-MAPK1; C) Canagliflozin-PIK3CA; D) Ipragliflozin-PIK3CD; E) Tofogliflozin-MAPK1; F) Canagliflozin-MAPK1; G) Ertugliflozin-MAPK1; H) Tofogliflozin-PIK3CD; I) Empagliflozin-MAPK1; J) Dapagliflozin-MAPK1.
|
SGLT2Is |
Pubchem ID |
Targets |
PDB ID |
Binding energy (kcal/mol) |
|
Bexagliflozin |
25195624 |
EGFR |
1M17 |
-2.78 |
|
MAPK1 |
1PME |
-4.22 |
||
|
PIK3CA |
3HHM |
-3.65 |
||
|
PIK3CD |
5DXU |
-2.65 |
||
|
Canagliflozin |
24812758 |
EGFR |
1M17 |
-3.86 |
|
MAPK1 |
1PME |
-5.35 |
||
|
PIK3CA |
3HHM |
-5.53 |
||
|
PIK3CD |
5DXU |
-4.34 |
||
|
Dapagliflozin |
9887712 |
EGFR |
1M17 |
-2.67 |
|
MAPK1 |
1PME |
-4.52 |
||
|
PIK3CA |
3HHM |
-3.33 |
||
|
PIK3CD |
5DXU |
-4.50 |
||
|
Empagliflozin |
11949646 |
EGFR |
1M17 |
-3.17 |
|
MAPK1 |
1PME |
-4.84 |
||
|
PIK3CA |
3HHM |
-3.96 |
||
|
PIK3CD |
5DXU |
-3.59 |
||
|
Ertugliflozin |
44814423 |
EGFR |
1M17 |
-2.58 |
|
MAPK1 |
1PME |
-4.97 |
||
|
PIK3CA |
3HHM |
-3.80 |
||
|
PIK3CD |
5DXU |
-3.88 |
||
|
Ipragliflozin |
10453870
|
EGFR |
1M17 |
-3.58 |
|
MAPK1 |
1PME |
-5.88 |
||
|
PIK3CA |
3HHM |
-4.33 |
||
|
PIK3CD |
5DXU |
-5.14 |
||
|
Luseogliflozin |
11988953
|
EGFR |
1M17 |
-2.65 |
|
MAPK1 |
1PME |
-4.20 |
||
|
PIK3CA |
3HHM |
-3.08 |
||
|
PIK3CD |
5DXU |
-2.95 |
||
|
Sotagliflozin |
24831714
|
EGFR |
1M17 |
-3.63 |
|
MAPK1 |
1PME |
-5.62 |
||
|
PIK3CA |
3HHM |
-3.65 |
||
|
PIK3CD |
5DXU |
-3.60 |
||
|
Tofogliflozin |
46908929
|
EGFR |
1M17 |
-4.52 |
|
MAPK1 |
1PME |
-5.26 |
||
|
PIK3CA |
3HHM |
-3.91 |
||
|
PIK3CD |
5DXU |
-4.88 |
Table 4 – Molecular docking findings of SGLT2Is
DISCUSSION:
Diabetes mellitus is a chronic metabolic disorder characterized by elevated blood glucose levels due to improper insulin synthesis or utilization by the body. Among the most concerning aspects of diabetes is its potential to result in cardiovascular disease (CVD). For those with diabetes, cardiovascular diseases such heart failure, stroke, and coronary artery disease are leading causes of death and disability. People with diabetes have a two to four times higher risk of developing CVD than people without the disease, according to numerous studies [3]. A lot of interest and attention was generated when it was discovered in clinical trials that SGLT2 inhibitors were useful in treating CVD in individuals with DM [14, 15]. However, the exact mechanism of SGLT2 inhibitors in the treatment of Diabetes induced CVD is still unknown. In this work, we investigated the SGLT2 inhibitor’s therapeutic mechanism in the treatment of T2DM complicated by CVD using the network pharmacology approach and molecular docking study. According to the combination of PPI network and Pathway-Target network, the top 4 core targets of SGLT2 inhibitors Mitogen-activated protein kinase 1 (MAPK1), Epidermal growth factor receptor (EGFR), Phosphatidylinositol-4,5-Bisphosphate 3-Kinase Catalytic Subunit Alpha (PIK3CA) and Phosphatidylinositol-4,5-Bisphosphate 3-Kinase Catalytic Subunit Delta (PIK3CD) acting on DM with HF and CAD were obtained. KEGG analysis was used to filter the key pathways, which mostly involved metabolic processes, lipid and atherosclerosis, chemical carcinogenesis - reactive oxygen species, AGE-RAGE signaling pathway in diabetic complications, and EGFR tyrosine kinase inhibitor resistance.
Among the top four key targets, the first, MAPK1, belongs to the MAPK protein family and is often referred to as ERK1(extracellular signal-regulated kinase 1) [29]. MAPKs are a class of serine/threonine protein kinases that, upon activation, phosphorylate a broad variety of downstream targets across several compartments to carry out highly specialized physiological responses [30]. Multiple biochemical signals can be integrated by MAPK, which is involved in many distinct cellular processes such as development, transcription regulation, differentiation, and proliferation. As a member of the MAPK family, cardiac hypertrophy and dysfunction have also been linked to ERK1 activation [31]. ERK 1 has been shown to have an impact on diabetes, as evidenced by the connection between dysregulated ERK 1 levels and dysregulation in a type 1 diabetic mice model [32]. Unlike empagliflozin or dapagliflozin, Canagliflozin inhibits ERK1/2 phosphorylation in lipopolysaccharide-stimulated human coronary artery endothelial cells, which lessens Hexokinase II expression and lowers inflammation [33]. This suggests that one of the possible targets in T2DM with HF and CAD is MAPK1. The next one is EGFR, the epidermal growth factor receptor is a protein on the cell surface that binds to the epidermal growth factor to control cell growth, proliferation, and survival. It also plays a role in atherogenesis, neointimal hyperplasia, blood pressure regulation, and reactive oxygen. Angiotensin II receptor type 1 (AT1) and EGFR receptors were hypothesized to be involved in the enhanced activity that led to this outcome.
According to Xu et al., the loss of plasmalemmal caveolae in mesenteric vascular smooth muscle cells may be connected to the increased myogenic constriction of the mesenteric artery in heart failure [34]. Resistance arterial dysfunction in type 2 diabetes was discovered to be influenced by increased EGFR phosphorylation by Belmadani et al [35]. This suggests that EGFR is another important target in DM with HF and CAD. Phosphoinositide 3-kinases (PI3Ks) are lipid kinases that create 3-phosphoinositides to regulate important intracellular signaling and vesicle trafficking functions. The final two genes in the top five core targets are PIK3CA and PIK3CD. Class I PI3Ks are mostly activated to catalyze PtdIns(4,5)P2 phosphorylation, which yields PtdIns(3,4,5)P3, in response to stimulation of cell surface receptors[36]. A catalytic component known as p110 is joined with a regulatory subunit to form these heterodimeric enzymes[37]. The isoform nomenclature for PI3Kα, β, δ, and γ is determined by the catalytic p110 subunit found in a Class I PI3K heterodimer; that is, p110α (PIK3CA gene), p110β (PIK3CB), p110δ (PIK3CD), or p110γ (PIK3CG) are present in each of these isoforms, respectively [36]. Thrombosis can result in acute myocardial infarction and sudden cardiac mortality in cases of coronary heart disease, which is frequently linked to atherosclerosis [38]. Though its involvement in platelet function is relatively minor, PI3Kα has been implicated in IGF1-mediated increase of platelet function, according to early investigations utilizing the PI3Kα selective inhibitor PIK75. Moreover, research on inhibitors revealed that PI3Kα may possibly be involved in Platelet glycoprotein VI GPVI-mediated platelet function [39-41]. Following that, two groups created a mouse model in which the megakaryocytic lineage's p110α had been selectively eliminated. researchers discovered that PI3Kα is the isoform that preserves platelet function, even though PI3Kβ and α both contribute to Insulin-like growth factor 1 IGF1-mediated Protein kinase B (AKT) phosphorylation. This was achieved by combining genetic and pharmacological techniques, such as cautious titration of PI3Kα and β inhibitors [42]. The processes of integrin αIIbβ3 activation and α-granule release mediated by PAR4, thrombin, CRP, and fucoidan, and thrombus formation on a collagen-coated surface under flow, were not affected [42]. On the other hand, p110α deletion, except PI3Kα inhibition, led to a synergistic augmentation of TPO mediated priming of platelet activity through increased phosphorylation of ERG1/2 and creation of TxA2. This suggests that PI3Kα has a unique negative regulatory role in platelet function that is independent of kinase. Additionally, research indicates that PI3Kα plays many functions in platelet function; inhibitors and PI3Kα deficiency reduce ADP release at low GPVI activation levels and impair platelet adhesion to vWF under shear. In addition to PI3Kβ, PI3Kα is involved in the platelet priming effect of anti-phospholipid antibodies [43,44]. More significantly, inhibition and deletion of PI3Kα reduced arterial thrombosis without affecting bleeding time, indicating that it may be a target for the treatment of CVD [44]. In both human and mouse platelets, the expression of the PI3Kδ isoform is small and has minimal effect on platelet function [45-47]. It is yet unknown how important PI3K inhibition is for myocardial infarction (MI). The significance of PI3K inhibition for myocardial infarction (MI) is still unclear. In animal models, the Class I PI3Kδ/γ inhibitor TG100-115 has been shown to provide cardio protection by reducing the formation of infarcts and maintaining myocardial function, even when administered up to three hours after cardiac infusion. This led to its entry into phase I and II clinical trials for acute MI [48]. According to published research, PI3K suppression may have cardioprotective and anti-thrombotic properties. Nevertheless, direct binding cannot be confirmed by our docking results for PIK3CA and PIK3CD “(-3.08 to -5.53 kcal/mol)”. Validation by experimentation is necessary.
In the enrichment of KEGG pathway, EGFR tyrosine kinase inhibitor resistance, AGE-RAGE signaling pathway in diabetic complications, Lipid and atherosclerosis and Metabolic pathways were found to be the significant pathways. The first KEGG pathway is EGFR tyrosine kinase inhibitor resistance. in 2005, the first in vivo publications that demonstrated a direct link between increased EGFR/ErbB1 signalling and vascular dysfunction brought on by diabetes.These reports indicated that pharmacological inhibition of this RTK corrected the pathology in the renal and carotid arteries, as well as the mesenteric vascular bed [49-51]. The first studies on vascular EGFR were carried out in rats with streptozotocin-induced type 1 diabetes, a preclinical model of the disease. The results of these studies were then repeated in the vasculature of animals with type 2 diabetes [35,52,53], indicating that dysregulated EGFR/ErbB1/HER1 signalling was a prevalent mediator of vascular issues in both T1 and T2DM.In rats that were spontaneously hypertensive, EGFR inhibition decreased the generation of reactive oxygen species in the left ventricle and decreased the size of the hypertensive myocarditis [54]. Consequently, there may be a shared effect of EGFR tyrosine kinase inhibitor resistance to quicken the progression of DM with CVD. The next one, Lipid and atherosclerosis (AS), the primary cause of cardiovascular disease (CVD) overall is atherosclerosis, an inflammatory illness. According to C-reactive protein (CRP), atherosclerosis is classified as an inflammatory disease with a high concentration of activated monocytes/macrophages and T lymphocytes in lesions [55-57]. The cells within the lesions generate significant quantities of cytokines, primarily proinflammatory ones [58,59]. Even though there are other factors contributing to the development of AS, DM is a well-known cause of AS [60]. The results of a comprehensive review and meta-analysis indicate that drugs that lower blood sugar, like SGLT2 inhibitors, can significantly minimize the risk of AS events [61]. Three distinct cell types are involved in the production of atherosclerotic plaques: monocytes/macrophages, vascular smooth muscle cells (VSMCs), and endothelial cells (ECs). Excessive lipids and lipoproteins build up in the subendothelial matrix during the first stage as a result of endothelial dysfunction. An accumulation of oxidized low-density lipoprotein (Ox-LDL) initiates this process by inducing the release of adhesion molecules such as monocyte chemoattractant protein 1 (MCP-1), macrophage colony-stimulating factor (M-CSF), intercellular cell adhesion molecule-1 (ICAM-1), and vascular cell adhesion protein 1 (VCAM-1). Subsequently, monocytes in circulation go towards the intima, where they multiply, undergo macrophage differentiation, and merge with lipoproteins to create foam cells. Tumour necrosis factor alpha (TNFα) and IL-1 are pro-inflammatory cytokines that are expressed by monocytes and macrophages. Pro-fibrosis chemicals can also be secreted by VSMCs that migrate out of the medial layer. Necrotic cores are formed when foam cells and SMCs die as a result of the ongoing migration of monocytes into the intima and the buildup of lipids and lipoproteins. Atherosclerotic plaques will eventually form when platelets clone to create thrombi. Acute cardiovascular and cerebrovascular events can arise from arterial blockage or plaque rupture [62-64]. Numerous metabolic traits, such as hypertension, dyslipidemia, obesity, and hyperglycemia, are independent risk factors for atherosclerosis [65]. These metabolic diseases contribute to the pathophysiology of atherosclerosis by promoting the production of plaques and oxidative stress, inflammation, endothelial dysfunction, and impaired autophagy [66]. The next one is the AGE-RAGE signaling pathway in diabetic complications; AGE-RAGE signaling is a well-researched cascade in diabetes mellitus. It has been discovered that vascular calcification in diabetes can be directly mediated by the AGE-RAGE signaling pathway. Furthermore, because the route causes oxidative stress, elevated inflammation, and heightened extracellular matrix buildup that results in diastolic and systolic dysfunction, it may potentially have an influence on diabetes consequences. When diabetes problems arise, activation of the AGE-RAGE signaling pathway may result in excessive generation of advanced glycation end products that harm cardiomyocytes and induce heart failure (HF), which, like outcomes of a different study's pathway analysis, suggests that the AGE-RAGE signaling pathway in diabetes complications may affect the onset of HF [67-69]. The next one is metabolic pathways, the heart always needs energy, and it uses a range of sources, including glucose and free fatty acids. The heart lacks sufficient energy sources due to poor glucose utilization in stress-related disorders such as T2DM and HF. Fatty acids and ketones offer an alternate energy source in this dire situation. The metabolism of these secondary energy stores gives the heart an increased supply of ATP [70-72]. Insulin-mediated glucose utilization is diminished in persons with type 2 diabetes. It is more dependable for free fatty acids (FFAs) to provide enough energy. Nevertheless, metabolizing FFAs requires more oxygen than metabolizing glucose [73]. Reduced heart metabolic efficiency and insufficient ATP generation are the results of this metabolic condition. Numerous investigations have demonstrated that SGLT-2 inhibitor therapy protects diabetic individuals by enhancing cardiac energy metabolism. β-hydroxybutyrate (βOHB) is a ketone that is promoted by empagliflozin. According to some research, βOHB might serve as a more affordable energy source and "super fuel" for those suffering from diabetic cardiovascular disease [74]. As previously discussed, when a person has diabetes and heart failure, glucose is no longer their main energy source. through encouraging the ketone body formation from energy sources, empagliflozin reverses cardiac remodelling and improves systolic function and myocardial energy metabolism. This improves poor cardiac remodelling in heart failure patients [75]. The administration of empagliflozin decreased ventricular preload and elevated plasma ketones in a diabetic db/db mouse model fed on a fasting diet. There is a positive correlation between myocardial ATP generation and elevated ketone levels [76]. Furthermore, ketone bodies are acknowledged as more than just a different kind of energy. Additionally, they can function as an inflammatory suppressant by blocking nucleotide-binding oligomerization domain-like receptor P3 (NLRP3) pathways. Contrasting results have been reported by other investigations, though. Empagliflozin alleviated heart failure symptoms in mice, however ketone bodies did not mediate this benefit, according to Verma et al. (2018). Rather, they saw more oxidation of traditional energy sources like glucose and fatty acids. This implies that SGLT2 inhibitors may have multifactorial and context-dependent metabolic effects [77,78]. In summary, our study methodically clarified the underlying molecular pathways by which SGLT2 inhibitors interfered with T2DM and CVD at the same time using network pharmacology and molecular docking. Thus, additional experimental results should be examined to attain the dependability of anticipated outcomes through both in vitro and in vivo methods.
Limitations: Instead of identifying causative pathways, network pharmacology finds connections. Binding energies below the usual threshold for high-confidence interactions (≤ -7.0 kcal/mol) were shown by the molecular docking data. As a result, these results should only be regarded as hypothesis-generating. Before any claim of direct target engagement can be made, experimental confirmation utilizing methods such cellular temperature shift assays, isothermal titration calorimetry, or surface plasmon resonance is necessary.
CONCLUSION
A network pharmacology analysis identified 27 possible SGLT2 inhibitor targets linked to coronary artery disease and heart failure associated with type 2 diabetes. With the exception of metabolic enzymes, the most promising candidate targets for additional validation are EGFR, MAPK1, PIK3CA, and PIK3CD. KEGG pathway analysis showed that lipid metabolism, atherosclerosis pathways, and AGE-RAGE signaling were all involved. Weak binding energies (-2.58 to -5.88 kcal/mol) were suggested by molecular docking, and direct target engagement must be confirmed through experimental validation. This study provides a hypothesis generating framework for future mechanistic investigations.
REFERENCES

Mohamed Sameer A.1*, Dhiyaneshwar A.1, Madhumitha S.1, Mohammed Kaif M.2, Mohamed Thoufik A.3, Selvi G.1, In Silico Identification of Cardioprotective Targets for SGLT2 Inhibitors in Type 2 Diabetes-Associated Heart Failure and Coronary Artery Disease, Int. J. Sci. R. Tech., 2026, 3 (6), 1484-1503. https://doi.org/10.5281/zenodo.20845996
 10.5281/zenodo.20845996
10.5281/zenodo.20845996