
We use cookies to ensure our website works properly and to personalise your experience. Cookies policy
1Gandhari College (School of Pharmacy), Garhbari, Nazirbazar, Bhutanathdham, Purba Medinipur, West Bengal, 721655.
2Pandaveswar School of Pharmacy, Near Coalfield College of Education (B.Ed), Pandaveswar - Raniganj Road, NH-14 (formerly NH-60), District - Paschim Bardhaman, West Bengal, India. Pin - 713346.
3Rangamati College of Pharmacy, Banior, Nalhati, Birbhum, West Bengal, 731243.
4Faculty of Medical Science and Research, Sai Nath University, Ranchi, Jharkhand-835219, India.
Prodrugs are inactive molecules that are metabolized to active drugs in the body. They are intended to address issues of poor solubility, low membrane permeability, rapid metabolism, and off-target toxicity. There has been considerable research on targeted prodrug systems that are activated at disease sites in recent years. This review highlights recent developments in prodrugs that are responsive to enzymes, pH-sensitive, hypoxia-activated, and receptor-targeted. We also explore nanoparticulate and antibody-drug conjugate (ADC) platforms that increase delivery accuracy. From the oncology field to infectious diseases and metabolic disorders, recent clinical approvals and running trials illustrate the increasing impact of prodrug strategies. While significant strides are being made, there are still hurdles to overcome in ensuring selectivity, complexity of manufacturing, and patient outcomes in different populations.
Bioavailability is a common reason for many promising drug candidates to be rejected from clinical development—not due to a lack of biological activity. Common barriers include poor solubility, enzymatic degradation, low cell membrane permeability, and non-specific distribution to healthy tissues. One of the strategies to resolve these problems is the prodrug approach [1].
A prodrug is an inactive compound that is metabolized to become an active compound in the body. Depending on the design, this transformation can occur under specific enzyme, pH level, redox, or light conditions. Many aspirin- and prontosil-like compounds have been in use for years, but today, prodrugs have undergone a significant leap in sophistication [2].
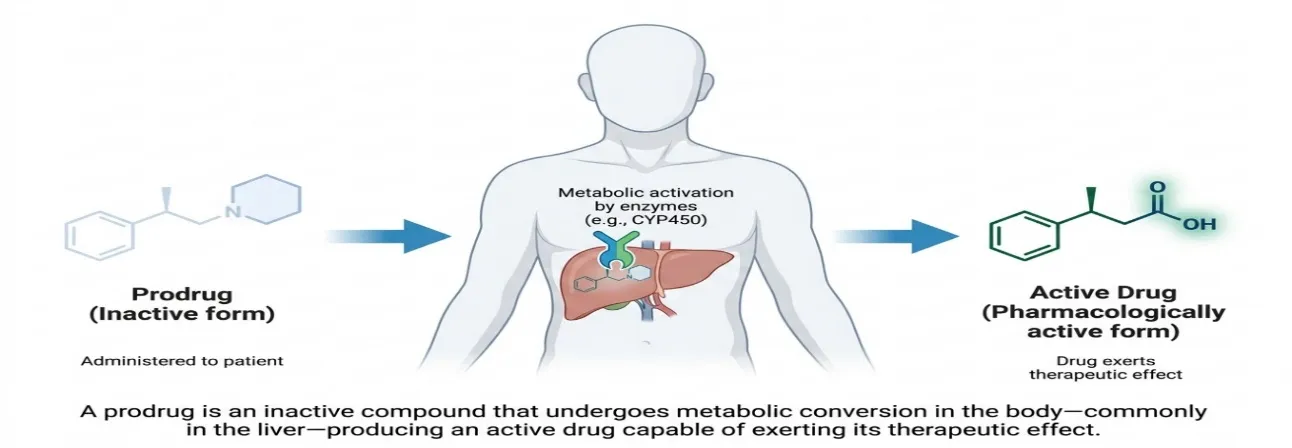
Fig 1: General concept of prodrug
The global prodrugs market has been growing significantly in the past few years due to the developments in molecular biology, structural chemistry, and nanotechnology. A significant proportion (approximately 10%) of all marketed drugs are prodrugs, and many new chemical entities currently undergoing clinical trials are formulated according to prodrug concepts [3]. This review aims to provide a concise overview of the current state of the art in prodrug design, specifically regarding targeted delivery systems, from 2018 to 2024.
2. CLASSIFICATION OF PRODRUGS
There are two types of prodrugs: Prodrugs that are activated within the cell (Type I) and prodrugs that are activated outside of the cell (Type II). Type I are prodrugs that utilize enzymes that are present in cells (e.g., cytochrome P450 enzymes or intracellular esterases). Type II prodrugs are activated in the gastrointestinal lumen, blood plasma, or tissue fluid [4].
These two can be further differentiated by whether the prodrug is activated by enzyme, pH, redox, receptor, or light. The following table summarizes the major classes and provides some examples.
|
Prodrug Type |
Activation Mechanism |
Example |
Target Site |
|
Type I (Intracellular) |
Enzymatic (cytochrome P450, esterase) |
Valacyclovir |
Intestinal epithelium / liver |
|
Type II (Extracellular) |
Enzymatic (alkaline phosphatase, protease) |
Fosamprenavir |
GI lumen / blood plasma |
|
Antibody-Drug Conjugates |
Lysosomal / protease cleavage |
Trastuzumab emtansine |
HER2+ tumor cells |
|
pH-sensitive |
Acid/base-triggered hydrolysis |
Omeprazole |
Gastric parietal cells |
|
Hypoxia-activated |
Reductive enzymes (NTR, DT-diaphorase) |
Tirapazamine |
Hypoxic tumor core |
|
Receptor-targeted |
Ligand-receptor binding + internalization |
Folate-drug conjugates |
Folate receptor+ tumors |
Table 1: Classification of prodrug types, their activation mechanisms, and target sites.
3. ENZYME-RESPONSIVE PRODRUGS
The most widespread triggers used in prodrug design are enzymes. Some tumors and infected tissues exhibit elevated levels of enzymes, which typically occur in low amounts in normal tissue. This differential expression can be applied to selectively activate a prodrug at the disease location [5].
3.1 Protease-Activated Prodrugs
The proteases, known as matrix metalloproteinases (MMPs) and cathepsins, are the proteases that are over-expressed in many solid cancers. Peptide linkers that are selectively cleaved by the enzymes have been engineered to make prodrugs from which the active drug is released at the site of the enzyme. For instance, there are legumain-cleavable prodrugs of doxorubicin that have demonstrated impressive tumor selectivity in preclinical studies [6].
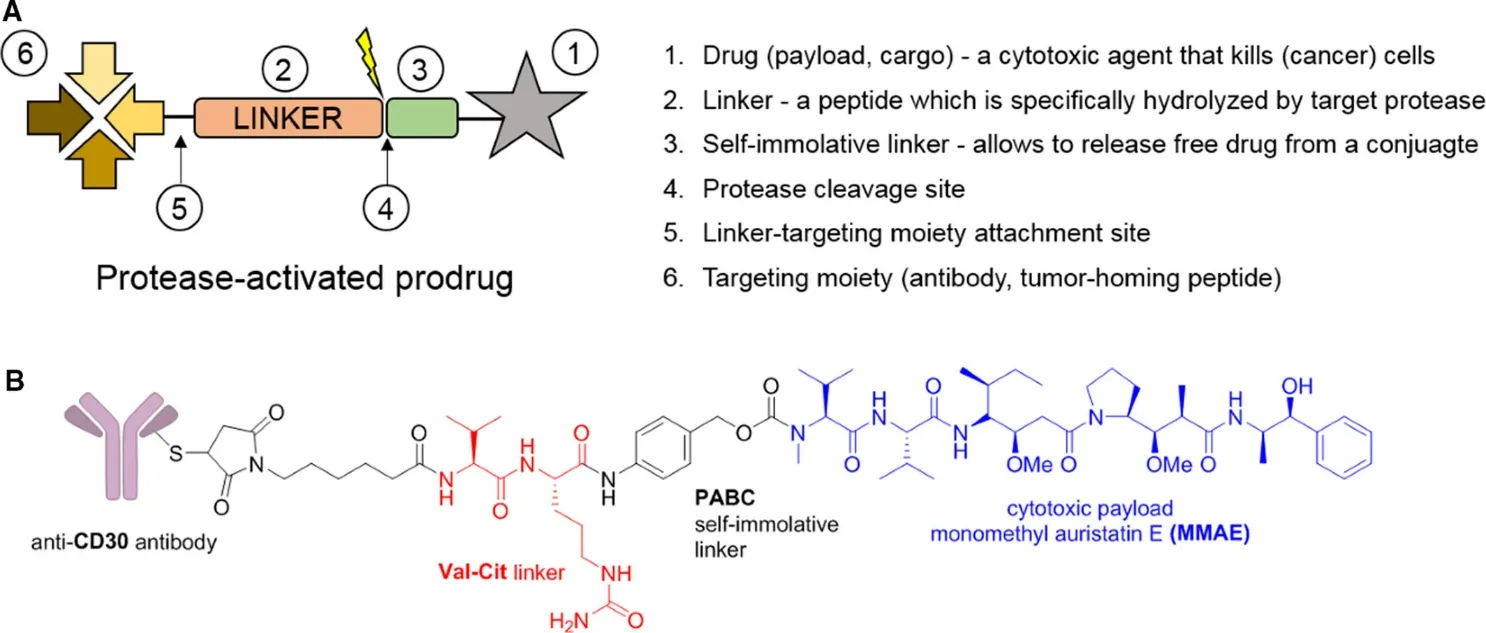
Fig 2: PAPs. Panel (A): PAPs' general framework. The targeting moiety, linker, and cytotoxic payload are the essential elements. The free payload is released when protease hydrolyzes peptide bonds. Panel (B) shows the structure of the protease-cleavable Ab–drug conjugate brentuximab vedotin, which is approved to treat relapsed systemic anaplastic large cell lymphoma and relapsed classical HL. The cytotoxic payload (MMAE) is indicated in blue, and the protease-cleavable linker (Val–Cit, VC) is indicated in red.
3.2 Phosphatase- and Glucuronidase-Activated Prodrugs
In certain cancers, such as osteosarcoma and colorectal cancer, alkaline phosphatase (ALP) is very active. Phosphate-masked prodrugs are converted to the active agent by ALP at the tumor site. Likewise, the accumulation of beta-glucuronosidase in necrotic tumor tissue has been exploited to mediate the release of a prodrug used for the treatment of cancer [7].
4. PH-SENSITIVE PRODRUGS
Tumors are generally more acidic (pH 6.5–6.9) compared with normal tissues (pH 7.4). This difference is due to the Warburg effect, the ability of cancer cells to metabolize through glycolysis even in the presence of oxygen, creating excess lactic acid [8].
This pH acidity is utilized by pH-sensitive prodrugs to release the drug. Hydrazones, acetals, and orthoester linkages are chemical bonds that are sensitive to acid. For example, doxorubicin hydrazone conjugates are not hydrolyzed at neutral pH, but rather hydrolyze very quickly at pH < 6.8, releasing the free drug in the tumor tissue [9].
Such systems can also be used in oral drug delivery. Drugs can be delivered to the intestine, where they are released once the pH of the gastrointestinal tract becomes alkaline, by using enteric-coated or pH-responsive prodrugs. The approach has been used for some medications, such as mesalazine, in inflammatory bowel disease [10].
5. HYPOXIA-ACTIVATED PRODRUGS
Often poor blood vessel development creates areas of very low oxygen concentration (hypoxia) within solid tumors. There is an association between hypoxia and conventional therapy resistance and poor prognosis. It also offers a novel activation platform for a prodrug [11].
Hypoxia-activated prodrugs (HAPs) are electron-accepting groups, e.g., nitro groups, N-oxide, or quinone groups that are reduced to electron-donating groups by reducing enzymes, e.g., nitroreductase or DT-diaphorase, under hypoxic conditions. Evofosfamide (TH-302) is a well-studied HAP that is activated in the hypoxic areas of a tumor by releasing a DNA alkylating agent [12].
Although they were initially promising, a number of HAPs have failed in large clinical trials, in part due to the heterogeneity of hypoxia in tumors. Current research continues to determine how to combine HAPs with anti-angiogenic agents that would exacerbate hypoxia, thus making it more selective [13].
6. RECEPTOR-TARGETED PRODRUG SYSTEMS
Receptor-targeted prodrugs deliver a prodrug to cells expressing a specific receptor via a specific ligand (e.g., folate, transferrin, glucose) or monoclonal antibody. Once bound, the complex is taken into the cell, and the active drug is released within the cell [14].
6.1 Folate-Receptor Targeting
Many types of cancer cells such as ovarian, lung and cervical cancers over-express folate receptor (FR) on their surface. This overexpression of folate receptors is used to target drugs specifically to tumor cells by the use of folate-drug conjugates. Vintafolide is a clinical-stage folate-receptor-targeted prodrug for therapeutic use in the treatment of cancer [15].
6.2 Antibody-Drug Conjugates (ADCs)
The class of targeted prodrugs is growing and is known as ADCs. They are composed of a monoclonal antibody with a potent cytotoxic drug attached by a cleavable linker. The antibody targets the specific surface antigen of cells to deliver the drug. Once inside the cell, the drugs released from the phagosomales are degraded by the content of the lysosomal enzymes, releasing the active drugs [16].
The FDA has approved a number of new ADCs since 2019: enfortumab vedotin, trastuzumab deruxtecan, and sacituzumab govitecan. In DESTINY-Breast03, trastuzumab deruxtecan (T-DXd) demonstrated an overall response rate of more than 60% in patients with HER2+ breast cancer [17].
7. NANOPARTICLE-BASED PRODRUG SYSTEMS
The use of prodrugs is a potent approach for the enhancement of systemically delivered nanoparticulate formulations. The enhanced permeability and retention (EPR) effect allows nanoparticles to accumulate in tumors and offers protection from early degradation as well as increasing circulation times of the prodrug [18].
Several types of lipid nanoparticles (LNPs), polymeric micelles, dendrimers, and mesoporous silica nanoparticles (MSNs) have been investigated as prodrug carriers. This drug has been used in one study that found a camptothecin prodrug loaded into self-assembling amphiphilic nanoparticles to be 5-fold more tumor-specific than the free drug in a mouse xenograft study [19].
There are further advantages for using polymer-prodrug conjugates since the drug is covalently attached to a biodegradable polymer backbone, such as the sustained release and the reduced burst effect. One of the most investigated systems in this group is the poly(ethylene glycol)-drug conjugate (PEGylated prodrug) [20].
8. RECENT CLINICAL APPROVALS AND ONGOING TRIALS
Table 2 highlights selected prodrugs with recent FDA approvals or strong clinical evidence. These examples span several therapeutic areas and demonstrate the breadth of prodrug applications.
|
Prodrug |
Active Drug |
Disease Indication |
Approval / Stage |
|
Sacituzumab govitecan |
SN-38 (irinotecan metabolite) |
Triple-negative breast cancer |
FDA approved 2020 |
|
Enfortumab vedotin |
Monomethyl auristatin E |
Urothelial carcinoma |
FDA approved 2019 |
|
Enalapril |
Enalaprilat |
Hypertension / heart failure |
Established clinical use |
|
Sofosbuvir |
GS-461203 (nucleoside) |
Hepatitis C virus |
FDA approved 2013 |
|
Capecitabine |
5-Fluorouracil |
Colorectal / breast cancer |
FDA approved 1998 |
Table 2: Selected clinically relevant prodrugs with recent approvals and therapeutic indications.
Sofosbuvir is a phosphoramidate prodrug of a nucleoside analog that is activated in the hepatocytes without being phosphorylated in the systemic circulation as in the case of the active form. It revolutionized hepatitis C treatment and got cure rates of over 95% [21].
Capecitabine is an anticancer agent that is selectively converted to 5-fluorouracil in tumor tissues but not in normal tissues, due to the differential expression of thymidine phosphorylase (TP) in these tissues. Capecitabine has a more favorable toxicity profile since the tumor-selective activation [22].
9. COMPARISON OF DELIVERY STRATEGIES
|
Strategy |
Advantages |
Limitations |
|
Nanoparticle-prodrug |
EPR effect; sustained release |
Batch variability; regulatory complexity |
|
ADC (Antibody-Drug Conjugate) |
High target selectivity; potent cytotoxicity |
High manufacturing cost; antigen heterogeneity |
|
Polymer-prodrug |
Long circulation; tunable release |
Incomplete drug release; immunogenicity risk |
|
Enzyme-responsive |
Precise tumor activation |
Enzyme expression variability across patients |
|
pH-responsive |
Simple design; oral delivery compatibility |
Non-specific activation in acidic healthy tissue |
Table 3: Comparative overview of major prodrug delivery strategies and their advantages and limitations.
10. CHALLENGES AND FUTURE DIRECTIONS
Although there have been significant advances, there are still significant hurdles in the way of the development of prodrugs. The first and most important is to be sure of selective activation. But if the activating enzyme or condition is too nonspecific in its action, it will activate in normal tissue, causing toxicity. This is further complicated by interpatient variability of enzyme expression [23].
Scaling up of the nanoparticle-prodrug system from lab to clinical production is significant. The batch-to-batch consistency, sterility, and shelf stability must be shown prior to regulatory approval [24].
The problem for ADCs is antigen heterogeneity, meaning that the antigen is not always expressed on all of the cells in a tumor. This may result in some tumor cells remaining undestroyed. In part this is overcome by bystander effects, whereby the released drug diffuses to neighboring antigen-negative cells and extends off-target toxicity [25].
Dual-trigger prodrugs: Future directions include the development of dual-trigger prodrugs that require two signals simultaneously (e.g. low pH AND elevated protease activity) which could significantly enhance the selectivity. Light activated prodrugs (photoactivatable prodrugs) are also under investigation for superficial tumours and local infections [26].
AI/ML has been used to predict the metabolism of prodrugs, optimize the linker chemistry, and discover new pairs of enzymes and substrates. The tools could potentially greatly speed up the rational design of next-generation prodrug systems [27].
CONCLUSION
Prodrug design has evolved from an idea to a complex, multi-disciplinary area of drug design. The rapid developments in enzyme biology, materials science, and immunology have enabled the development of highly targeted prodrug systems that can be selectively activated at disease sites. The recent clinical approvals, especially within the ADC area, support the therapeutic worth of these approaches.
The quest for selectivity, manufacturing, and patient-to-patient variability still needs to be tackled and will require ongoing collaboration between chemists, biologists, and clinicians. As investment in this field continues to increase and computational tools are being integrated, prodrug-based therapies will no doubt be a larger part of precision medicine in the next decade.
REFERENCES





Suvasish Mitra1, Soumita Das2, Ishita De1, Arpan Bera3, Deep Jyoti Shah4*, Recent Advances In Prodrug Design For Targeted Drug Delivery, Int. J. Sci. R. Tech., 2026, 3 (7), 1854-1860. https://doi.org/10.5281/zenodo.21103836
 10.5281/zenodo.21103836
10.5281/zenodo.21103836